Musculoskeletal System - Axial Skeleton Development
| Embryology - 12 Jul 2026 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Introduction

During the third week the paraxial mesoderm forms into "balls" of mesoderm paired either side of the neural groove, called somites, that are patterned by the notochord. Similar regions of each somite differentiate initially into 2 parts: the dermomyotome (dermal and muscle component) and the sclerotome (forms vertebral column). Each somite undergoes a segmental shift to form a vertebral body and the intervertebral disc.
The sclerotome mesenchyme first differentiates to form cartilage, that ossifies through endochondral ossification to form bone. The vertebral body begins as a bony collar that expands into regions of dying cartilage. The vertebral arch, enclosing the spinal cord, forms later and the arch remains open dorsally (linked by a ligament) to allow continued growth of the spinal cord.
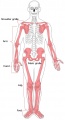
The axial skeleton consists of: skull, Auditory Ossicles, Hyoid bone, Vertebral column, Chest (sternum, ribs)
The vertebral column is a series of bone segments (vertebra) separated by specialized joints (intervertebral disc).
In the adult, the vertebra form rostro-caudally: 7 cervical, 12 thoracic, 5 lumbar, 1 sacrum, coccyx. There has been identified a population variability in the distribution of the number of vertebra.
Skeletal ossification continues postnatally, through puberty until mid-20s. Abnormalities of vertebral column development can lead to defects including scoliosis.
See this series of articles by O'Rahilly, Müller and others on human vertebral column development using embryos from the Carnegie Collection.[1][2][3][4][5][6]
| skull (22) | Auditory Ossicles (6) | Hyoid bone (1) | Vertebral Column (26) | Thoracic cage (27) |
|---|---|---|---|---|
|
|
|||
| Links: axial skeleton |
Some Recent Findings
|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Axial Skeleton Development | Vertebral Column Development | Vertebra Development | Intervertebral Disc Development | Rib Development | Scoliosis |
| Older papers |
|---|
| These papers originally appeared in the Some Recent Findings table, but as that list grew in length have now been shuffled down to this collapsible table.
See also the Discussion Page for other references listed by year and References on this current page.
|
Textbooks

- The Developing Human: Clinically Oriented Embryology (8th Edition) by Keith L. Moore and T.V.N Persaud - Moore & Persaud Chapter 15 the skeletal system
- Larsen’s Human Embryology by GC. Schoenwolf, SB. Bleyl, PR. Brauer and PH. Francis-West - Chapter 11 Limb Dev (bone not well covered in this textbook)
- Before we Are Born (5th ed.) Moore and Persaud Chapter 16,17: p379-397, 399-405
- Essentials of Human Embryology Larson Chapter 11 p207-228
Objectives
- Identify the components of a somite and the adult derivatives of each component.
- Give examples of sites of (a) endochondral and (b) intramembranous ossification and to compare these two processes.
- Identify the general times (a) of formation of primary and (b) of formation of secondary ossification centres, and (c) of fusion of such centres with each other.
- Briefly summarise the development of the limbs.
- Describe the developmental abnormalities responsible for the following malformations: selected growth plate disorders; congenital dislocation of the hip; scoliosis; arthrogryposis; and limb reduction deformities.
Development Overview
Below is a very brief overview using simple figures of 3 aspects of early musculoskeletal development. More detailed overviews are shown on other notes pages Mesoderm and Somite, Vertebral Column, Limb in combination with serial sections and Carnegie images.
Mesoderm

|
Cells migrate through the primitive streak to form mesodermal layer. Extraembryonic mesoderm lies adjacent to the trilaminar embryo totally enclosing the amnion, yolk sac and forming the connecting stalk. |

|
Paraxial mesoderm accumulates under the neural plate with thinner mesoderm laterally. This forms 2 thickened streaks running the length of the embryonic disc along the rostrocaudal axis. In humans, during the 3rd week, this mesoderm begins to segment. The neural plate folds to form a neural groove and folds. |

|
Segmentation of the paraxial mesoderm into somites continues caudally at 1 somite/90minutes and a cavity (intra-embryonic coelom) forms in the lateral plate mesoderm separating somatic and splanchnic mesoderm.
Note intra-embryonic coelomic cavity communicates transiently with extra-embryonic coelom through portals (holes) initially on lateral margin of embryonic disc. |

|
Somites continue to form. The neural groove fuses dorsally to form a tube at the level of the 4th somite and "zips up cranially and caudally and the neural crest migrates into the mesoderm. |
Sclerotome
The sclerotome forms from the ventromedial portion (region) of each somite with a mesenchymal cell organisation. The left and right sclerotome from each somite level contributes the vertebra and intervertebral disc of the entire axial skeleton.

