Cloaca Development: Difference between revisions
mNo edit summary |
mNo edit summary |
||
| (10 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{Header}} | '''Bold text'''{{Header}} | ||
==Introduction== | ==Introduction== | ||
[[File:Stage12 sem9 cloacal membrane.jpg|alt=Carnegie stage 12 cloacal membrane|thumb|Human Embryo stage {{CS12}} cloacal membrane (SEM}]] | [[File:Stage12 sem9 cloacal membrane.jpg|alt=Carnegie stage 12 cloacal membrane|thumb|Human Embryo stage {{CS12}} cloacal membrane (SEM}]] | ||
The initial {{cloaca}} is the common early endoderm lined space of the {{hindgut}} that will later become partitioned by a septum into a dorsal gastrointestinal component (rectum) and ventral renal/genital component (urogenital sinus). Note that the cloaca in mammals is an early embryonic transient structure and only persists in birds and reptiles. Located at the superior end of the cloaca is the {{allantois}}, that extends into the connecting stalk and later the placental cord. Located at the inferior end of the cloaca is the cloacal membrane, that also forms part of the embryo surface. | The initial {{cloaca}} is the common early endoderm lined space of the {{hindgut}} that will later become partitioned by a septum into a dorsal gastrointestinal component (rectum) and ventral renal/genital component (urogenital sinus). Note that the cloaca in mammals is an early embryonic transient structure and only persists in birds and reptiles. Located at the superior end of the cloaca is the {{allantois}}, that extends into the connecting stalk and later the placental cord. Located at the inferior end of the cloaca is the {{cloacal membrane}}, that also forms part of the embryo surface. | ||
The gastrointestinal tract ends at this cloacal membrane, equivalent to the beginning of the tract at the buccopharyngeal membrane at the upper end. The cloacal membrane is formed during gastrulation by {{ectoderm}} and {{endoderm}} without a middle (intervening) layer of {{mesoderm}}, that later degenerates after cloacal septation. | The gastrointestinal tract ends at this cloacal membrane, equivalent to the beginning of the tract at the buccopharyngeal membrane at the upper end. The cloacal membrane is formed during gastrulation by {{ectoderm}} and {{endoderm}} without a middle (intervening) layer of {{mesoderm}}, that later degenerates by {{apoptosis}} after cloacal septation. | ||
| Line 12: | Line 12: | ||
:'''Links:''' {{cloaca}} | {{Intestine}} | {{bladder}} | {{genital}} | :'''Links:''' {{cloaca}} | {{Intestine}} | {{bladder}} | {{genital}} | {{apoptosis}} | ||
:: [[Historic Embryology Papers|Historic papers]]: [[Paper - The development of the cloaca in human embryos|1911 human cloaca]] | [[Book_-_Manual_of_Human_Embryology_19-1#Cloaca.2C_Bladder.2C_Urethra.2C_and_Urogenital_Sinus|1912 Cloaca, Bladder, Urethra, and Urogenital Sinus]] | [[Paper - The Early Development of Man, with Special Reference to the Development of the Mesoderm and Cloacal Membrane|1933 Cloacal Membrane]] | [[Paper - Congenital hernia into the umbilical cord - two cases, one associated with persistent cloaca|1938 persistent cloaca]] | :: [[Historic Embryology Papers|Historic papers]]: [[Paper - The development of the cloaca in human embryos|1911 human cloaca]] | [[Book_-_Manual_of_Human_Embryology_19-1#Cloaca.2C_Bladder.2C_Urethra.2C_and_Urogenital_Sinus|1912 Cloaca, Bladder, Urethra, and Urogenital Sinus]] | [[Paper - The Early Development of Man, with Special Reference to the Development of the Mesoderm and Cloacal Membrane|1933 Cloacal Membrane]] | [[Paper - Congenital hernia into the umbilical cord - two cases, one associated with persistent cloaca|1938 persistent cloaca]] | ||
<br> | <br> | ||
| Line 30: | Line 30: | ||
| | | | ||
* '''The development of the cloaca in the human embryo'''{{#pmid:30294789|PMID30294789}} "Subdivision of cloaca into urogenital and anorectal passages has remained controversial because of disagreements about the identity and role of the septum developing between both passages. This study aimed to clarify the development of the cloaca using a quantitative 3D morphological approach in human embryos of 4-10 post-fertilisation weeks. ...Our main finding was a pronounced difference in growth between rapidly expanding central and ventral parts, and slowly or non-growing cranial and dorsal parts. The entrance of the Wolffian duct into the cloaca proved a stable landmark that remained linked to the position of vertebra S3. Suppressed growth in the cranial cloaca resulted in an apparent craniodorsal migration of the entrance of the Wolffian duct, while suppressed growth in the dorsal cloaca changed the entrance of the hindgut from cranial to dorsal on the cloaca. Transformation of this 'end-to-end' into an 'end-to-side' junction produced temporary 'lateral (Rathke's) folds'. The persistent difference in dorsoventral growth straightened the embryonic caudal body axis and concomitantly extended the frontally oriented 'urorectal (Tourneux's) septum' caudally between the ventral urogenital and dorsal anorectal parts of