Bold text
Introduction
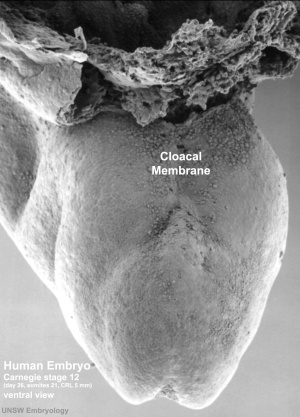
Human Embryo stage
12 cloacal membrane (SEM}
The initial cloaca is the common early endoderm lined space of the hindgut that will later become partitioned by a septum into a dorsal gastrointestinal component (rectum) and ventral renal/genital component (urogenital sinus). Note that the cloaca in mammals is an early embryonic transient structure and only persists in birds and reptiles. Located at the superior end of the cloaca is the allantois, that extends into the connecting stalk and later the placental cord. Located at the inferior end of the cloaca is the cloacal membrane, that also forms part of the embryo surface.
The gastrointestinal tract ends at this cloacal membrane, equivalent to the beginning of the tract at the buccopharyngeal membrane at the upper end. The cloacal membrane is formed during gastrulation by ectoderm and endoderm without a middle (intervening) layer of mesoderm, that later degenerates by apoptosis after cloacal septation.
The hindgut component will contribute to the gastrointestinal tract intestine of the distal transverse colon, descending colon, sigmoid colon, rectum.
The urogenital sinus component will contribute the renal urinary bladder and participate in genital development.
- Links: cloaca | intestine | bladder | genital | apoptosis
- Historic papers: 1911 human cloaca | 1912 Cloaca, Bladder, Urethra, and Urogenital Sinus | 1933 Cloacal Membrane | 1938 persistent cloaca
Some Recent Findings
- The development of the cloaca in the human embryo[1] "Subdivision of cloaca into urogenital and anorectal passages has remained controversial because of disagreements about the identity and role of the septum developing between both passages. This study aimed to clarify the development of the cloaca using a quantitative 3D morphological approach in human embryos of 4-10 post-fertilisation weeks. ...Our main finding was a pronounced difference in growth between rapidly expanding central and ventral parts, and slowly or non-growing cranial and dorsal parts. The entrance of the Wolffian duct into the cloaca proved a stable landmark that remained linked to the position of vertebra S3. Suppressed growth in the cranial cloaca resulted in an apparent craniodorsal migration of the entrance of the Wolffian duct, while suppressed growth in the dorsal cloaca changed the entrance of the hindgut from cranial to dorsal on the cloaca. Transformation of this 'end-to-end' into an 'end-to-side' junction produced temporary 'lateral (Rathke's) folds'. The persistent difference in dorsoventral growth straightened the embryonic caudal body axis and concomitantly extended the frontally oriented 'urorectal (Tourneux's) septum' caudally between the ventral urogenital and dorsal anorectal parts of the cloaca. The dorsoventral growth difference also divided the cloacal membrane into a well-developed ventral urethral plate and a thin dorsal cloacal membrane proper, which ruptured at 6.5 weeks. The expansion of the pericloacal mesenchyme followed the dorsoventral growth difference and produced the genital tubercle. Dysregulation of dorsal cloacal development is probably an important cause of anorectal malformations: too little regressive development may result in anorectal agenesis, and too much regression in stenosis or atresia of the remaining part of the dorsal cloaca." (see also historic 1911 paper)
- Clarification of mammalian cloacal morphogenesis using high-resolution episcopic microscopy[2] "The developmental process through which the cloaca transforms from one hollow structure to two separated urinary and digestive outlets remains controversial and speculative. Here, we use high-resolution episcopic microscopy to examine a comprehensive series of normal and mutant mouse cloaca in which the detailed 3-dimensional (3-D) morphological features are illuminated throughout the development. We provide evidence that the dorsal peri-cloacal mesenchyme (dPCM) remains stationary while other surrounding tissues grow towards it. This causes dramatic changes of spatial relationship among caudal structures and morphological transformation of the cloaca. The 3-D characterizations of Dkk1 mutants reveal a hyperplastic defect of dPCM, which leads to a significant anterior shift of the caudal boundary of the cloaca, premature occlusion of the cloaca and, imperforate anus phenotype. Conversely, Shh knockout causes a severe hypoplastic defect of cloaca mesenchyme including dPCM and persistent cloaca. Collectively, these findings suggest that formation of the dPCM is critical for cloacal morphogenesis and furthermore, growth and movement of the mesenchymal tissues towards the dPCM lead to the cloaca occlusion and separation of the urinary and digestive outlets."