|
Mesoderm beside the notochord (axial mesoderm, blue) thickens, forming the paraxial mesoderm as a pair of strips along the rostro-caudal axis. |

|
Paraxial mesoderm towards the rostral end, begins to segment forming the first somite. Somites are then sequentially added caudally. The somitocoel, is a cavity forming in early somites, which is lost as the somite matures. |

|
Cells in the somite differentiate medially to form the sclerotome (forms vertebral column) and dorsolaterally to form the dermomyotome. |

|
The dermomyotome then forms the dermotome (forms dermis) and myotome (forms muscle).
Neural crest cells migrate beside and through somite. |

|
The myotome differentiates to form 2 components dorsally the epimere and ventrally the hypomere, which in turn form epaxial and hypaxial muscles respectively. The bulk of the trunk and limb muscle coming from the Hypaxial mesoderm. Different structures will be contributed depending upon the somite level. |
Axial Features
- human occipitocervical segmentation[13]
- head and vertebral column boundary - located between the 5th and 6th somites[14]
- craniovertebral junction - caudal occiput, atlas, and axis[15]
Embryonic Development
Week 8

Human embryo (Stage 22) vertebra and spinal cord development. Note the structure of the vertebral arch, the dorsal ligament allowing expansion of the arch to accommodate spinal cord growth.
Skull

- Links: Skull Development
Vertebral Column
Cervical Vertebra

- C1 - (atlas) from fourth occipital and first cervical sclerotomes. Posterior arch ossifies from 2 centres in the lateral masses fusing postnatally between 3 - 5th years.
A comparison of vertebral element ossification between different species also in relation to Hox gene expression.[16]
- For each taxon, circles indicate centra, and squares indicate left and right neural arches.
- Colours represent the order of ossification.
- Hox expression boundaries in the mouse (placentals) and vertebral segment identity are shown at right.
- Conserved timing of V7 centrum ossification across mammals, including sloths (bradypus)
- Overlap in Hox5-6 expression in the V6–V9 region of the sloth neck.
bradypus - three-toed sloths are the only members of this genus
dasypus - armadillo genus in the Dasypodidae family
Sacrum
Evolution of the sacrum[17] "In order to study the formation of the sacrum during the primate evolution, a new way of numbering mammalian vertebrae is presented; this demonstrates that the thoracolumbosacral complex is fixed at 22 vertebrae in 80% and at 22 +/- 1 in 100% of the cases. The shift of a vertebra from one type to another occurs either at the thoracolumbar or at the lumbosacral junction and not at the cervicothoracic junction. Rarely does the shift take place at the sacrococcygeal junction. Data from 318 primates reveal that the seven original lumbar vertebrae of the Old World monkeys are reduced in the great apes by a caudad "thoracization" of one to two lumbar vertebrae and a cephalad sacralization of one to four lumbar vertebrae. In the apes, sacralization is not total and different stages that are intermediate between lumbar and sacral are described. In Homo sapiens there is a total sacralization of the last two original lumbar vertebrae. In addition, development of the sacral wings (alae) is minimal in apes and reaches its maximum in hominids. The tendency of the hominoid sacrum to incorporate the last lumbar vertebrae and to widen markedly provides for an enhanced articulation of the sacrum with the ilium and offers a firm base of support for the trunk during erect posture. This is necessary for the support of the weight of the trunk above the sacrum and for the stabilization of the body during bipedal posture and locomotion. Encephalization did not play any major role in the widening of the sacrum since the former by far preceded the latter."
Intervertebral Disc