the cloaca. The dorsoventral growth difference also divided the cloacal membrane into a well-developed ventral urethral plate and a thin dorsal cloacal membrane proper, which ruptured at 6.5 weeks. The expansion of the pericloacal mesenchyme followed the dorsoventral growth difference and produced the genital tubercle. Dysregulation of dorsal cloacal development is probably an important cause of anorectal malformations: too little regressive development may result in anorectal agenesis, and too much regression in stenosis or atresia of the remaining part of the dorsal cloaca." (see also historic [[Paper - The development of the cloaca in human embryos|1911 paper]]) | * '''The development of the cloaca in the human embryo'''{{#pmid:30294789|PMID30294789}} "Subdivision of cloaca into urogenital and anorectal passages has remained controversial because of disagreements about the identity and role of the septum developing between both passages. This study aimed to clarify the development of the cloaca using a quantitative 3D morphological approach in human embryos of 4-10 post-fertilisation weeks. ...Our main finding was a pronounced difference in growth between rapidly expanding central and ventral parts, and slowly or non-growing cranial and dorsal parts. The entrance of the Wolffian duct into the cloaca proved a stable landmark that remained linked to the position of vertebra S3. Suppressed growth in the cranial cloaca resulted in an apparent craniodorsal migration of the entrance of the Wolffian duct, while suppressed growth in the dorsal cloaca changed the entrance of the hindgut from cranial to dorsal on the cloaca. Transformation of this 'end-to-end' into an 'end-to-side' junction produced temporary 'lateral (Rathke's) folds'. The persistent difference in dorsoventral growth straightened the embryonic caudal body axis and concomitantly extended the frontally oriented 'urorectal (Tourneux's) septum' caudally between the ventral urogenital and dorsal anorectal parts of the cloaca. The dorsoventral growth difference also divided the cloacal membrane into a well-developed ventral urethral plate and a thin dorsal cloacal membrane proper, which ruptured at 6.5 weeks. The expansion of the pericloacal mesenchyme followed the dorsoventral growth difference and produced the genital tubercle. Dysregulation of dorsal cloacal development is probably an important cause of anorectal malformations: too little regressive development may result in anorectal agenesis, and too much regression in stenosis or atresia of the remaining part of the dorsal cloaca." (see also historic [[Paper - The development of the cloaca in human embryos|1911 paper]]) | ||
|} | |} | ||
{| class="wikitable mw-collapsible mw-collapsed" | {| class="wikitable mw-collapsible mw-collapsed" | ||
| Line 37: | Line 37: | ||
| [[File:Mark_Hill.jpg|90px|left]] {{Most_Recent_Refs}} | | [[File:Mark_Hill.jpg|90px|left]] {{Most_Recent_Refs}} | ||
Search term: [http://www.ncbi.nlm.nih.gov/pubmed/?term=Cloaca ''Cloaca''] | Search term: [http://www.ncbi.nlm.nih.gov/pubmed/?term=Cloaca ''Cloaca''] | [http://www.ncbi.nlm.nih.gov/pubmed/?term=Cloacal+Membrane ''Cloacal Membrane''] | ||
|} | |} | ||
{| class="wikitable mw-collapsible mw-collapsed" | {| class="wikitable mw-collapsible mw-collapsed" | ||
| Line 49: | Line 44: | ||
|- | |- | ||
| {{Older papers}} | | {{Older papers}} | ||
* '''Clarification of mammalian cloacal morphogenesis using high-resolution episcopic microscopy'''{{#pmid:26485363|PMID26485363}} "The developmental process through which the cloaca transforms from one hollow structure to two separated urinary and digestive outlets remains controversial and speculative. Here, we use high-resolution episcopic microscopy to examine a comprehensive series of normal and mutant {{mouse}} cloaca in which the detailed 3-dimensional (3-D) morphological features are illuminated throughout the development. We provide evidence that the dorsal peri-cloacal mesenchyme (dPCM) remains stationary while other surrounding tissues grow towards it. This causes dramatic changes of spatial relationship among caudal structures and morphological transformation of the cloaca. The 3-D characterizations of Dkk1 mutants reveal a hyperplastic defect of dPCM, which leads to a significant anterior shift of the caudal boundary of the cloaca, premature occlusion of the cloaca and, imperforate anus phenotype. Conversely, {{Shh}} knockout causes a severe hypoplastic defect of cloaca mesenchyme including dPCM and persistent cloaca. Collectively, these findings suggest that formation of the dPCM is critical for cloacal morphogenesis and furthermore, growth and movement of the mesenchymal tissues towards the dPCM lead to the cloaca occlusion and separation of the urinary and digestive outlets." | |||
|} | |} | ||
==Movies== | ==Movies== | ||
{| | {| | ||
| Line 69: | Line 66: | ||
|} | |} | ||
:'''Links:''' [[Carnegie stage 10]] | [[Model Embryo 3.1mm Movie 1|Stage 10 Movie]] | :'''Links:''' [[Carnegie stage 10]] | [[Model Embryo 3.1mm Movie 1|Stage 10 Movie]] | ||
===Stage 11=== | ===Stage 11=== | ||