|
| More recent papers
|
|
This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
- This search now requires a manual link as the original PubMed extension has been disabled.
- The displayed list of references do not reflect any editorial selection of material based on content or relevance.
- References also appear on this list based upon the date of the actual page viewing.
References listed on the rest of the content page and the associated discussion page (listed under the publication year sub-headings) do include some editorial selection based upon both relevance and availability.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References
Search term: Cloaca
<pubmed limit=5>Cloaca</pubmed>
Search term: Cloacal Membrane
<pubmed limit=5>Cloacal Membrane</pubmed>
|
| Older papers
|
| These papers originally appeared in the Some Recent Findings table, but as that list grew in length have now been shuffled down to this collapsible table.
See also the Discussion Page for other references listed by year and References on this current page.
|
Movies
| Early Endoderm
|
Week 3 Folding
|
| <html5media height="400" width="350">File:Amnion 001.mp4</html5media>
|
<html5media height="500" width="350">File:Week3_folding.mp4</html5media>
|
- Links: Early Endoderm Movie | Week 3 Folding Movie
Embryonic Development
Stage 10

|

|
Caudal end of embryo showing primitive streak region, cloacal membrane, and connecting stalk.
|
- Links: Carnegie stage 10 | Stage 10 Movie
Stage 11
- Links: Carnegie stage 11
Stage 12
- Links: Carnegie stage 12
Stage 13
| <html5media height="420" width="400">File:Stage13 GIT3d.mp4</html5media>
|
Hindgut and Cloaca (brown - hindgut and cloaca)
|
- Links: Carnegie stage 13 | Stage 13 Movie
Stage 22
Molecular
Sonic Hedgehog
In the mouse model of cloacal development, Shh knockout causes a severe hypoplastic defect of cloaca mesenchyme including dorsal peri-cloacal mesenchyme and persistent cloaca.[2]
- Links: SHH
Apoptosis
apoptosis - process of cell death required for the removal of the cloacal membrane.
Abnormalities
ICD-11 LB17 Structural developmental anomalies of anal canal
Persistent Cloaca
ICD-11 LB17.2 Persistent cloaca is a congenital anomaly in which the intestinal, urinary, and reproductive ducts open into a common cavity, a result of the failure of the urorectal septum to form during prenatal development. They occur exclusively in girls and comprise the most complex defect in the spectrum of anorectal malformations.
Persistent Cloaca Perineum[3]

|
In females this abnormality results in all three structures (urinary tract, vagina, and rectum) all meeting in a common channel, similar to the early developing cloaca. Clinically the presence of a single perineal orifice is evidence of a patient with persistent cloaca.[3]
|
- Links: LB17.2 Persistent cloaca | GIT Abnormalities
Cloacal Exstrophy
ICD-11 LB17.3 Cloacal exstrophy a rare (about 1/200,000[4]) and complex anorectal and genitourinary malformation in which rectum, vagina and urinary tract share a common everted orifice, accompanied by an omphalocele and an imperforate anus. Exstrophy of the cloaca is a well-known malformation that includes the persistence and the exstrophy of a cloaca that receives ureters, ileum and a rudimentary hindgut. Cloacal exstrophy is a severe birth defect wherein much of the abdominal organs (the bladder and intestines) are exposed. It often causes the splitting of both male and female genitalia (specifically, the penis and clitoris respectively), and the anus is occasionally sealed.
