Cardiovascular System - Abnormalities: Difference between revisions
mNo edit summary |
mNo edit summary |
||
| Line 78: | Line 78: | ||
{{Anderson2016 table2}} | {{Anderson2016 table2}} | ||
===Sex Ratios=== | |||
{{USA 1997-2009 Abnormalities Sex Ratio table}} | |||
===Ventricular Septal Defect=== | ===Ventricular Septal Defect=== | ||
Revision as of 05:52, 26 May 2018
| Embryology - 23 Jun 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Introduction
Heart defects and preterm birth are the most common causes of neonatal and infant death. The long-term development of the heart combined with extensive remodelling and post-natal changes in circulation lead to an abundance of abnormalities associated with this system. A good recent review of cardiac abnormalities is available online.[1]
A UK study literature showed that preterm infants have more than twice as many cardiovascular malformations (5.1 / 1000 term infants and 12.5 / 1000 preterm infants) as do infants born at term and that 16% of all infants with cardiovascular malformations are preterm. (0.4% of live births occur at greater than 28 weeks of gestation, 0.9% at 28 to 31 weeks, and 6% at 32 to 36 weeks. Overall, 7.3% of live-born infants are preterm)[2]
"Baltimore-Washington Infant Study data on live-born cases and controls (1981-1989) was reanalyzed for potential environmental and genetic risk-factor associations in complete atrioventricular septal defects AVSD (n = 213), with separate comparisons to the atrial (n = 75) and the ventricular (n = 32) forms of partial AVSD. ...Maternal diabetes constituted a potentially preventable risk factor for the most severe, complete form of AVSD."[3]
In addition, there are in several congenital abnormalities that exist in adults (bicuspid aortic valve, mitral valve prolapse, and partial anomalous pulmonary venous connection) which may not be clinically recognized.
Developmental abnormalities of the cardiovascular system are classified under ICD-10 as "Congenital malformations of the circulatory system (Q20-Q28)". Note that the updated release of this coding system (ICD-11) will include a coding based upon the International Pediatric Cardiac Code.[4][5]
Some Recent Findings
|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Cardiovascular Abnormality <pubmed limit=5>Cardiovascular Abnormality</pubmed> |
International Classification of Diseases
The International Classification of Diseases (ICD) World Health Organization's classification used worldwide as the standard diagnostic tool for epidemiology, health management and clinical purposes. This includes the analysis of the general health situation of population groups. It is used to monitor the incidence and prevalence of diseases and other health problems.
ICD11
| ICD-11 Structural developmental anomalies of the circulatory system (draft) |
|---|
| ICD-11 Beta Draft - NOT FINAL, updated on a daily basis, It is not approved by WHO, NOT TO BE USED for CODING except for agreed FIELD TRIALS.
20 Developmental Anomalies - Structural Developmental Anomalies Beta coding and tree structure for "structural developmental anomalies" within this section are shown in the table below. |
| Structural developmental anomalies of the circulatory system |
|