{| | {| | ||
| Line 79: | Line 77: | ||
File:Stage12 sem9.jpg | File:Stage12 sem9.jpg | ||
File:Stage12 sem9 cloacal membrane.jpg | File:Stage12 sem9 cloacal membrane.jpg | ||
<gallery> | </gallery> | ||
:'''Links:''' [[Carnegie stage 12]] | :'''Links:''' [[Carnegie stage 12]] | ||
| Line 92: | Line 90: | ||
===Stage 22=== | ===Stage 22=== | ||
==Animal Model== | |||
See this recent analysis of {{mouse}} cloacal morphogenesis using high-resolution episcopic microscopy.{{#pmid:26485363|PMID26485363}} | |||
* [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4688061/bin/NIHMS734311-supplement-2.mp4 Video 1. Figure S2.] The 3-D images of the entire mouse cloaca morphogenetic process from {{ME9.5}} to {{ME13.5}}. | |||
==Molecular== | |||
===Sonic Hedgehog=== | |||
In the {{mouse}} model of cloacal development, {{Shh}} knockout causes a severe hypoplastic defect of cloaca mesenchyme including dorsal peri-cloacal mesenchyme and persistent cloaca.{{#pmid:26485363|PMID26485363}} | |||
:'''Links:''' {{SHH}} | |||
===Apoptosis=== | |||
{{apoptosis}} - process of cell death required for the removal of the cloacal membrane. | |||
==Abnormalities== | ==Abnormalities== | ||
{{ICD-11}} LB17 Structural developmental anomalies of anal canal | |||
* [https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/2131510660 LB17.2 Persistent cloaca] | |||
* [https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/2004612103 LB17.3 Cloacal exstrophy] | |||
* [https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/2020658461 GC04.19 Combined urinary and rectal fistula including cloaca with severe scar or extensive tissue loss] | |||
===Persistent Cloaca=== | |||
{{ICD-11}} [https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/2131510660 LB17.2 Persistent cloaca] is a congenital anomaly in which the intestinal, urinary, and reproductive ducts open into a common cavity, a result of the failure of the urorectal septum to form during prenatal development. They occur exclusively in girls and comprise the most complex defect in the spectrum of anorectal malformations. | |||
{| | {| | ||
|+ Persistent Cloaca Perineum{{#pmid:17651510|PMID17651510}} | |+ Persistent Cloaca Perineum{{#pmid:17651510|PMID17651510}} | ||
| Line 103: | Line 122: | ||
|} | |} | ||
:'''Links:''' [[Gastrointestinal Tract - Abnormalities|GIT Abnormalities]] | :'''Links:''' [https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/2131510660 LB17.2 Persistent cloaca] | [[Gastrointestinal Tract - Abnormalities|GIT Abnormalities]] | ||
===Cloacal Exstrophy=== | ===Cloacal Exstrophy=== | ||
{{ICD-11}} [https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/2004612103 LB17.3 Cloacal exstrophy] a rare (about 1/200,000{{#pmid:19878548|PMID19878548}}) and complex anorectal and genitourinary malformation in which rectum, vagina and urinary tract share a common everted orifice, accompanied by an {{omphalocele}} and an imperforate anus. Exstrophy of the cloaca is a well-known malformation that includes the persistence and the exstrophy of a cloaca that receives ureters, ileum and a rudimentary hindgut. Cloacal exstrophy is a severe birth defect wherein much of the abdominal organs (the bladder and intestines) are exposed. It often causes the splitting of both male and female genitalia (specifically, the penis and clitoris respectively), and the anus is occasionally sealed. | |||
:'''Links:''' [https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/2004612103 LB17.3 Cloacal exstrophy] | |||
===OEIS Complex=== | |||
Omphalocele-Exstrophy-Imperforate Anus-Spinal (OEIS) defects, a combination of defects comprising omphalocele, exstrophy of the cloaca, imperforate anus, and spinal defects. | |||
OMIM: [https://omim.org/entry/258040 OEIS Complex] | |||
| Line 116: | Line 144: | ||
===Reviews=== | ===Reviews=== | ||
{{#pmid:30367985}} | {{#pmid:30367985}} | ||
{{#pmid:26969227}} | |||
{{#pmid:25217828}} | {{#pmid:25217828}} | ||
| Line 141: | Line 171: | ||
{{#pmid:9562679}} | {{#pmid:9562679}} | ||
===Historic=== | |||
{{#pmid:5832420}} | |||
{{#pmid:14444236}} | {{#pmid:14444236}} | ||
{{Ref-PrentissArey1918}} [[Book_-_A_Laboratory_Manual_and_Text-book_of_Embryology_8#Differentiation_of_Cloaca.2C_Bladder.2C_Urethra_and_Urogenital_Sinus|Differentiation of Cloaca, Bladder, Urethra and Urogenital Sinus]] | |||
{{Ref-Felix1912}} | {{Ref-Felix1912}} | ||
| Line 185: | Line 218: | ||
<gallery> | <gallery> | ||
File:Florian1933 fig01.jpg|Fig.1 | File:Florian1933 fig01.jpg|Fig.1 | ||
File:Florian1933 | File:Florian1933 fig02.jpg|Fig.2 | ||
File:Florian1933 | File:Florian1933 fig03.jpg|Fig.3 | ||
File:Florian1933 | File:Florian1933 fig04.jpg|Fig.4 | ||
File:Florian1933 | File:Florian1933 fig05.jpg|Fig.5 | ||
File:Florian1933 | File:Florian1933 fig06.jpg|Fig.6 | ||
File:Florian1933 | File:Florian1933 fig07.jpg|Fig.7 | ||
File:Florian1933 | File:Florian1933 fig08.jpg|Fig.8 | ||
</gallery> | </gallery> | ||
Latest revision as of 14:17, 17 April 2019
Bold text
| Embryology - 16 Jun 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Introduction

