Cardiovascular System - Patent Ductus Arteriosus
| Embryology - 14 Jun 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Introduction

International Classification of Diseases (ICD-10) - Q25 Congenital malformations of great arteries Q25.0 Patent ductus arteriosus Patent ductus Botallo Persistent ductus arteriosus
Patent ductus arteriosus (PDA), or Patent arterial duct (PAD), or common truncus, occurs commonly in preterm infants, and at approximately 1 in 2000 full term infants and more common in females (to male ratio is 2:1). Can also be associated with specific genetic defects, trisomy 21 and trisomy 18, and the Rubinstein-Taybi and CHARGE syndromes.
The opening is asymptomatic when the duct is small and can close spontaneously (by day three in 60% of normal term neonates), the remainder are ligated simply and with little risk, with transcatheter closure of the duct generally indicated in older children. The operation is always recommended even in the absence of cardiac failure and can often be deferred until early childhood.
- The ductus arteriosus, and its corresponding ligament, historically were described as the ductus Botallo, but should this have really been the ductus Aranzio?[1]
Some Recent Findings

|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Patent Ductus Arteriosus <pubmed limit=5>Patent Ductus Arteriosus</pubmed> |
Diagnostic Images

PDA echocardiogram
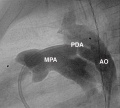
PDA angiogram

PDA computed tomography



Cardiovascular Abnormalities

Heart defects and preterm birth are the most common causes of neonatal and infant death. The long-term development of the heart combined with extensive remodelling and post-natal changes in circulation lead to an abundance of abnormalities associated with this system.
A UK study literature showed that preterm infants have more than twice as many cardiovascular malformations (5.1 / 1000 term infants and 12.5 / 1000 preterm infants) as do infants born at term and that 16% of all infants with cardiovascular malformations are preterm. (0.4% of live births occur at greater than 28 weeks of gestation, 0.9% at 28 to 31 weeks, and 6% at 32 to 36 weeks. Overall, 7.3% of live-born infants are preterm)[5]
"Baltimore-Washington Infant Study data on live-born cases and controls (1981-1989) was reanalyzed for potential environmental and genetic risk-factor associations in complete atrioventricular septal defects AVSD (n = 213), with separate comparisons to the atrial (n = 75) and the ventricular (n = 32) forms of partial AVSD. ...Maternal diabetes constituted a potentially preventable risk factor for the most severe, complete form of AVSD." [6]
In addition, there are in several congenital abnormalities that exist in adults (bicuspid aortic valve, mitral valve prolapse, and partial anomalous pulmonary venous connection) which may not be clinically recognized.
International Classification of Diseases
The International Classification of Diseases (ICD) World Health Organization's classification used worldwide as the standard diagnostic tool for epidemiology, health management and clinical purposes. This includes the analysis of the general health situation of population groups. It is used to monitor the incidence and prevalence of diseases and other health problems. Within this classification "congenital malformations, deformations and chromosomal abnormalities" are (Q00-Q99) but excludes "inborn errors of metabolism" (E70-E90).
Congenital malformations of the circulatory system (Q20-Q28)
International Classification of Diseases (ICD-10) - Q25 Congenital malformations of great arteries Q25.0 Patent ductus arteriosus Patent ductus Botallo Persistent ductus arteriosus
Clinical Classifications
Patent Ductus Arteriosus (PDA) classification system on the basis of angiogram appearance by Krichenko (1989).[7]
|

|
A recent publication suggests a classification based on angiographic size and haemodynamic sound significance.[8]
| Type | Size | Haemodynamics |
|---|---|---|
| Silent PDA | usually less than 1.5 mm | PDA murmur not present |
| Very small PDA | less than 1.5 mm | PDA murmur present |
| Small PDA | 1.5 to 3.0 mm | PDA murmur present |
| Moderate PDA | 3 to 5 mm | PDA murmur present |
| Large PDA | greater than 5 mm | PDA murmur present |
The Aristotle Comprehensive Complexity (ACC) score has been suggested as a clinical tool for complexity adjustment in the analysis of outcome after reparative congenital heart surgery.[9][10]
References
Reviews
<pubmed>21532100</pubmed>
Articles
<pubmed>21829408</pubmed> <pubmed>21532789</pubmed>
Search Pubmed
Search Pubmed: Patent Ductus Arteriosus
Search OMIM: Patent Ductus Arteriosus
External Links
External Links Notice - The dynamic nature of the internet may mean that some of these listed links may no longer function. If the link no longer works search the web with the link text or name. Links to any external commercial sites are provided for information purposes only and should never be considered an endorsement. UNSW Embryology is provided as an educational resource with no clinical information or commercial affiliation.
- MedlinePlus Patent Ductus Arteriosus
- OMIM 607411 Patent Ductus Arteriosus
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, June 14) Embryology Cardiovascular System - Patent Ductus Arteriosus. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Cardiovascular_System_-_Patent_Ductus_Arteriosus
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G