| CD-11 Beta Draft - NOT FINAL, updated on a daily basis, It is not approved by WHO, NOT TO BE USED for CODING except for agreed FIELD TRIALS.
|
ICD10
Within the ICD10 classification "congenital malformations, deformations and chromosomal abnormalities" are (Q00-Q99) but excludes "inborn errors of metabolism" (E70-E90).
Congenital malformations of the circulatory system (Q20-Q28) can be viewed in the collapsed table below. Note that the updated release of this coding system (ICD-11) will include a coding based upon the International Paediatric and Congenital Cardiac Code International Pediatric Cardiac Code. This system was initiated in 2005 by the International Society for Nomenclature of Paediatric and Congenital Heart Disease (ISNPCHD).[4][5]
| ICD10 Congenital malformations of the circulatory system (Q20-Q28) |
|---|
| Cardiovascular System - Abnormalities |
| Q20 Congenital malformations of cardiac chambers and connections
Excl.: dextrocardia with situs inversus (Q89.3) mirror-image atrial arrangement with situs inversus (Q89.3)
|
| Q21 Congenital malformations of cardiac septa
Excl.: acquired cardiac septal defect (I51.0)
|
Q22 Congenital malformations of pulmonary and tricuspid valves
|
Q23 Congenital malformations of aortic and mitral valves
|
| Q24 Other congenital malformations of heart
Excl.: endocardial fibroelastosis (I42.4)
|
Q25 Congenital malformations of great arteries
|
Q26 Congenital malformations of great veins
|
| Q27 Other congenital malformations of peripheral vascular system
Excl.: anomalies of: cerebral and precerebral vessels (Q28.0-Q28.3) coronary vessels (Q24.5) pulmonary artery (Q25.5-Q25.7) congenital retinal aneurysm (Q14.1) haemangioma and lymphangioma (D18.-)
|
| Q28 Other congenital malformations of circulatory system
Excl.: congenital aneurysm: NOS (Q27.8) coronary (Q24.5) peripheral (Q27.8) pulmonary (Q25.7) retinal (Q14.1) ruptured: cerebral arteriovenous malformation (I60.8) malformation of precerebral vessels (I72.-)
|
| ICD-10 |
See also ICD-10 Chapter XVI Certain conditions originating in the perinatal period (P00-P96) P29 Cardiovascular disorders originating in the perinatal period.
Excl.: congenital malformations of the circulatory system (Q20-Q28)
- P29.0 Neonatal cardiac failure
- P29.1 Neonatal cardiac dysrhythmia
- P29.2 Neonatal hypertension
- P29.3 Persistent fetal circulation Delayed closure of ductus arteriosus Pulmonary hypertension of newborn (persistent)
- P29.4 Transient myocardial ischaemia of newborn
- P29.8 Other cardiovascular disorders originating in the perinatal period
- P29.9 Cardiovascular disorder originating in the perinatal period, unspecified
- Links: Neonatal Development | International Society for Nomenclature of Paediatric and Congenital Heart Disease (ISNPCHD)
Heart Abnormalities
Critical Periods
| Lesion | Start of Susceptibility to Malformation |
End of Susceptibility to Malformation | |||
|---|---|---|---|---|---|
| Interatrial communications | |||||
| Oval fossa defect | 6 weeks (E13.5) | Term | |||
| Sinus venosus defect | 8 weeks | 12 weeks | |||
| Coronary sinus defect | 8 weeks | Term | |||
| Vestibular defect | 7 weeks | 8 weeks | |||
| Ventricular Septal Defect | |||||
| Muscular | 8 weeks | Difficult to predict | |||
| Perimembranous | 6 weeks | 8 weeks | |||
| Doubly committed | 7 weeks | 8 weeks | |||