The initial cloaca is the common early endoderm lined space of the hindgut that will later become partitioned by a septum into a dorsal gastrointestinal component (rectum) and ventral renal/genital component (urogenital sinus). Note that the cloaca in mammals is an early embryonic transient structure and only persists in birds and reptiles. Located at the superior end of the cloaca is the allantois, that extends into the connecting stalk and later the placental cord. Located at the inferior end of the cloaca is the cloacal membrane, that also forms part of the embryo surface.
The gastrointestinal tract ends at this cloacal membrane, equivalent to the beginning of the tract at the buccopharyngeal membrane at the upper end. The cloacal membrane is formed during gastrulation by ectoderm and endoderm without a middle (intervening) layer of mesoderm, that later degenerates by apoptosis after cloacal septation.
The hindgut component will contribute to the gastrointestinal tract intestine of the distal transverse colon, descending colon, sigmoid colon, rectum.
The urogenital sinus component will contribute the renal urinary bladder and participate in genital development.
Some Recent Findings
|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Cloaca | Cloacal Membrane |
| Older papers |
|---|
| These papers originally appeared in the Some Recent Findings table, but as that list grew in length have now been shuffled down to this collapsible table.
See also the Discussion Page for other references listed by year and References on this current page.
|
Movies
| Early Endoderm | Week 3 Folding |
|---|---|
| <html5media height="400" width="350">File:Amnion 001.mp4</html5media> | <html5media height="500" width="350">File:Week3_folding.mp4</html5media> |
- Links: Early Endoderm Movie | Week 3 Folding Movie
Embryonic Development
Stage 10