The adult intervertebral disc (IVD) has to bear the same loads as the vertebra and also have flexibility to allow axial column movement. This is achieved by a complex structure (cartilaginous end-plate) that links the vertebra above and below the disc to a outer dense fibrous structure (annulus fibrosus) containing a gel-like core region (nucleus pulposus). Some research in this area focusses on the degeneration of the IVD with ageing.
- cartilaginous end-plate - that anchor the discs to the adjacent vertebral body bones
- annulus fibrosus - cells are derived from the sclerotome
- nucleus pulposus - cells are derived from the notochord[19]
Annulus Fibrosus
- cells are derived from the sclerotome
Nucleus Pulposus
- cells are derived from the notochord[19]
- notochordal marker brachyury
- proteoglycan rich extracellular matrix
Rib Development


Humans form 12 paired ribs from the cartilaginous costal processes of the developing thoracic vertebrae. Early rib development occurs at 7 weeks (((GA}} week 9) from lateral plate mesoderm and continues postnatal with secondary ossification centres appearing at 15 years of age.
A recent paper has looked at rib cage development[7] between embryonic Week 7 to Week 9, 17 to 23. First identifying cartilage formation at CS1717 that expanding outward from the dorsal side of the chest-abdominal region. Ribs elongated progressively to surround the chest, differentiating into the upper and lower rib cage regions by CS20.
- First 7 “true” ribs connect to the sternum through the costal cartilages about day 45.
- Lower 5 “false” ribs do not connect to the sternum.
- Human Embryonic Rib Development

Embryo 13 mm CRL
Embryo 17 mm CRL
Embryo 16 mm CRL

Embryo 32 mm CRL





Sox9 expression in the Mouse (E12.5) rib primordial.[20]
| Historic Rib papers |
|---|
| Bardeen CR. XI. Development of the Skeleton and of the Connective Tissues in Keibel F. and Mall FP. Manual of Human Embryology I. (1910) J. B. Lippincott Company, Philadelphia.
Chondrogenous Period and Rib Development
|
Developmental rib abnormalities may be isolated or can occur with other congenital anomalies.
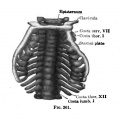
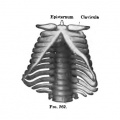
Sternum Development
The sternum and sternal ribs derive from the somatic layer of the lateral plate mesoderm.[21][22]
| Historic Sternum papers |
|---|
| Paterson The sternum - its early development and ossification in man and mammals. (1900) J Anat Physiol. 35(1): 21-32 PMID 17232454
Keith A. Human Embryology and Morphology. (1902) London: Edward Arnold. Body Wall, Ribs, and Sternum Whitehead RH. and Waddell JA. The early development of the mammalian sternum (1911) Amer. J Anat. 12: 89-106. |
Molecular
Like many other embryonic structures there are two separate considerations:
- Pattern Formation - sclerotome differentiation and segmentation
- Overt Differentiation - mesoderm differentiation to cartilage differentiation and ossification to bone.
Notch
- Links: Notch
Nuclear factor of activated T-cells, cytoplasmic 1
- Transcription factor (Nfatc1) has been identified in developing mouse intervertebral disc (IVD).
- The NFAT family of transcription factors regulates cytokine gene expression by binding to the promoter/enhancer regions of antigen-responsive genes, usually in cooperation with heterologous DNA-binding partners.
- The activation of NFAT proteins is controlled by calcineurin, the calmodulin-dependent phosphatase.
- Links: OMIM - NFATC1
Transforming growth factor beta
Two functions in IVD development:[18]
- prevent chondrocyte differentiation in the presumptive IVD
- promote differentiation of annulus fibrosus from sclerotome
Abnormalities
Spina Bifida

Folic Acid and Neural Tube Defects
Absent Cervical Spine Pedicle

Absent cervical spine pedicle[23]
The vertebral pedicles (Latin, pediculus ="small foot") are paired processes that project dorsally and connect the body of the spinal vertebra to the arch. Absence is a rare abnormality characterized by the absence of a pedicle of the affected vertebral body, seen most frequently at the level C6 followed by the level C5 and C7.
Scoliosis