- Links: LB17.3 Cloacal exstrophy
OEIS Complex
Omphalocele-Exstrophy-Imperforate Anus-Spinal (OEIS) defects, a combination of defects comprising omphalocele, exstrophy of the cloaca, imperforate anus, and spinal defects.
OMIM: OEIS Complex
References
- ↑ Kruepunga N, Hikspoors JPJM, Mekonen HK, Mommen GMC, Meemon K, Weerachatyanukul W, Asuvapongpatana S, Eleonore Köhler S & Lamers WH. (2018). The development of the cloaca in the human embryo. J. Anat. , 233, 724-739. PMID: 30294789 DOI.
- ↑ 2.0 2.1 Huang YC, Chen F & Li X. (2016). Clarification of mammalian cloacal morphogenesis using high-resolution episcopic microscopy. Dev. Biol. , 409, 106-113. PMID: 26485363 DOI.
- ↑ 3.0 3.1 Levitt MA & Peña A. (2007). Anorectal malformations. Orphanet J Rare Dis , 2, 33. PMID: 17651510 DOI.
- ↑ Ebert AK, Reutter H, Ludwig M & Rösch WH. (2009). The exstrophy-epispadias complex. Orphanet J Rare Dis , 4, 23. PMID: 19878548 DOI.
Books
Reviews
Vilanova-Sanchez A, McCracken K, Halleran DR, Wood RJ, Reck-Burneo CA, Levitt MA & Hewitt G. (2018). Obstetrical outcomes in adult patients born with complex anorectal malformations and cloacal anomalies: a literature review. J Pediatr Adolesc Gynecol , , . PMID: 30367985 DOI.
Peña A. (2016). Cloaca--Historical aspects and terminology. Semin. Pediatr. Surg. , 25, 62-5. PMID: 26969227 DOI.
Gupta A, Bischoff A, Peña A, Runck LA & Guasch G. (2014). The great divide: septation and malformation of the cloaca, and its implications for surgeons. Pediatr. Surg. Int. , 30, 1089-95. PMID: 25217828 DOI.
Kluth D. (2010). Embryology of anorectal malformations. Semin. Pediatr. Surg. , 19, 201-8. PMID: 20610193 DOI.
Hynes PJ & Fraher JP. (2004). The development of the male genitourinary system. I. The origin of the urorectal septum and the formation of the perineum. Br J Plast Surg , 57, 27-36. PMID: 14672675
Marshall FF. (1978). Embryology of the lower genitourinary tract. Urol. Clin. North Am. , 5, 3-15. PMID: 347662
Articles
Qian C, Wu Z, Ng RC, Garcia-Barceló MM, Yuan ZW, Wong KKY, Tam PKH & Lui VCH. (2018). Conditional deletion of platelet derived growth factor receptor alpha (Pdgfra) in urorectal mesenchyme causes mesenchyme apoptosis and urorectal developmental anomalies in mice. Cell Death Differ. , , . PMID: 30323271 DOI.
Tang XB, Li H, Zhang J, Wang WL, Yuan ZW & Bai YZ. (2018). Expression pattern of Wif1 and β-catenin during development of anorectum in fetal rats with anorectal malformations. PeerJ , 6, e4445. PMID: 29507836 DOI.
Hoshi M, Reginensi A, Joens MS, Fitzpatrick JAJ, McNeill H & Jain S. (2018). Reciprocal Spatiotemporally Controlled Apoptosis Regulates Wolffian Duct Cloaca Fusion. J. Am. Soc. Nephrol. , 29, 775-783. PMID: 29326158 DOI.
Tang XB, Zhang T, Wang WL, Yuan ZW & Bai YZ. (2016). Spatiotemporal distribution of caudal-type homeobox proteins during development of the hindgut and anorectum in human embryos. PeerJ , 4, e1771. PMID: 27042391 DOI.
Huang YC, Chen F & Li X. (2016). Clarification of mammalian cloacal morphogenesis using high-resolution episcopic microscopy. Dev. Biol. , 409, 106-113. PMID: 26485363 DOI.