|

|
Caudal end of embryo showing primitive streak region, cloacal membrane, and connecting stalk. |
- Links: Carnegie stage 10 | Stage 10 Movie
Stage 11

|
Historic image<ref name=Low1908>Low A. Description of a human embryo of 13-14 mesodermic somites. (1908) J Anat Physiol. 42(3): 237-51. PMID 17232769 | PMC1289161 of an embryo model (sagittal section, viewed from the left) showing hindgut and cloaca. |
- Links: Carnegie stage 11
Stage 12

- Links: Carnegie stage 12
Stage 13
| <html5media height="420" width="400">File:Stage13 GIT3d.mp4</html5media> | Hindgut and Cloaca (brown - hindgut and cloaca) |
- Links: Carnegie stage 13 | Stage 13 Movie
Stage 22
Animal Model
See this recent analysis of mouse cloacal morphogenesis using high-resolution episcopic microscopy.[2]
- Video 1. Figure S2. The 3-D images of the entire mouse cloaca morphogenetic process from E9.5 to E13.5.
Molecular
Sonic Hedgehog
In the mouse model of cloacal development, Shh knockout causes a severe hypoplastic defect of cloaca mesenchyme including dorsal peri-cloacal mesenchyme and persistent cloaca.[2]
- Links: SHH
Apoptosis
apoptosis - process of cell death required for the removal of the cloacal membrane.
Abnormalities
ICD-11 LB17 Structural developmental anomalies of anal canal
- LB17.2 Persistent cloaca
- LB17.3 Cloacal exstrophy
- GC04.19 Combined urinary and rectal fistula including cloaca with severe scar or extensive tissue loss
Persistent Cloaca
ICD-11 LB17.2 Persistent cloaca is a congenital anomaly in which the intestinal, urinary, and reproductive ducts open into a common cavity, a result of the failure of the urorectal septum to form during prenatal development. They occur exclusively in girls and comprise the most complex defect in the spectrum of anorectal malformations.