- frequency of congenital scoliosis is approximately 0.5, or 1 in 1,000 births.
- assymetric growth impairment of vertebral bodies
- lateral deviation of spine (Lateral flexion, Forward flexion, Rotation of vertebral column on long axis)
- compensated by movement of vertebral column above and below affected region (producing a primary and two secondary curves)
- progresses rapidly in adolescence and becomes fixed once bone growth is completed.
- both genetic and environmental terartogens implicated.
- Links: Scoliosis
VACTERL
| ICD-11 - LD2F.11 VATER association - VACTERL/VATER is an association of congenital malformations typically characterized by the presence of at least three of the following: vertebral defects, anal atresia, cardiac defects, tracheo-esophageal fistula, renal anomalies, and limb abnormalities. |
VACTERL/VATER are the acronyms used to describe a multi-system congenital malformations including at least three of the following:
- Vertebral defects
- Anal atresia
- Cardiac defects
- Tracheo-esophageal fistula
- Renal anomalies
- Limb abnormalities
| VACTERL Clinical Diagnosis | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||
- Links: VACTERL
Sagittal Cleft Vertebra
Sagittal cleft vertebra, "butterfly vertebrae" or anterior rachischisis, is an abnormal vertebral body caused by failure of fusion of the 2 lateral chondrification centres during development. The term "butterfly vertebrae" is based upon the butterfly wings appearance of the 2 hemivertebrae on x-ray. See a recent review.{{#pmid"31448202|PMID31448202}}
- Links: Sagittal Cleft Vertebra
Spondylocostal Dysostosis
A rare heritable axial skeleton growth disorder characterized by abnormal development of vertebra, multiple segmentation defects, and ribs.
- Links: GeneReviews | Spondylocostal Dysostosis
References
- ↑ O'Rahilly R & Meyer DB. (1979). The timing and sequence of events in the development of the human vertebral column during the embryonic period proper. Anat. Embryol. , 157, 167-76. PMID: 517765
- ↑ O'Rahilly R, Muller F & Meyer DB. (1980). The human vertebral column at the end of the embryonic period proper. 1. The column as a whole. J. Anat. , 131, 565-75. PMID: 7216919
- ↑ O'Rahilly R, Müller F & Meyer DB. (1983). The human vertebral column at the end of the embryonic period proper. 2. The occipitocervical region. J. Anat. , 136, 181-95. PMID: 6833119
- ↑ O'Rahilly R, Müller F & Meyer DB. (1990). The human vertebral column at the end of the embryonic period proper. 3. The thoracicolumbar region. J. Anat. , 168, 81-93. PMID: 2323997
- ↑ O'Rahilly R, Müller F & Meyer DB. (1990). The human vertebral column at the end of the embryonic period proper. 4. The sacrococcygeal region. J. Anat. , 168, 95-111. PMID: 2182589
- ↑ Müller F & O'Rahilly R. (1994). Occipitocervical segmentation in staged human embryos. J. Anat. , 185 ( Pt 2), 251-8. PMID: 7961131
- ↑ 7.0 7.1 Okuno K, Ishizu K, Matsubayashi J, Fujii S, Sakamoto R, Ishikawa A, Yamada S, Yoneyama A & Takakuwa T. (2019). Rib Cage Morphogenesis in the Human Embryo: A Detailed Three-Dimensional Analysis. Anat Rec (Hoboken) , 302, 2211-2223. PMID: 31344324 DOI.
- ↑ Arlegi M, Veschambre-Couture C & Gómez-Olivencia A. (2019). Evolutionary selection and morphological integration in the vertebral column of modern humans. Am. J. Phys. Anthropol. , , . PMID: 31675109 DOI.
- ↑ Skórzewska A, Grzymisławska M, Bruska M, Lupicka J & Woźniak W. (2013). Ossification of the vertebral column in human foetuses: histological and computed tomography studies. Folia Morphol. (Warsz) , 72, 230-8. PMID: 24068685
- ↑ Maier JA, Lo Y & Harfe BD. (2013). Foxa1 and Foxa2 are required for formation of the intervertebral discs. PLoS ONE , 8, e55528. PMID: 23383217 DOI.
- ↑ Alexander PG & Tuan RS. (2010). Role of environmental factors in axial skeletal dysmorphogenesis. Birth Defects Res. C Embryo Today , 90, 118-32. PMID: 20544699 DOI.
- ↑ Pang D & Thompson DN. (2011). Embryology and bony malformations of the craniovertebral junction. Childs Nerv Syst , 27, 523-64. PMID: 21193993 DOI.
- ↑ <pubmed>14529047</pubmed>
