Cardiovascular System - Ventricular Septal Defects
| Embryology - 26 Apr 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Introduction

The Ventricular Septal Defect (VSD) is the most common form of congenital cardiovascular anomaly, occurring in nearly 50% of all infants with a congenital heart defect. Usually occurs in the membranous (perimembranous) rather than muscular interventricular septum, and is more frequent in males that females. This defect can also contribute to outflow tract (OFT) malformations.
Perimembranous defects are located close to the aortic and tricuspid valves and adjacent to atrioventricular conduction bundle.
Some Recent Findings
|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Ventricular Septal Defect <pubmed limit=5>Ventricular Septal Defect</pubmed> |
History
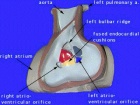
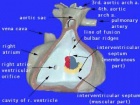
 Le Gros Clark (1847)[2] Heart autopsy drawing.
|
The first western clinical description of ventricular septal defects was made by Henri Roger in 1879[3], which later became known as maladie de Roger.
His description was based upon 6 acyanotic patients and autopsy finding of a child with ventricular septal defect. |
Ultrasound

There is a defect in the ventricular septum adjacent to the atrioventricular valves. Blood flow is seen across the defect on Colour Doppler imaging.
Pulmonary Changes
Heath-Edwards classification

(Heath-Edward grade) A pathological grading system for pulmonary artery structural changes that occur with congenital cardiac septal defects. The classification is named after the two original paper authors Donald HEATH and Jessee EDWARDS[4] and grades from I to VI with increasing severity of the arterial changes.
- Grade I - hypertrophy of the media of small muscular arteries and arterioles.
- Grade II - intimal cellular proliferation in addition to medial hypertrophy.
- Grade III - advanced medial thickening with hypertrophy and hyperplasia including progressive intimal proliferation and concentric fibrosis. Results in an obliteration of the arterioles and small arteries.
- Grade IV - "plexiform lesions" of the muscular pulmonary arteries and arterioles with a plexiform network of capillary-like channels within a dilated segment.
- Grade V - complex plexiform, angiomatous and cavernous lesions and hyalinization of intimal fibrosis.
- Grade VI - necrotizing arteritis.
International Classification of Diseases
The International Classification of Diseases (ICD) World Health Organization's classification used worldwide as the standard diagnostic tool for epidemiology, health management and clinical purposes. This includes the analysis of the general health situation of population groups. It is used to monitor the incidence and prevalence of diseases and other health problems. Within this classification "congenital malformations, deformations and chromosomal abnormalities" are (Q00-Q99) but excludes "inborn errors of metabolism" (E70-E90).
Congenital malformations of the circulatory system (Q20-Q28)
- ICD-10 Code: Q21.0 Ventricular septal defect
Q21 Congenital malformations of cardiac septa
Excl.: acquired cardiac septal defect (I51.0)
- Q21.0 Ventricular septal defect
- Q21.1 Atrial septal defect Coronary sinus defect Patent or persistent: foramen ovale ostium secundum defect (type II) Sinus venosus defect
- Q21.2 Atrioventricular septal defect Common atrioventricular canal Endocardial cushion defect Ostium primum atrial septal defect (type I)
- Q21.3 Tetralogy of Fallot Ventricular septal defect with pulmonary stenosis or atresia, dextroposition of aorta and hypertrophy of right ventricle.
- Q21.4 Aortopulmonary septal defect Aortic septal defect Aortopulmonary window
- Q21.8 Other congenital malformations of cardiac septa Eisenmenger's defect Pentalogy of Fallot Excl.: Eisenmenger's complex (I27.8) syndrome (I27.8)
- Q21.9 Congenital malformation of cardiac septum, unspecified Septal (heart) defect NOS
Movies
|
| ||||||||||
|
| ||||||||||
|
|
|

Cardiovascular Abnormalities

Heart defects and preterm birth are the most common causes of neonatal and infant death. The long-term development of the heart combined with extensive remodelling and post-natal changes in circulation lead to an abundance of abnormalities associated with this system.
A UK study literature showed that preterm infants have more than twice as many cardiovascular malformations (5.1 / 1000 term infants and 12.5 / 1000 preterm infants) as do infants born at term and that 16% of all infants with cardiovascular malformations are preterm. (0.4% of live births occur at greater than 28 weeks of gestation, 0.9% at 28 to 31 weeks, and 6% at 32 to 36 weeks. Overall, 7.3% of live-born infants are preterm)[5]
"Baltimore-Washington Infant Study data on live-born cases and controls (1981-1989) was reanalyzed for potential environmental and genetic risk-factor associations in complete atrioventricular septal defects AVSD (n = 213), with separate comparisons to the atrial (n = 75) and the ventricular (n = 32) forms of partial AVSD. ...Maternal diabetes constituted a potentially preventable risk factor for the most severe, complete form of AVSD." [6]
In addition, there are in several congenital abnormalities that exist in adults (bicuspid aortic valve, mitral valve prolapse, and partial anomalous pulmonary venous connection) which may not be clinically recognized.
References
- ↑ <pubmed>22263148</pubmed>
- ↑ <pubmed>20895864</pubmed>| PMC2104017 | PDF
- ↑ <pubmed>382810</pubmed>
- ↑ <pubmed>13573570</pubmed>Circulation
- ↑ <pubmed>16322141</pubmed>
- ↑ <pubmed>11241431</pubmed>
Reviews
<pubmed>21349577</pubmed>
Articles
<pubmed>22263148</pubmed> <pubmed>22229525</pubmed> <pubmed>22163127</pubmed> <pubmed>3808993</pubmed> <pubmed>2938464</pubmed> <pubmed>6179217</pubmed>
Search Pubmed
Search Pubmed: Ventricular Septal Defect
External Links
External Links Notice - The dynamic nature of the internet may mean that some of these listed links may no longer function. If the link no longer works search the web with the link text or name. Links to any external commercial sites are provided for information purposes only and should never be considered an endorsement. UNSW Embryology is provided as an educational resource with no clinical information or commercial affiliation.
Terms
| Cardiovascular Terms |
|---|
Cardiovascular System Development See also Heart terms, Immune terms and Blood terms.
|
| Other Terms Lists |
|---|
| Terms Lists: ART | Birth | Bone | Cardiovascular | Cell Division | Endocrine | Gastrointestinal | Genital | Genetic | Head | Hearing | Heart | Immune | Integumentary | Neonatal | Neural | Oocyte | Palate | Placenta | Radiation | Renal | Respiratory | Spermatozoa | Statistics | Tooth | Ultrasound | Vision | Historic | Drugs | Glossary |
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, April 26) Embryology Cardiovascular System - Ventricular Septal Defects. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Cardiovascular_System_-_Ventricular_Septal_Defects
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G