Sasaki C, Yamaguchi K & Akita K. (2004). Spatiotemporal distribution of apoptosis during normal cloacal development in mice. Anat Rec A Discov Mol Cell Evol Biol , 279, 761-7. PMID: 15278947 DOI.
Nievelstein RA, van der Werff JF, Verbeek FJ, Valk J & Vermeij-Keers C. (1998). Normal and abnormal embryonic development of the anorectum in human embryos. Teratology , 57, 70-8. PMID: 9562679 <70::AID-TERA5>3.0.CO;2-A DOI.
Historic
Ludwig KS. (1965). [On the relation of the cloacal membrane and the urorectal septum in human embryos of 9-33 mm SSL]. Z Anat Entwicklungsgesch , 124, 401-13. PMID: 5832420
SCOTT JE & SWENSON O. (1959). Imperforate anus: results in 63 cases and some anatomic considerations. Ann. Surg. , 150, 477-87. PMID: 14444236
Felix W. The development of the urinogenital organs. In Keibel F. and Mall FP. Manual of Human Embryology II. (1912) J. B. Lippincott Company, Philadelphia. pp 752-979.
Search Pubmed
Search Bookshelf Cloaca Development
Search Pubmed Now: Cloaca Development | Cloacal Membrane
Additional Images
Historic
| Historic Disclaimer - information about historic embryology pages
|
| Pages where the terms "Historic" (textbooks, papers, people, recommendations) appear on this site, and sections within pages where this disclaimer appears, indicate that the content and scientific understanding are specific to the time of publication. This means that while some scientific descriptions are still accurate, the terminology and interpretation of the developmental mechanisms reflect the understanding at the time of original publication and those of the preceding periods, these terms, interpretations and recommendations may not reflect our current scientific understanding. (More? Embryology History | Historic Embryology Papers)
|
Bremer JL. Description of a 4-mm human embryo. (1906) Amer. J Anat. 5: 459-480.

Fig.8. Section through body of Harvard Embryo Template:HE714 near the cloaca.
Felix W. The development of the urinogenital organs. In Keibel F. and Mall FP. Manual of Human Embryology II. (1912) J. B. Lippincott Company, Philadelphia. pp 752-979.
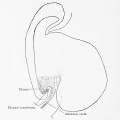
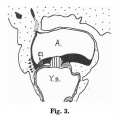
Fig. 599. Embryo Pfannenstiel-Kromer, 1.38 mm long, 5-6 somites, shows relation of cloaca and cloacal membrane to allantoic stalk.
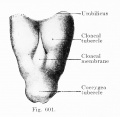
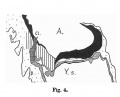
Fig. 600. Embryo Pfannenstiel III 2.6 mm GL 13-14 somites, allantoic stalk is given off at a right angle from the cloaca, immediately above cloacal membrane. Ventral wall of the cloaca is formed only by the cloacal membrane.
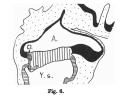
Fig. 601. Cloacal membrane human embryo 3 mm GL (Embryo E. B.) forms a rhomboidal groove slightly depressed below the surface of the embryo, between the umbilicus and the coccygeal tubercle.
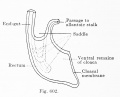
Fig. 602. Cloaca human embryo 7 mm GL (embryo Chr. I), separation of the rectum from the ventral remains of the cloaca is shown
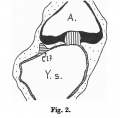
Fig. 603 a and b. Human embryo 7 mm GL (Embryo Chr. I) division of cloaca into rectum and ventral remains of the cloaca is almost complete, the saddle between the two being immediately over the cloacal membrane.
Fig. 604 a and b. Human embryo 11 mm GL (Embryo P. I.) The rectum is completely separated from the ventral remains of the cloaca, and the cloacal membrane has been divided into the canal and urogenital membranes.
Fig. 605. Human embryo 5.3 mm GL (Embryo 1420) Primary excretory duct and opening with reference to cloaca and cloacal membrane, anlage of ureteric bud.