| Atrioventricular Septal Defect | |||||
| Ostium primum | 5 weeks | 6 weeks | |||
| “Complete” | 5 weeks | 6 weeks | |||
| Aortic coarctation | |||||
| With VSD | 5 weeks | 8 weeks | |||
| With intact ventricular septum | 8 weeks | Term | |||
| Double Outlet Right Ventricle | 6 weeks | 8 weeks | |||
| Transposition of Great Arteries | 6 weeks | 8 weeks | |||
| Ebstein’s malformation | 6 weeks | 8 weeks | |||
| Hypoplastic left heart syndrome | |||||
| With mitral atresia | 5 weeks | 8 weeks | |||
| With mitral stenosis | 8 weeks | Term | |||
| Pulmonary atresia | |||||
| With VSD | 6 weeks | 8 weeks | |||
| With intact ventricular septum | 8 weeks | Term | |||
| Other | |||||
| Functionally single ventricle | 5 weeks | 6 weeks | |||
| Tetralogy of Fallot | 7 weeks | 8 weeks | |||
| Totally anomalous pulmonary venous return | 8 weeks | 12 weeks | |||
| Tricuspid atresia | 5 weeks | 6 weeks | |||
| Common arterial trunk | 5 weeks | 7 weeks | |||
| Bicuspid aortic valve | 6 weeks | Term | |||
| Notes | |||||
| For approximate clinical Gestational Age GA add 2 weeks; number in brackets is mouse equivalent. Data Reference[1] | Links: heart | abnormal development | timeline | Category:Timeline | ||||
| Table 2. Summary of Timing (Post Fertilization) of Cardiac Susceptibility to a Drug-Induced Malformation | ||
|---|---|---|
| Lesion | Start of Susceptibility to Malformation |
End of Susceptibility to Malformation |
| Interatrial communications | ||
| Oval fossa defect | 6 weeks (E13.5) | Term |
| Sinus venosus defect | 8 weeks | 12 weeks |
| Coronary sinus defect | 8 weeks | Term |
| Vestibular defect | 7 weeks | 8 weeks |
| Ventricular Septal Defect | ||
| Muscular | 8 weeks | Difficult to predict |
| Perimembranous | 6 weeks | 8 weeks |
| Doubly committed | 7 weeks | 8 weeks |
| Atrioventricular Septal Defect | ||
| Ostium primum | 5 weeks | 6 weeks |
| “Complete” | 5 weeks | 6 weeks |
| Aortic coarctation | ||
| With VSD | 5 weeks | 8 weeks |
| With intact ventricular septum | 8 weeks | Term |
| Double Outlet Right Ventricle | 6 weeks | 8 weeks |
| Transposition of Great Arteries | 6 weeks | 8 weeks |
| Ebstein’s malformation | 6 weeks | 8 weeks |
| Hypoplastic left heart syndrome | ||
| With mitral atresia | 5 weeks | 8 weeks |
| With mitral stenosis | 8 weeks | Term |
| Pulmonary atresia | ||
| With VSD | 6 weeks | 8 weeks |
| With intact ventricular septum | 8 weeks | Term |
| Other | ||
| Functionally single ventricle | 5 weeks | 6 weeks |
| Tetralogy of Fallot | 7 weeks | 8 weeks |
| Totally anomalous pulmonary venous return | 8 weeks | 12 weeks |
| Tricuspid atresia | 5 weeks | 6 weeks |
| Common arterial trunk | 5 weeks | 7 weeks |
| Bicuspid aortic valve | 6 weeks | Term |
|
Notes: For approximate clinical Gestational Age GA add 2 weeks; number in brackets is mouse equivalent. Reference: Anderson RH. Teratogenecity in the setting of cardiac development and maldevelopment. (2016) | ||
Sex Ratios
| Male preponderance | Female preponderance |
|---|---|
|
|
| Cardiac defects | |
|
|
| Table data[11] Links: abnormal development | cardiovascular abnormalities | USA | Male | Female | cleft lip and palate | |
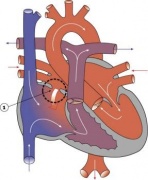
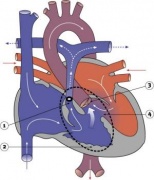
Ventricular Septal Defect

