AACP Meeting 2013 - Face Embryology: Difference between revisions
mNo edit summary |
mNo edit summary |
||
| (19 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
=Face Embryology= | =Face Embryology= | ||
{| | |||
| | |||
'''2013 Australian Chapter, American Academy of Craniofacial Pain (AACP) Meeting''' [http://www.aacfp.com.au/ | '''2013 Australian Chapter, American Academy of Craniofacial Pain (AACP) Meeting''' [http://www.aacfp.com.au/2013events/AACP_MAY2013_EVENT_show2.pdf May 18 May 2013] | ||
[[File:Gray0784.jpg|400px]] | [[File:Gray0784.jpg|400px]] | ||
| I hope you enjoyed today's presentation. Please feel free to now come back and do some self-directed learning. | |||
If you are interested I also have one of those [https://twitter.com/MarkHill_UNSW twitter accounts], though I know am not as active as I should be. Tweets are focussed on Embryology and developmental news. | |||
--[[User:Z8600021|Mark Hill]] ([[User talk:Z8600021|talk]]) 12:24, 18 May 2013 (EST) | |||
| [[File:Twitter_icon.jpg|link=https://twitter.com/MarkHill_UNSW|thumb|120px|@MarkHill_UNSW]] | |||
| [[File:Mark Hill.jpg|thumb|Dr Mark Hill, Medicine UNSW]] | |||
[[File:Acps-logo.png|right|180px|link=http://www.acps.unsw.edu.au]] | |||
|} | |||
==Introduction== | ==Introduction== | ||
{| | {| | ||
| width=440px|< | | width=440px|<html5media height="500" width="420">File:Face_001.mp4</html5media> | ||
| | | | ||
===Development of the Face=== | |||
This animation shows a ventral view of development of the human face from approximately week 5 through to neonate. | This animation shows a ventral view of development of the human face from approximately week 5 through to neonate. | ||
| Line 134: | Line 144: | ||
{| | {| | ||
| width=330px|< | | width=330px|<html5media height="420" width="320">File:Stage16to18 face 01.mp4</html5media> | ||
| [[File:Stage16-18 face 02.jpg|right]] | | [[File:Stage16-18 face 02.jpg|right]] | ||
Movie shows a quick animation of the ventral views of the human embryo face, between [[Carnegie stage 16|Carnegie stage 16]] to [[Carnegie stage 18|stage 18]] ([[Week 6|Week 6]] to [[Week 7|Week 7]]). Animation based on Kyoto embryos. | Movie shows a quick animation of the ventral views of the human embryo face, between [[Carnegie stage 16|Carnegie stage 16]] to [[Carnegie stage 18|stage 18]] ([[Week 6|Week 6]] to [[Week 7|Week 7]]). Animation based on Kyoto embryos. | ||
| Line 143: | Line 153: | ||
:'''Links:''' [[Media:Stage16to18 face 01.mp4|MP4 | :'''Links:''' [[Media:Stage16to18 face 01.mp4|MP4 version]] | [[Lecture - Head Development]] | [[Movies]] | ||
|} | |} | ||
==Week 5 to 8== | ==Week 5 to 8== | ||
| Line 149: | Line 159: | ||
{| | {| | ||
| width=400px|< | | width=400px|<html5media height="400" width="380">File:Stage15to22 head 01.mp4</html5media> | ||
| | | | ||
[[File:Stage15to22_head_icon.jpg|right|200px]] | [[File:Stage15to22_head_icon.jpg|right|200px]] | ||
| Line 165: | Line 175: | ||
{| border='0px' | {| border='0px' | ||
|- | |- | ||
| width=360px|< | | width=360px|<html5media height="350" width="350">File:Palate_001.mp4</html5media> | ||
| valign="top" |[[File:Palate_001_icon.jpg|200px|right]] | | valign="top" |[[File:Palate_001_icon.jpg|200px|right]] | ||
| Line 175: | Line 185: | ||
* Secondary palate formation is the growth of the palatal shelves towards the midline. | * Secondary palate formation is the growth of the palatal shelves towards the midline. | ||
|- | |- | ||
| width=360px|< | | width=360px|<html5media height="350" width="350">File:Palate_002.mp4</html5media> | ||
