Lecture - Gastrointestinal Development
| Embryology - 10 Jun 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Endoderm Development
Introduction
This lecture will cover the early development of the endoderm layer of the trilaminar embryo as it contributes to the lining, glands and organs of the gastrointestinal tract (GIT).
Gastrulation, or gut formation, was historically the easiest observable feature of frog development. In human development, during the 4th week the 3 distinct portions (fore-, mid- and hind-gut) extend the length of the embryo and will contribute different structures.
The oral cavity (mouth) is formed following breakdown of the buccopharyngeal membrane (= oropharyngeal or oral) and the opening means that it contains amniotic fluid, which is also swallowed later in development.
The large mid-gut is generated by lateral embryonic folding which "pinches off" a pocket of the yolk sac, the 2 compartments continue to communicate through the vitelline duct.
The hindgut (cloaca) will later be divided into separate urogenital and rectal regions that end at the cloacal membrane.
Note that we will be returning in the laboratory and later (head, endocrine, neural crest) to discuss the gastrointestinal tract, associated organs and physical growth changes.
Lecture Objectives

- Understanding of germ layer contributions to the early gastrointestinal tract (GIT)
- Understanding of the folding of the GIT
- Understanding of three main GIT embryonic divisions
- Understanding of associated organ development (liver, pancreas, spleen)
- Brief understanding of mechanical changes (rotations) during GIT development
- Brief understanding of gastrointestinal abnormalities
Lecture Resources
| Movies | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Week 4-5 Stage 13 |
Week 8 Stage 22 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||




Germ Layer Contributions
- Endoderm - epithelium and associated glands.
- Mesoderm (splanchnic) - mesentry, connective tissues, smooth muscle, blood vessels.
- Ectoderm (neural crest) - enteric nervous system.
Both endoderm and mesoderm will contribute to associated organs.
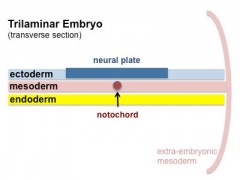
Folding of the embryonic disc occurs ventrally around the notochord, which forms a rod-like region running rostro-caudally in the midline.
In relation to the notochord:
- Laterally (either side of the notochord) lies mesoderm.
- Rostrally (above the notochord end) lies the buccopharyngeal membrane, above this again is the mesoderm region forming the heart.
- Caudally (below the notochord end) lies the primitive streak (where gastrulation occurred), below this again is the cloacal membrane.
- Dorsally (above the notochord) lies the neural tube then ectoderm.
- Ventrally (beneath the notochord) lies the mesoderm then endoderm.
The ventral endoderm (shown yellow) has grown to line a space called the yolk sac. Folding of the embryonic disc "pinches off" part of this yolk sac forming the first primative GIT.
| <html5media height="340" width="300">File:Endoderm 003.mp4</html5media> | 
|
Coelomic Cavity
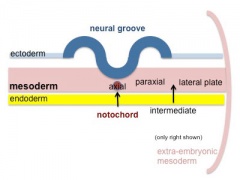
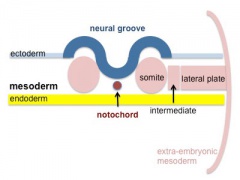
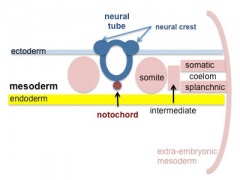
- The mesoderm initially undergoes segmentation to form paraxial, intermediate mesoderm and lateral plate mesoderm.
- Paraxial mesoderm segments into somites and lateral plate mesoderm divides into somatic and splanchnic mesoderm.
- The space forming between them is the coelomic cavity, that will form the 3 major body cavities (pericardial, pleural, peritoneal)
- Most of the gastrointestinal tract will eventually lie within the peritoneal cavity.
- Mesoderm and Ectoderm Cartoons
Trilaminar Embryo
Paraxial and Lateral Plate
Somites
Somatic and Splanchnic




(Note only the righhand side is shown, lefthand side would be identical.)
Week 4
(Gestational age GA 6 weeks) Carnegie stage 11

|

|

|
| Embryo (stage 11 ventral view) | Embryo (midline section) | Embryo (EM section) endoderm, splanchnic mesoderm, Intraembryonic coelom |

|

|
|
| Stomodeum | Buccopharyngeal membrane |

Stage 7 Membranes

Stage 11 25 days, Low power ventral view of the Buccopharyngeal Membrane

Higher power ventrolateral view of the Buccopharyngeal Membrane

Close up view of the degenerating Buccopharyngeal Membrane

Stage 12 Week 4, 26 days

Stage 12 Cloacal membrane





Liver Development

|

|

|
Endoderm and splanchnic mesoderm at the level of the transverse septum (week 4)
- Stage 11 - hepatic diverticulum development
- Stage 12 - cell differentiation, septum transversum forming liver stroma, hepatic diverticulum forming hepatic trabeculae
- Stage 13 - epithelial cord proliferation enmeshing stromal capillaries
The liver initially occupies the entire anterior body. All blood vessels enter the liver (placental, vitelline) and leave to enter the heart.
Stomach
|
|

|
|
- During week 4 at the level where the stomach will form the tube begins to dilate, forming an enlarged lumen.
- The dorsal border grows more rapidly than ventral first rotation (of 90 degrees), which establishes the greater curvature of the stomach.
- A second rotation (of 90 degrees) occurs on the longitudinal axis establishing the adult orientation of the stomach.
Week 5
(GA 7 weeks)
Canalization
|
|
Mesentery Development

|
Spleen
|
Week 8 - 10
(GA 10-12 weeks)
Intestine Herniation


|
|
Intestine Rotation

Normal intestinal rotation (note these are gestational age GA weeks)[1]
Hindgut
|
|
Gastrointestinal Tract Divisions
| During the 4th week the 3 distinct portions (fore-, mid- and hind-gut) extend the length of the embryo and will contribute different components of the GIT. These 3 divisions are also later defined by the vascular (artery) supply to each of theses divisions.
|