- ↑ Christ B & Wilting J. (1992). From somites to vertebral column. Ann. Anat. , 174, 23-32. PMID: 1605355
- ↑ Raybaud C. (2011). Anatomy and development of the craniovertebral junction. Neurol. Sci. , 32 Suppl 3, S267-70. PMID: 21822704 DOI.
- ↑ 16.0 16.1 Hautier L, Weisbecker V, Sánchez-Villagra MR, Goswami A & Asher RJ. (2010). Skeletal development in sloths and the evolution of mammalian vertebral patterning. Proc. Natl. Acad. Sci. U.S.A. , 107, 18903-8. PMID: 20956304 DOI.
- ↑ Abitbol MM. (1987). Evolution of the sacrum in hominoids. Am. J. Phys. Anthropol. , 74, 65-81. PMID: 3688211 DOI.
- ↑ 18.0 18.1 18.2 Sohn P, Cox M, Chen D & Serra R. (2010). Molecular profiling of the developing mouse axial skeleton: a role for Tgfbr2 in the development of the intervertebral disc. BMC Dev. Biol. , 10, 29. PMID: 20214815 DOI.
- ↑ 19.0 19.1 Risbud MV, Schaer TP & Shapiro IM. (2010). Toward an understanding of the role of notochordal cells in the adult intervertebral disc: from discord to accord. Dev. Dyn. , 239, 2141-8. PMID: 20568241 DOI.
- ↑ Plummer NW, Spicher K, Malphurs J, Akiyama H, Abramowitz J, Nürnberg B & Birnbaumer L. (2012). Development of the mammalian axial skeleton requires signaling through the Gα(i) subfamily of heterotrimeric G proteins. Proc. Natl. Acad. Sci. U.S.A. , 109, 21366-71. PMID: 23236180 DOI.
- ↑ Sadler TW. (2000). Embryology of the sternum. Chest Surg. Clin. N. Am. , 10, 237-44, v. PMID: 10803330
- ↑ Mekonen HK, Hikspoors JP, Mommen G, Köhler SE & Lamers WH. (2015). Development of the ventral body wall in the human embryo. J. Anat. , 227, 673-85. PMID: 26467243 DOI.
- ↑ Guggenberger R, Andreisek G, Scheffel H, Wildermuth S, Leschka S & Stolzmann P. (2010). Absent cervical spine pedicle and associated congenital spinal abnormalities - a diagnostic trap in a setting of acute trauma: case report. BMC Med Imaging , 10, 25. PMID: 21062465 DOI.
- ↑ Postema SG, van der Sluis CK, Waldenlöv K & Norling Hermansson LM. (2012). Body structures and physical complaints in upper limb reduction deficiency: a 24-year follow-up study. PLoS ONE , 7, e49727. PMID: 23226218 DOI.
- ↑ Zaborowska-Sapeta K, Kowalski IM, Kotwicki T, Protasiewicz-Fałdowska H & Kiebzak W. (2011). Effectiveness of Chêneau brace treatment for idiopathic scoliosis: prospective study in 79 patients followed to skeletal maturity. Scoliosis , 6, 2. PMID: 21266084 DOI.
- ↑ Solomon BD. (2011). VACTERL/VATER Association. Orphanet J Rare Dis , 6, 56. PMID: 21846383 DOI.
Reviews
Pang D & Thompson DN. (2011). Embryology and bony malformations of the craniovertebral junction. Childs Nerv Syst , 27, 523-64. PMID: 21193993 DOI.
Iimura T, Denans N & Pourquié O. (2009). Establishment of Hox vertebral identities in the embryonic spine precursors. Curr. Top. Dev. Biol. , 88, 201-34. PMID: 19651306 DOI.
Alexander T, Nolte C & Krumlauf R. (2009). Hox genes and segmentation of the hindbrain and axial skeleton. Annu. Rev. Cell Dev. Biol. , 25, 431-56. PMID: 19575673 DOI.
Mallo M, Vinagre T & Carapuço M. (2009). The road to the vertebral formula. Int. J. Dev. Biol. , 53, 1469-81. PMID: 19247958 DOI.
Tyl RW, Chernoff N & Rogers JM. (2007). Altered axial skeletal development. Birth Defects Res. B Dev. Reprod. Toxicol. , 80, 451-72. PMID: 18157900 DOI.
Articles
Mead TJ & Yutzey KE. (2009). Notch pathway regulation of chondrocyte differentiation and proliferation during appendicular and axial skeleton development. Proc. Natl. Acad. Sci. U.S.A. , 106, 14420-5. PMID: 19590010 DOI.
Skuntz S, Mankoo B, Nguyen MT, Hustert E, Nakayama A, Tournier-Lasserve E, Wright CV, Pachnis V, Bharti K & Arnheiter H. (2009). Lack of the mesodermal homeodomain protein MEOX1 disrupts sclerotome polarity and leads to a remodeling of the cranio-cervical joints of the axial skeleton. Dev. Biol. , 332, 383-95. PMID: 19520072 DOI.
Wilson V, Olivera-Martinez I & Storey KG. (2009). Stem cells, signals and vertebrate body axis extension. Development , 136, 1591-604. PMID: 19395637 DOI.
Search PubMed
Search Pubmed: Axial Skeleton Development | Vertebra Development | Intervertebral Disc Development | Axial Skeleton Abnormalities
Additional Images