| valign="top" |[[File:Palate_002_icon.jpg|200px|right]] | | valign="top" |[[File:Palate_002_icon.jpg|200px|right]] | ||
Animation shows an anterior view of the developmental sequence of secondary palate formation. The frontal region of the head has been removed to show the changes within the oral cavity. | Animation shows an anterior view of the developmental sequence of secondary palate formation. The frontal region of the head has been removed to show the changes within the oral cavity. | ||
| Line 317: | Line 327: | ||
|} | |} | ||
===External Ear=== | ===External Ear=== | ||
{| | |||
| | |||
Images of the lateral view of the human embryonic head from [[week 5]] ([[Carnegie_stage_14|stage 14]]) through to [[week 8]] ([[Carnegie_stage_23|stage 23]]) showing development of the [[A#auricular hillocks|auricular hillocks]] that will form the external ear. | Images of the lateral view of the human embryonic head from [[week 5]] ([[Carnegie_stage_14|stage 14]]) through to [[week 8]] ([[Carnegie_stage_23|stage 23]]) showing development of the [[A#auricular hillocks|auricular hillocks]] that will form the external ear. | ||
| Line 323: | Line 334: | ||
Images are not to scale. | Images are not to scale. | ||
| {{External ear movie}} | |||
|} | |||
[[File:External_ear_stages-14-23-adult.jpg|600px]] | [[File:External_ear_stages-14-23-adult.jpg|600px]] | ||
| Line 338: | Line 350: | ||
The bones enclosing the brain have large flexible fibrous joints (sutures) which allow firstly the head to compress and pass through the birth canal and secondly to postnatally expand for brain growth. (More? [[#Molecular_Skull_Sutures|Molecular Skull Sutures]]) These sutures gradually fuse at different times postnatally, firstly the metopic suture in infancy and the others much later. Abnormal fusion (synostosis) of any of the sutures will lead to a number of different skull defects, leading to disruption of brain development. (More? [[#Abnormal_Synostosis|Abnormal Synostosis]]) In old age all these sutures are generally completely fused and ossified. | The bones enclosing the brain have large flexible fibrous joints (sutures) which allow firstly the head to compress and pass through the birth canal and secondly to postnatally expand for brain growth. (More? [[#Molecular_Skull_Sutures|Molecular Skull Sutures]]) These sutures gradually fuse at different times postnatally, firstly the metopic suture in infancy and the others much later. Abnormal fusion (synostosis) of any of the sutures will lead to a number of different skull defects, leading to disruption of brain development. (More? [[#Abnormal_Synostosis|Abnormal Synostosis]]) In old age all these sutures are generally completely fused and ossified. | ||
At the molecular level, accelerated suture intramembranous ossification can be mediated through a dual role of β-catenin in both the expansion of osteoprogenitors and the maturation of osteoblasts. | At the molecular level, accelerated suture intramembranous ossification can be mediated through a dual role of β-catenin in both the expansion of osteoprogenitors and the maturation of osteoblasts.{{#pmid:17113065|PMID17113065}} These researchers also show that disruption of Axin2/β-catenin signaling alters the regulation of the downstream transcription target, cyclin D1, in the canonical Wnt pathway.{{#pmid:21108844|PMID21108844}} | ||
===Cranial Base Synchondroses=== | ===Cranial Base Synchondroses=== | ||