|
The Ventricular Septal Defect (VSD) usually occurs in the membranous (perimembranous) rather than muscular interventricular septum, and is more frequent in males that females.
Perimembranous defects are located close to the aortic and tricuspid valves and adjacent to atrioventricular conduction bundle. ICD-10 Q21.0 Ventricular septal defect
|
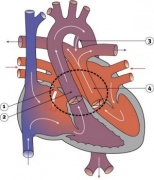
Atrial Septal Defects

|
Atrial Septal Defects (ASD) are a group of common (1% of cardiac) congenital anomolies defects occuring in a number of different forms and more often in females.
ICD-10 Q21.1 Atrial septal defect Coronary sinus defect Patent or persistent: foramen ovale ostium secundum defect (type II) Sinus venosus defect Treatment: The surgical repair requires a cardiopulmonary bypass and is recommended in most cases of ostium secundum ASD, even though there is a significant risk involved. Ostium primum defects tend to present earlier and are often associated with endocardial cushion defects and defective mitral or tricuspid valves. In such cases, valve replacement may be necessary and the extended operation has a considerable chance of mortality.
|
Patent Ductus Arteriosus

|
Patent ductus arteriosus (PDA), or Patent arterial duct (PAD), or common truncus, occurs commonly in preterm infants, and at approximately 1 in 2000 full term infants and more common in females (to male ratio is 2:1). Can also be associated with specific genetic defects, trisomy 21 and trisomy 18, and the Rubinstein-Taybi and CHARGE syndromes. The opening is asymptomatic when the duct is small and can close spontaneously (by day three in 60% of normal term neonates), the remainder are ligated simply and with little risk, with transcatheter closure of the duct generally indicated in older children. The operation is always recommended even in the absence of cardiac failure and can often be deferred until early childhood.
ICD-10 Q25.0 Patent ductus arteriosus Patent ductus Botallo Persistent ductus arteriosus
|



Tetralogy of Fallot

|
Named after Etienne-Louis Arthur Fallot (1888) who described it as "la maladie blue" and is a common developmental cardiac defect. The syndrome consists of a number of a number of cardiac defects possibly stemming from abnormal neural crest migration.
ICD-10 Q21.3 Tetralogy of Fallot Ventricular septal defect with pulmonary stenosis or atresia, dextroposition of aorta and hypertrophy of right ventricle.
|
Hypoplastic Left Heart

|
Characterized by hypoplasia (underdevelopment or absence) of the left ventricle obstructive valvular and vascular lesion of the left side of the heart.
ICD-10 Q23.4 Hypoplastic left heart syndrome Atresia, or marked hypoplasia of aortic orifice or valve, with hypoplasia of ascending aorta and defective develop-ment of left ventricle (with mitral valve stenosis or atresia).
|
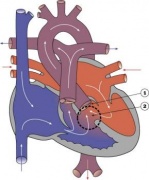
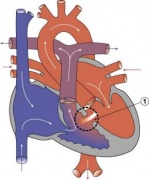
Double Outlet Right Ventricle

|
De-oxygenated blood enters the aorta from the right ventricle and is returned to the body. ICD-10 Q20.1 Double outlet right ventricle Taussig-Bing syndrome |
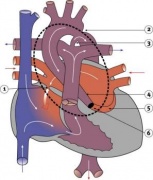
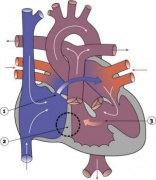
Tricuspid Atresia

|
Blood is shunted through an atrial septal defect to the left atrium and through the ventricular septal defect to the pulmonary artery. The shaded arrows indicate mixing of the blood.
ICD-10 Q22.4 Congenital tricuspid stenosis Tricuspid atresia Fontan Procedure: a surgical procedure developed by Fontan and Baudet (1971) to restore a circulation in patients with tricuspid atresia.
|
Dextrocardia

|

|
| Dextrocardia anatomical heart position[13] | Dextrocardia (postnatal 1 year old)[13] |
Initial malrotation of the heart tube bending left instead of right. Results in heart and greater vessels reversed. Can also occur with situs invertus, where viscera are transposed LR.
Anatomical left-right normal asymmetry is called situs solitus. The alternative heterotaxy can be either randomization (situs ambiguus) or a complete reversal (situs inversus) of normal organ position.
Abnormalities of Conducting System