Fig. 606. Human embryo 4.25 mm vertex-breech length, 28 somites (Embryo H. M. 1) Primary excretory duct and position of orifice relatively to cloaca and cloacal membrane.
Fig. 607. Human embryo 18 mm Between the umbilicus and the coccygeal tubercle cranio-caudally and the two lower extremities laterally, the cloacal tubercle has appeared.
Florian J. The early development of man, with special reference to the development of the mesoderm and cloacal membrane. (1933) J. Anat., 67(2): 263-76. PMID 17104422
Terms
- cloacal duct of Reichel - Reichel P. The development of the bladder and urinary tubes (Die Entwicklung der Harnblase und der Harnrohre), (1893) Verb. phys. med. Gesellsch. Wiirzburg.
- cloacal tubercle - (genital tubercle)
| Gastrointestinal Tract Terms
|
- allantois - An extraembryonic membrane, endoderm in origin extension from the early hindgut, then cloaca into the connecting stalk of placental animals, connected to the superior end of developing bladder. In reptiles and birds, acts as a reservoir for wastes and mediates gas exchange. In mammals is associated/incorporated with connecting stalk/placental cord fetal-maternal interface.
- amnion - An extra-embryonic membrane, ectoderm and extraembryonic mesoderm in origin, also forms the innermost fetal membrane, that produces amniotic fluid. This fluid-filled sac initially lies above the trilaminar embryonic disc and with embryoic disc folding this sac is drawn ventrally to enclose (cover) the entire embryo, then fetus. The presence of this membrane led to the description of reptiles, bird, and mammals as amniotes.
- amniotic fluid - The fluid that fills amniotic cavity totally encloses and cushions the embryo. Amniotic fluid enters both the gastrointestinal and respiratory tract following rupture of the buccopharyngeal membrane. The late fetus swallows amniotic fluid.
- atresia - is an abnormal interruption of the tube lumen, the abnormality naming is based upon the anatomical location.
- buccal - (Latin, bucca = cheek) A term used to relate to the mouth (oral cavity).
- bile salts - Liver synthesized compounds derived from cholesterol that function postnatally in the small intestine to solubilize and absorb lipids, vitamins, and proteins. These compounds act as water-soluble amphipathic detergents. liver
- buccopharyngeal membrane - (oral membrane) (Latin, bucca = cheek) A membrane which forms the external upper membrane limit (cranial end) of the early gastrointestinal tract. This membrane develops during gastrulation by ectoderm and endoderm without a middle (intervening) layer of mesoderm. The membrane lies at the floor of the ventral depression (stomodeum) where the oral cavity will open and will breakdown to form the initial "oral opening" of the gastrointestinal tract. The equivilent membrane at the lower end of the gastrointestinal tract is the cloacal membrane.
- celiac artery - (celiac trunk) main blood supply to the foregut, excluding the pharynx, lower respiratory tract, and most of the oesophagus.
- cholangiocytes - epithelial cells that line the intra- and extrahepatic ducts of the biliary tree. These cells modify the hepatocyte-derived bile, and are regulated by hormones, peptides, nucleotides, neurotransmitters, and other molecules. liver
- cloaca - (cloacal cavity) The term describing the common cavity into which the intestinal, genital, and urinary tracts open in vertebrates. Located at the caudal end of the embryo it is located on the surface by the cloacal membrane. In many species this common cavity is later divided into a ventral urogenital region (urogenital sinus) and a dorsal gastrointestinal (rectal) region.
- cloacal membrane - Forms the external lower membrane limit (caudal end) of the early gastrointestinal tract (GIT). This membrane is formed during gastrulation by ectoderm and endoderm without a middle (intervening) layer of mesoderm. The membrane breaks down to form the initial "anal opening" of the gastrointestinal tract.
- coelomic cavity - (coelom) Term used to describe a space. There are extra-embryonic and intra-embryonic coeloms that form during vertebrate development. The single intra-embryonic coelom forms the 3 major body cavities: pleural cavity, pericardial cavity and peritoneal cavity.