|
In females this abnormality results in all three structures (urinary tract, vagina, and rectum) all meeting in a common channel, similar to the early developing cloaca. Clinically the presence of a single perineal orifice is evidence of a patient with persistent cloaca.[3] |
Cloacal Exstrophy
ICD-11 LB17.3 Cloacal exstrophy a rare (about 1/200,000[4]) and complex anorectal and genitourinary malformation in which rectum, vagina and urinary tract share a common everted orifice, accompanied by an omphalocele and an imperforate anus. Exstrophy of the cloaca is a well-known malformation that includes the persistence and the exstrophy of a cloaca that receives ureters, ileum and a rudimentary hindgut. Cloacal exstrophy is a severe birth defect wherein much of the abdominal organs (the bladder and intestines) are exposed. It often causes the splitting of both male and female genitalia (specifically, the penis and clitoris respectively), and the anus is occasionally sealed.
- Links: LB17.3 Cloacal exstrophy
OEIS Complex
Omphalocele-Exstrophy-Imperforate Anus-Spinal (OEIS) defects, a combination of defects comprising omphalocele, exstrophy of the cloaca, imperforate anus, and spinal defects.
OMIM: OEIS Complex
References
- ↑ Kruepunga N, Hikspoors JPJM, Mekonen HK, Mommen GMC, Meemon K, Weerachatyanukul W, Asuvapongpatana S, Eleonore Köhler S & Lamers WH. (2018). The development of the cloaca in the human embryo. J. Anat. , 233, 724-739. PMID: 30294789 DOI.
- ↑ 2.0 2.1 2.2 Huang YC, Chen F & Li X. (2016). Clarification of mammalian cloacal morphogenesis using high-resolution episcopic microscopy. Dev. Biol. , 409, 106-113. PMID: 26485363 DOI.
- ↑ 3.0 3.1 Levitt MA & Peña A. (2007). Anorectal malformations. Orphanet J Rare Dis , 2, 33. PMID: 17651510 DOI.
- ↑ Ebert AK, Reutter H, Ludwig M & Rösch WH. (2009). The exstrophy-epispadias complex. Orphanet J Rare Dis , 4, 23. PMID: 19878548 DOI.
Books
Reviews
Vilanova-Sanchez A, McCracken K, Halleran DR, Wood RJ, Reck-Burneo CA, Levitt MA & Hewitt G. (2018). Obstetrical outcomes in adult patients born with complex anorectal malformations and cloacal anomalies: a literature review. J Pediatr Adolesc Gynecol , , . PMID: 30367985 DOI.
Peña A. (2016). Cloaca--Historical aspects and terminology. Semin. Pediatr. Surg. , 25, 62-5. PMID: 26969227 DOI.
Gupta A, Bischoff A, Peña A, Runck LA & Guasch G. (2014). The great divide: septation and malformation of the cloaca, and its implications for surgeons. Pediatr. Surg. Int. , 30, 1089-95. PMID: 25217828 DOI.
Kluth D. (2010). Embryology of anorectal malformations. Semin. Pediatr. Surg. , 19, 201-8. PMID: 20610193 DOI.
Hynes PJ & Fraher JP. (2004). The development of the male genitourinary system. I. The origin of the urorectal septum and the formation of the perineum. Br J Plast Surg , 57, 27-36. PMID: 14672675
Marshall FF. (1978). Embryology of the lower genitourinary tract. Urol. Clin. North Am. , 5, 3-15. PMID: 347662
Articles
Qian C, Wu Z, Ng RC, Garcia-Barceló MM, Yuan ZW, Wong KKY, Tam PKH & Lui VCH. (2018). Conditional deletion of platelet derived growth factor receptor alpha (Pdgfra) in urorectal mesenchyme causes mesenchyme apoptosis and urorectal developmental anomalies in mice. Cell Death Differ. , , . PMID: 30323271 DOI.
Tang XB, Li H, Zhang J, Wang WL, Yuan ZW & Bai YZ. (2018). Expression pattern of Wif1 and β-catenin during development of anorectum in fetal rats with anorectal malformations. PeerJ , 6, e4445. PMID: 29507836 DOI.
Hoshi M, Reginensi A, Joens MS, Fitzpatrick JAJ, McNeill H & Jain S. (2018). Reciprocal Spatiotemporally Controlled Apoptosis Regulates Wolffian Duct Cloaca Fusion. J. Am. Soc. Nephrol. , 29, 775-783. PMID: 29326158 DOI.
Tang XB, Zhang T, Wang WL, Yuan ZW & Bai YZ. (2016). Spatiotemporal distribution of caudal-type homeobox proteins during development of the hindgut and anorectum in human embryos. PeerJ , 4, e1771. PMID: 27042391 DOI.
Huang YC, Chen F & Li X. (2016). Clarification of mammalian cloacal morphogenesis using high-resolution episcopic microscopy. Dev. Biol. , 409, 106-113. PMID: 26485363 DOI.
Sasaki C, Yamaguchi K & Akita K. (2004). Spatiotemporal distribution of apoptosis during normal cloacal development in mice. Anat Rec A Discov Mol Cell Evol Biol , 279, 761-7. PMID: 15278947 DOI.
Nievelstein RA, van der Werff JF, Verbeek FJ, Valk J & Vermeij-Keers C. (1998). Normal and abnormal embryonic development of the anorectum in human embryos. Teratology , 57, 70-8. PMID: 9562679 <70::AID-TERA5>3.0.CO;2-A DOI.
Historic
Ludwig KS. (1965). [On the relation of the cloacal membrane and the urorectal septum in human embryos of 9-33 mm SSL]. Z Anat Entwicklungsgesch , 124, 401-13. PMID: 5832420
SCOTT JE & SWENSON O. (1959). Imperforate anus: results in 63 cases and some anatomic considerations. Ann. Surg. , 150, 477-87. PMID: 14444236
Prentiss CW. and Arey LB. A laboratory manual and text-book of embryology. (1918) W.B. Saunders Company, Philadelphia and London. Differentiation of Cloaca, Bladder, Urethra and Urogenital Sinus
Felix W. The development of the urinogenital organs. In Keibel F. and Mall FP. Manual of Human Embryology II. (1912) J. B. Lippincott Company, Philadelphia. pp 752-979.
Search Pubmed
Search Bookshelf Cloaca Development
Search Pubmed Now: Cloaca Development | Cloacal Membrane
Additional Images
Historic
| Historic Disclaimer - information about historic embryology pages |
|---|
|
Bremer JL. Description of a 4-mm human embryo. (1906) Amer. J Anat. 5: 459-480.