Also variously called the cardiac conduction system (CCS), cardiac pacemaking and conduction system (CPCS), or atrioventricular conduction system (AVCS). Recently animal models (CCS-lacZ transgenic mouse) have helped identify key processes in the development of this specialized conduction system.
"Known arrhythmogenic areas including Bachmann's bundle, the pulmonary veins, and sinus venosus derived internodal structures, demonstrate lacZ expression." (Jongbloed et al, 2004)
Long QT Syndrome
Congenital long QT syndrome (LQTS) is a group of rare genetic disorders with prolonged ventricular repolarization and a risk of ventricular tachyarrhythmias. Cause is mutations in genes encoding either cardiac ion channels or channel interacting proteins.
Search NCBI Bookshelf: Congenital long-QT syndrome
- Links: Search PubMed
Heart Vessel Abnormalities
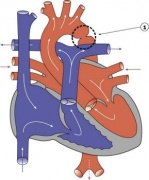
Transposition of the Great Vessels

|
Characterized by aorta arising from right ventricle and pulmonary artery from the left ventricle and often associated with other cardiac abnormalities (e.g. ventricular septal defect).
|
{kind=link}
Coarctation of the Aorta

|
|
Interrupted Aortic Arch
- LInks: Search PubMed
Pulmonary Atresia

|
|
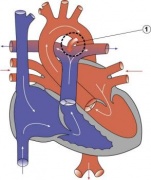
Total Anomalous Pulmonary Venous Connection

|
Total Anomalous Pulmonary Venous Connection (TAPVC) or Total Anomalous Pulmonary Venous Return (TAPVR) occurs when pulmonary veins connect to the right atrium (RA) and not the left atrium (LA). This abnormal connection returns oxygenated pulmonary blood from the lungs back to the right atrium or a vein flowing into the right atrium.
|
Complete Atrioventricular Canal

|
|
Partial Anomalous Pulmonary Venous Drainage

|
|
Aortic Stenosis

|
|
Pulmonary Stenosis

|
ICD-10 Q25.6 Stenosis of pulmonary artery Supravalvular pulmonary stenosis
|
Hypertrophic Cardiomyopathy
Hypertrophic cardiomyopathy (HCM) is a postnatal cardiac abnormality with left ventricular hypertrophy following pre-hypertrophic crypts, abnormal mitral leaflets and trabeculae. This heart anomaly is due to mutations in the sarcomeric protein genes, most commonly myosin-binding protein C (MYBPC3).
Blood Disorders
Sickle Cell Anemia
| People who have this form of sickle cell disease inherit two sickle cell genes (“S”), one from each parent. This is commonly called “sickle cell anemia”, and is usually the most severe form of the disease. The name comes from the "sickle" shape of the RBC compared to the normal "donut" shape.
|

Sickle cell RBC (Image CDC) |
Thalassemia
Thalassemia is a group of inherited (genetic) blood disorders most frequently in people of Italian, Greek, Middle Eastern, Southern Asian and African Ancestry. The most severe form of alpha thalassemia, affecting mainly people of Southeast Asian, Chinese and Filipino ancestry, results in fetal or newborn death.
The two main types of thalassemia are called "alpha" and "beta," depending on which part of an oxygen-carrying protein in the red blood cells is lacking. Both types of thalassemia are inherited in the same manner. A child who inherits one mutated gene is a carrier, which is sometimes called "thalassemia trait." Most carriers lead completely normal, healthy lives.
Statistics
Australia