- crypt of Lieberkühn - (intestinal gland, intestinal crypt) intestinal villi epithelia extend down into the lamina propria where they form crypts that are the source of epithelial stem cells and immune function.
- duplication - is an abnormal incomplete tube recanalization resulting in parallel lumens, this is really a specialized form of stenosis. (More? Image - small intestine duplication)
- esophageal - (oesophageal)
- foregut - first embryonic division of gastrointestinal tract extending from the oral (buccopharyngeal) membrane and contributing oesophagus, stomach, duodenum (to bile duct opening), liver, biliary apparatus (hepatic ducts, gallbladder, and bile duct), and pancreas. The forgut blood supply is the celiac artery (trunk) excluding the pharynx, lower respiratory tract, and most of the oesophagus.
- galactosemia - Metabolic abnormality where the simple sugar galactose (half of lactose, the sugar in milk) cannot be metabolised. People with galactosemia cannot tolerate any form of milk (human or animal). Detected by the Guthrie test.
- gastric transposition - clinical term for postnatal surgery treatment for esophageal atresia involving esophageal replacement. Typically performed on neonates between day 1 to 4. (More? gastrointestinal abnormalities | PMID 28658159
- gastrointestinal divisions - refers to the 3 embryonic divisions contributing the gastrointestinal tract: foregut, Midgut and hindgut.
- gastrula - (Greek, gastrula = little stomach) A stage of an animal embryo in which the three germ layers (endoderm/mesoderm/ectoderm) have just formed. All of these germ layers have contributions to the gastrointestinal tract.
- gastrulation - The process of differentiation forming a gastrula. Term means literally means "to form a gut" but is more in development, as this process converts the bilaminar embryo (epiblast/hypoblast) into the trilaminar embryo (endoderm/mesoderm/ectoderm) establishing the 3 germ layers that will form all the future tissues of the entire embryo. This process also establishes the the initial body axes. (More? gastrulation)
- Guthrie test - (heel prick) A neonatal blood screening test developed by Dr Robert Guthrie (1916-95) for determining a range of metabolic disorders and infections in the neonate. (More? Guthrie test)
- heterotaxia - (Greek heteros = different; taxis = arrangement) is the right/left transposition of thoracic and/or abdominal organs.
- hindgut - final embryonic division of gastrointestinal tract extending to the cloacal membrane and contributing part of the transverse colon (left half to one third), descending colon, sigmoid colon, rectum, part of anal canal (superior), urinary epithelium (bladder and most urethra). The hindgut blood supply is the inferior mesenteric artery.
- inferior mesenteric artery - main blood supply to the hindgut
- intestine - (bowel) part of the gastrointestinal tract (GIT) lying between the stomach and anus where absorption of nutrients and water occur. This region is further divided anatomically and functionally into the small intestine or bowel (duodenum, jejunum and ileum) and large intestine or bowel (cecum and colon).
- intestinal perforation - gastrointestinal abnormality identified in neonates can be due to necrotizing enterocolitis, Hirschsprung’s disease or meconium ileus.
- intraembryonic coelom - The "horseshoe-shaped" space (cavity) that forms initially in the third week of development in the lateral plate mesoderm that will eventually form the 3 main body cavities: pericardial, pleural, peritoneal. The intraembryonic coelom communicates transiently with the extraembryonic coelom.
- meconium ileus intestine obstruction within the ileum due to abnormal meconium properties.
- mesentery - connects gastrointestinal tract to the posterior body wall and is a double layer of visceral peritoneum.
- mesothelium - The mesoderm derived epithelial covering of coelomic organs and also line their cavities.
- Midgut - middle embryonic division of gastrointestinal tract contributing the small intestine (including duodenum distal bile duct opening), cecum, appendix, ascending colon, and part of the transverse colon (right half to two thirds). The midgut blood supply is the superior mesenteric artery.