Adult axial skeleton
Adult appendicular skeleton

Bone structure
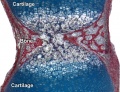
Developing vertebra

Fetal head lateral (12 weeks)
Fetal head medial (12 weeks)

Fetal head section (12 weeks)

Historic plate - human axis development






Historic
| Human Embryology And Morphology (1921) |
|---|
Keith, A. Human Embryology And Morphology (1921) Longmans, Green & Co.:New York.
|















Terms
- centrum - (vertebral body) anatomical term referring to the main bony part of the vertebra that forms the majority of the axial skeleton.
- Cobb angle - clinical method of measuring the degree of scoliosis and post-traumatic kyphosis. Named after the American orthopedic surgeon John Robert Cobb (1903 - 1967) an American orthopedic surgeon.
- haemal arch - referring to the bony arch region within animal tail vertebra that contains blood vessels.
- idiopathic scoliosis - clinical term for a spinal column deformity appearing usually postnatally after the age of 10 years old.
- lordosis - clinical and anatomy term describing the curvature of the spine with the convexity toward the front. Normal to have lordosis in the cervical and lumbar regions of the spinal column.
- neural arch - referring to the bony arch region within vertebra that contains the spinal cord.
- notochord sheath - region surrounding the notochord. in teleost fish direct mineralization of this region, by intramembranous ossification, forms the initial vertebral centrum. (More? zebrafish)
- rib hump - clinical term for the prominence formed by ribs on the convexity of a curve, caused by rotation of the spine and attached ribs.
- spinal column - term referring to the musculoskeletal elements (vertebrae, ligaments, and intervertebral discs), that surround the spinal cord and form the axial skeleton.
- synsacrum - in birds sacral and lumbar vertebrae fused region forming elongated sacral region.
- thoracic hypokyphosis - term referring to the backward curve in the upper spine is to great, round back, Scheuermann's disease, or simply kyphosis.
Terms
| Bone Terms | ||
|---|---|---|
Bone Development
| ||
|
External Links
External Links Notice - The dynamic nature of the internet may mean that some of these listed links may no longer function. If the link no longer works search the web with the link text or name. Links to any external commercial sites are provided for information purposes only and should never be considered an endorsement. UNSW Embryology is provided as an educational resource with no clinical information or commercial affiliation.
- Scoliosis Australia
- Scoliosis - the official journal of the Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) and affiliated with the International Research Society of Spinal Deformities (IRSSD).
- Young Women's Health - scoliosis
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2026, July 12) Embryology Musculoskeletal System - Axial Skeleton Development. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Musculoskeletal_System_-_Axial_Skeleton_Development
- © Dr Mark Hill 2026, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G