Data shown as a percentage of all major abnormalities based upon published statistics using the same groupings as Congenital Malformations Australia 1981-1992 P. Lancaster and E. Pedisich ISSN 1321-8352.
Belgium
Congenital heart disease in 111 225 births in Belgium 2008 study[15]:
- 921 children with congenital heart disease (birth prevalence of 8.3 per 1000).
- 33% ventricular septal defects most frequently occurring condition
- 18% ostium secundum atrial septal defects
- 10% pulmonary valve abnormalities
- 39% had either cardiosurgical operation or catheter intervention.
- 4% of the children died (higher in univentricular physiology, pulmonary atresia with VSD, left ventricle outflow obstruction and tetralogy of Fallot).
South America
Paediatric and congenital heart disease in South America: an overview.[16]
- Ventricular septal defects - Surgical mortality with repair in infancy, mainly in the muscular septum, probably slightly higher in South America than in North America and Europe.
- Secundum atrial septal defects - trans-catheter closure is the preferred method of treating most patients.
- Pulmonary valve stenosis and atresia with intact ventricular septum - balloon pulmonary valvuloplasty for PVS.
- Aortic stenosis - balloon valvuloplasty.
- Coarctation of the aorta - children balloon angioplasty, adolescents and adults a trend towards the use of bare and covered stents.
- Tetralogy of Fallot - patients with severe hypoxaemia have a modified Blalock–Taussig shunt.
USA
"Baltimore-Washington Infant Study data on live-born cases and controls (1981-1989) was reanalyzed for potential environmental and genetic risk-factor associations in complete atrioventricular septal defects AVSD (n = 213), with separate comparisons to the atrial (n = 75) and the ventricular (n = 32) forms of partial AVSD. ...Maternal diabetes constituted a potentially preventable risk factor for the most severe, complete form of AVSD."[3]
((USA 1997-2009 Abnormalities Sex Ratio table}}
References
- ↑ 1.0 1.1 Anderson RH. Teratogenecity in the setting of cardiac development and maldevelopment. (2016)
- ↑ Tanner K, Sabrine N & Wren C. (2005). Cardiovascular malformations among preterm infants. Pediatrics , 116, e833-8. PMID: 16322141 DOI.
- ↑ 3.0 3.1 Loffredo CA, Hirata J, Wilson PD, Ferencz C & Lurie IW. (2001). Atrioventricular septal defects: possible etiologic differences between complete and partial defects. Teratology , 63, 87-93. PMID: 11241431 <87::AID-TERA1014>3.0.CO;2-5 DOI.
- ↑ 4.0 4.1 Franklin RC, Jacobs JP, Krogmann ON, Béland MJ, Aiello VD, Colan SD, Elliott MJ, William Gaynor J, Kurosawa H, Maruszewski B, Stellin G, Tchervenkov CI, Walters Iii HL, Weinberg P & Anderson RH. (2008). Nomenclature for congenital and paediatric cardiac disease: historical perspectives and The International Pediatric and Congenital Cardiac Code. Cardiol Young , 18 Suppl 2, 70-80. PMID: 19063777 DOI.
- ↑ 5.0 5.1 Giroud JM, Jacobs JP, Spicer D, Backer C, Martin GR, Franklin RC, Béland MJ, Krogmann ON, Aiello VD, Colan SD, Everett AD, William Gaynor J, Kurosawa H, Maruszewski B, Stellin G, Tchervenkov CI, Walters HL, Weinberg P, Anderson RH & Elliott MJ. (2010). Report from the international society for nomenclature of paediatric and congenital heart disease: creation of a visual encyclopedia illustrating the terms and definitions of the international pediatric and congenital cardiac code. World J Pediatr Congenit Heart Surg , 1, 300-13. PMID: 23804886 DOI.
- ↑ Dong SZ & Zhu M. (2018). Utility of fetal cardiac magnetic resonance imaging to assess fetuses with right aortic arch and right ductus arteriosus. J. Matern. Fetal. Neonatal. Med. , 31, 1627-1631. PMID: 28438064 DOI.
- ↑ Zhu JY, Fu Y, Nettleton M, Richman A & Han Z. (2017). High throughput in vivo functional validation of candidate congenital heart disease genes inDrosophila. Elife , 6, . PMID: 28084990 DOI.
- ↑ Rydeen AB & Waxman JS. (2016). Cyp26 Enzymes Facilitate Second Heart Field Progenitor Addition and Maintenance of Ventricular Integrity. PLoS Biol. , 14, e2000504. PMID: 27893754 DOI.