- neuralation - The general term used to describe the early formation of the nervous system. It is often used to describe the early events of differentiation of the central ectoderm region to form the neural plate, then neural groove, then neural tube. The nervous system includes the central nervous system (brain and spinal cord) from the neural tube and the peripheral nervous system (peripheral sensory and sympathetic ganglia) from neural crest. In humans, early neuralation begins in week 3 and continues through week 4.
- neural crest - region of cells at the edge of the neural plate that migrates throughout the embryo and contributes to many different tissues. In the gastrointestinal tract it contributes mainly the enteric nervous system within the wall of the gut responsible for peristalsis and secretion.
- peritoneal stomata - the main openings forming the pathways for drainage of intra-peritoneal fluid from the peritoneal cavity into the lymphatic system.
- pharynx - uppermost end of gastrointestinal and respiratory tract, in the embryo beginning at the buccopharyngeal membrane and forms a major arched cavity within the phrayngeal arches.
- recanalization - describes the process of a hollow structure becoming solid, then becoming hollow again. For example, this process occurs during GIT, auditory and renal system development.
- retroperitoneal - (retroperitoneum) is the anatomical space (sometimes a potential space) in the abdominal cavity behind (retro) the peritoneum. Developmentally parts of the GIT become secondarily retroperitoneal (part of duodenum, ascending and descending colon, pancreas)
- somitogenesis The process of segmentation of the paraxial mesoderm within the trilaminar embryo body to form pairs of somites, or balls of mesoderm. A somite is added either side of the notochord (axial mesoderm) to form a somite pair. The segmentation does not occur in the head region, and begins cranially (head end) and extends caudally (tailward) adding a somite pair at regular time intervals. The process is sequential and therefore used to stage the age of many different species embryos based upon the number visible somite pairs. In humans, the first somite pair appears at day 20 and adds caudally at 1 somite pair/4 hours (mouse 1 pair/90 min) until on average 44 pairs eventually form.
- splanchnic mesoderm - Gastrointestinal tract (endoderm) associated mesoderm formed by the separation of the lateral plate mesoderm into two separate components by a cavity, the intraembryonic coelom. Splanchnic mesoderm is the embryonic origin of the gastrointestinal tract connective tissue, smooth muscle, blood vessels and contribute to organ development (pancreas, spleen, liver). The intraembryonic coelom will form the three major body cavities including the space surrounding the gut, the peritoneal cavity. The other half of the lateral plate mesoderm (somatic mesoderm) is associated with the ectoderm of the body wall.
- stomodeum - (stomadeum, stomatodeum) A ventral surface depression on the early embryo head surrounding the buccopharyngeal membrane, which lies at the floor of this depression. This surface depression lies between the maxillary and mandibular components of the first pharyngeal arch.
- stenosis - abnormal a narrowing of the tube lumen, the abnormality naming is based upon the anatomical location.
- superior mesenteric artery - main blood supply to the Midgut.
- viscera - the internal organs in the main cavities of the body, especially those in the abdomen, for example the Template:Intestines.
- visceral peritoneum - covers the external surfaces of the intestinal tract and organs within the peritoneum. The other component (parietal peritoneum) lines the abdominal and pelvic cavity walls.
- yolk sac - An extraembryonic membrane which is endoderm origin and covered with extraembryonic mesoderm. Yolk sac lies outside the embryo connected initially by a yolk stalk to the midgut with which it is continuous with. The endodermal lining is continuous with the endoderm of the gastrointestinal tract. The extra-embryonic mesoderm differentiates to form both blood and blood vessels of the vitelline system. In reptiles and birds, the yolk sac has a function associated with nutrition. In mammals the yolk sac acts as a source of primordial germ cells and blood cells. Note that in early development (week 2) a structure called the "primitive yolk sac" forms from hypoblast, this is an entirely different structure.
- yolk stalk - (vitelline duct, omphalomesenteric duct, Latin, vitellus = yolk of an egg) The endodermal connection between the midgut and the yolk sac. See vitelline duct.
|
|
|
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, June 21) Embryology Cloaca Development. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Cloaca_Development
- What Links Here?
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G