Fig.8. Section through body of Harvard Embryo Template:HE714 near the cloaca.
Felix W. The development of the urinogenital organs. In Keibel F. and Mall FP. Manual of Human Embryology II. (1912) J. B. Lippincott Company, Philadelphia. pp 752-979.
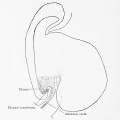
Fig. 599. Embryo Pfannenstiel-Kromer, 1.38 mm long, 5-6 somites, shows relation of cloaca and cloacal membrane to allantoic stalk.

Fig. 600. Embryo Pfannenstiel III 2.6 mm GL 13-14 somites, allantoic stalk is given off at a right angle from the cloaca, immediately above cloacal membrane. Ventral wall of the cloaca is formed only by the cloacal membrane.
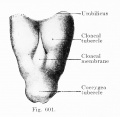
Fig. 601. Cloacal membrane human embryo 3 mm GL (Embryo E. B.) forms a rhomboidal groove slightly depressed below the surface of the embryo, between the umbilicus and the coccygeal tubercle.
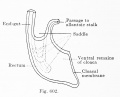
Fig. 602. Cloaca human embryo 7 mm GL (embryo Chr. I), separation of the rectum from the ventral remains of the cloaca is shown

Fig. 603 a and b. Human embryo 7 mm GL (Embryo Chr. I) division of cloaca into rectum and ventral remains of the cloaca is almost complete, the saddle between the two being immediately over the cloacal membrane.

Fig. 604 a and b. Human embryo 11 mm GL (Embryo P. I.) The rectum is completely separated from the ventral remains of the cloaca, and the cloacal membrane has been divided into the canal and urogenital membranes.

Fig. 605. Human embryo 5.3 mm GL (Embryo 1420) Primary excretory duct and opening with reference to cloaca and cloacal membrane, anlage of ureteric bud.

Fig. 606. Human embryo 4.25 mm vertex-breech length, 28 somites (Embryo H. M. 1) Primary excretory duct and position of orifice relatively to cloaca and cloacal membrane.

Fig. 607. Human embryo 18 mm Between the umbilicus and the coccygeal tubercle cranio-caudally and the two lower extremities laterally, the cloacal tubercle has appeared.








Florian J. The early development of man, with special reference to the development of the mesoderm and cloacal membrane. (1933) J. Anat., 67(2): 263-76. PMID 17104422

Fig.1
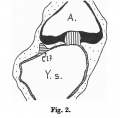
Fig.2
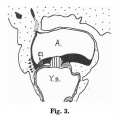
Fig.3
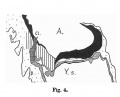
Fig.4

Fig.5
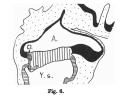
Fig.6

Fig.7

Fig.8








Terms
- cloacal duct of Reichel - Reichel P. The development of the bladder and urinary tubes (Die Entwicklung der Harnblase und der Harnrohre), (1893) Verb. phys. med. Gesellsch. Wiirzburg.
- cloacal tubercle - (genital tubercle)
| Gastrointestinal Tract Terms | ||
|---|---|---|
| ||
|
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, June 16) Embryology Cloaca Development. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Cloaca_Development
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G