Gastrointestinal Tract Blood Supply |
Fetal

|

|
| Small Intestine length (mm) | Liver Growth (weight grams) |
| 1 to 124 grams (birth) |
Liver
- Differentiates to form the hepatic diverticulum and hepatic primordium, generates the gall bladder then divides into right and left hepatic (liver) buds.
- Hepatic Buds - form hepatocytes, produce bile from week 13 (forms meconium of newborn)
- Left Hepatic Bud - left lobe, quadrate, caudate (both q and c anatomically Left) caudate lobe of human liver consists of 3 anatomical parts: Spiegel's lobe, caudate process, and paracaval portion.
- Right Hepatic Bud - right lobe
- Bile duct - 3 connecting stalks (cystic duct, hepatic ducts) which fuse.
- Early liver also involved in blood formation, after the yolk sac and blood islands acting as a primary site.
Pancreas

- Pancreatic buds - endoderm, covered in splanchnic mesoderm
- Pancreatic bud formation – duodenal level endoderm, splanchnic mesoderm forms dorsal and ventral mesentery, dorsal bud (larger, first), ventral bud (smaller, later)
- Duodenum growth/rotation – brings ventral and dorsal buds together, fusion of buds, exocrine function (postnatal function)
- Pancreatic duct – ventral bud duct and distal part of dorsal bud
- Pancreatic islets - endocrine function (week 10 onwards)

Spleen
|

Gastrointestinal Tract Abnormalities

| USA Statistics | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Lumen Abnormalities
There are several types of abnormalities that impact upon the continuity of the gastrointestinal tract lumen.
Atresia
Stenosis
Duplication
|
![Gastrointestinal tract duplication sites based upon 78 clinical studies.[2]](/embryology/index.php?title=File:Gastrointestinal_tract_duplication_sites.jpg)
|
Meckel's Diverticulum
|

Meckel's Diverticulum |
Intestinal Malrotation
Presents clinically in symptomatic malrotation as:
|

Intestinal malrotation |
Intestinal Aganglionosis
(intestinal aganglionosis, Hirschsprung's disease, aganglionic colon, megacolon, congenital aganglionic megacolon, congenital megacolon)
|

|
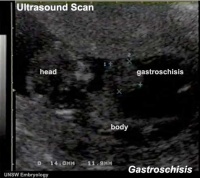
Gastroschisis
| Gastroschisis (omphalocele, paraomphalocele, laparoschisis, abdominoschisis, abdominal hernia) is a congenital abdominal wall defect which results in herniation of fetal abdominal viscera (intestines and/or organs) into the amniotic cavity.
Incidence of gastroschisis has been reported at 1.66/10,000, occuring more frequently in young mothers (less than 20 years old). By definition, it is a body wall defect, not a gastrointestinal tract defect, which in turn impacts upon GIT development. This indirect developmental effect (one system impacting upon another) occurs in several other systems.
|
|
| Gastroschisis |
Final Thoughts- After Birth
Remember that the GIT does not function until after birth consider:
- metabolic disorders discovered by neonatal diagnosis
- Neonatal feeding difficulties due to cleft lip and cleft palate.
{kind=link}
Links: Gastrointestinal Tract - Abnormalities
- ↑ <pubmed>20549505</pubmed>| PMC2908440
- ↑ <pubmed>718292</pubmed>
Terms
| Gastrointestinal Tract Terms | ||
|---|---|---|
| ||
|
- 2015 Course: Week 2 Lecture 1 Lecture 2 Lab 1 | Week 3 Lecture 3 Lecture 4 Lab 2 | Week 4 Lecture 5 Lecture 6 Lab 3 | Week 5 Lecture 7 Lecture 8 Lab 4 | Week 6 Lecture 9 Lecture 10 Lab 5 | Week 7 Lecture 11 Lecture 12 Lab 6 | Week 8 Lecture 13 Lecture 14 Lab 7 | Week 9 Lecture 15 Lecture 16 Lab 8 | Week 10 Lecture 17 Lecture 18 Lab 9 | Week 11 Lecture 19 Lecture 20 Lab 10 | Week 12 Lecture 21 Lecture 22 Lab 11 | Week 13 Lecture 23 Lecture 24 Lab 12 | 2015 Projects: Three Person Embryos | Ovarian Hyper-stimulation Syndrome | Polycystic Ovarian Syndrome | Male Infertility | Oncofertility | Preimplantation Genetic Diagnosis | Students | Student Designed Quiz Questions | Moodle page
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, June 10) Embryology Lecture - Gastrointestinal Development. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Lecture_-_Gastrointestinal_Development
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G