- ↑ Best KE & Rankin J. (2016). Long-Term Survival of Individuals Born With Congenital Heart Disease: A Systematic Review and Meta-Analysis. J Am Heart Assoc , 5, . PMID: 27312802 DOI.
- ↑ Miyake T, Shinohara T, Inoue T, Marutani S & Takemura T. (2011). Spontaneous closure of muscular trabecular ventricular septal defect: comparison of defect positions. Acta Paediatr. , 100, e158-62. PMID: 21517965 DOI.
- ↑ Michalski AM, Richardson SD, Browne ML, Carmichael SL, Canfield MA, VanZutphen AR, Anderka MT, Marshall EG & Druschel CM. (2015). Sex ratios among infants with birth defects, National Birth Defects Prevention Study, 1997-2009. Am. J. Med. Genet. A , 167A, 1071-81. PMID: 25711982 DOI.
- ↑ Pendse N, Gupta S, Geelani MA, Minhas HS, Agarwal S, Tomar A & Banerjee A. (2009). Repair of atrial septal defects on the perfused beating heart. Tex Heart Inst J , 36, 425-7. PMID: 19876418
- ↑ 13.0 13.1 Faig-Leite FS & Faig-Leite H. (2008). Anatomy of a dextrocardia case with situs solitus. Arq. Bras. Cardiol. , 91, e64-6. PMID: 19142355
- ↑ Kenny D & Hijazi ZM. (2011). Coarctation of the aorta: from fetal life to adulthood. Cardiol J , 18, 487-95. PMID: 21947983
- ↑ Moons P, Sluysmans T, De Wolf D, Massin M, Suys B, Benatar A & Gewillig M. (2009). Congenital heart disease in 111 225 births in Belgium: birth prevalence, treatment and survival in the 21st century. Acta Paediatr. , 98, 472-7. PMID: 19046347 DOI.
- ↑ Pedra CA, Haddad J, Pedra SF, Peirone A, Pilla CB & Marin-Neto JA. (2009). Paediatric and congenital heart disease in South America: an overview. Heart , 95, 1385-92. PMID: 19174420 DOI.
Articles
Kumar SD, Dheen ST & Tay SS. (2007). Maternal diabetes induces congenital heart defects in mice by altering the expression of genes involved in cardiovascular development. Cardiovasc Diabetol , 6, 34. PMID: 17967198 DOI.
Search Pubmed
Search Pubmed: Cardiovascular System Abnormalities
5 Most Recent
Note - This sub-heading shows an automated computer PubMed search using the listed sub-heading term. References appear in this list based upon the date of the actual page viewing. Therefore the list of references do not reflect any editorial selection of material based on content or relevance. In comparison, references listed on the content page and discussion page (under the publication year sub-headings) do include editorial selection based upon relevance and availability. (More? Pubmed Most Recent)
Ventricular Septal Defect
<pubmed limit=5>Ventricular+Septal+Defect</pubmed>
Atrial Septal Defect
<pubmed limit=5>Atrial+Septal+Defect</pubmed>
Patent Ductus Arteriosus
<pubmed limit=5>Patent+Ductus+Arteriosus</pubmed>
Tetralogy of Fallot
<pubmed limit=5>Tetralogy+of+Fallot</pubmed>
Terms
| Cardiovascular Terms |
|---|
Cardiovascular System Development See also Heart terms, Immune terms and Blood terms.
|
| Other Terms Lists |
|---|
| Terms Lists: ART | Birth | Bone | Cardiovascular | Cell Division | Endocrine | Gastrointestinal | Genital | Genetic | Head | Hearing | Heart | Immune | Integumentary | Neonatal | Neural | Oocyte | Palate | Placenta | Radiation | Renal | Respiratory | Spermatozoa | Statistics | Tooth | Ultrasound | Vision | Historic | Drugs | Glossary |
External Links
External Links Notice - The dynamic nature of the internet may mean that some of these listed links may no longer function. If the link no longer works search the web with the link text or name. Links to any external commercial sites are provided for information purposes only and should never be considered an endorsement. UNSW Embryology is provided as an educational resource with no clinical information or commercial affiliation.
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, June 23) Embryology Cardiovascular System - Abnormalities. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Cardiovascular_System_-_Abnormalities
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G