In the base of the skull there can also be found a number of synchondrosis, "cartilage sutures", that are the last to close and have a role in the ongoing growth of the postnatal skull. | In the base of the skull there can also be found a number of synchondrosis, "cartilage sutures", that are the last to close and have a role in the ongoing growth of the postnatal skull. | ||
| Line 388: | Line 400: | ||
|} | |} | ||
{| class="wikitable collapsible collapsed" | {| class="wikitable collapsible collapsed" | ||
! Statistics | ! Statistics | ||
| Line 495: | Line 506: | ||
Turricephaly | Turricephaly | ||
| [[ | | [[File:Skull CT abnormal 05.jpg|300px]] | ||
Posterior Plagiocephaly | Posterior Plagiocephaly | ||
| Line 538: | Line 549: | ||
* retroglossia | * retroglossia | ||
* U-shaped posterior cleft palate | * U-shaped posterior cleft palate | ||
[[File:Newborn micrognathia 01.jpg|thumb|Newborn micrognathia | [[File:Newborn micrognathia 01.jpg|thumb|Newborn micrognathia{{#pmid:20716376|PMID20716376}}]] | ||
[[File:Pierre Robin sequence 01.jpg|200px]] | [[File:Pierre Robin sequence 01.jpg|200px]] | ||
Frontal and lateral views of an infant with Pierre Robin sequence. | Frontal and lateral views of an infant with Pierre Robin sequence.{{#pmid:22300418|PMID22300418}} | ||
====DiGeorge Syndrome==== | ====DiGeorge Syndrome==== | ||
| Line 558: | Line 569: | ||
====Choanal Atresia==== | ====Choanal Atresia==== | ||
[[File:Choanal atresia computed tomography 01.jpg|thumb|Choanal atresia computed tomography | [[File:Choanal atresia computed tomography 01.jpg|thumb|Choanal atresia computed tomography{{#pmid:21772853|PMID21772853}}]] | ||
* Choanal atresia is the most common form of congenital nasal obstruction, usually diagnosed at birth. | * Choanal atresia is the most common form of congenital nasal obstruction, usually diagnosed at birth.{{#pmid:21772853|PMID21772853}} | ||
* failure of the posterior nasal cavity (choanae) to communicate with the nasopharynx. | * failure of the posterior nasal cavity (choanae) to communicate with the nasopharynx. | ||
* Thought to be secondary to an abnormality during the rupture of the buccopharyngeal membrane in the embryological period. | * Thought to be secondary to an abnormality during the rupture of the buccopharyngeal membrane in the embryological period. | ||
| Line 596: | Line 607: | ||
| valign="bottom"|{{Mandible movie}} | | valign="bottom"|{{Mandible movie}} | ||
|- | |- | ||
| valign="bottom"|{{Fetal week 10 palate movie}} | |||
| valign="bottom"|{{External ear movie}} | |||
| valign="bottom"|{{Cleft Lip 01}} | | valign="bottom"|{{Cleft Lip 01}} | ||
| valign="bottom"|{{Cleft Lip 02}} | | valign="bottom"|{{Cleft Lip 02}} | ||
| Line 610: | Line 623: | ||
==Historic== | ==Historic== | ||
As I mentioned in my presentation, I have included here links to some beautiful illustrations and plates from historic embryology sources. | |||
===1910 Manual of Human Embryology=== | ===1910 Manual of Human Embryology=== | ||
{{Ref-KeibelMall1910}} - [[Book_-_Manual_of_Human_Embryology_11E#E._The_Skull.2C_Hyoid_Bone.2C_and_Larynx|The The Skull, Hyoid Bone, and Larynx]] | |||
| Line 636: | Line 650: | ||
===1920 Contributions to Embryology Carnegie Institution No.39=== | ===1920 Contributions to Embryology Carnegie Institution No.39=== | ||
{{Ref-Lewis1920}} | |||
<gallery> | <gallery> | ||
| Line 648: | Line 661: | ||
===1921 Contributions to Embryology Carnegie Institution No.48=== | ===1921 Contributions to Embryology Carnegie Institution No.48=== | ||
{{Ref-Macklin1921}} | |||
<gallery> | <gallery> | ||
| Line 656: | Line 669: | ||
File:Macklin-plate04.jpg|Plate 4 | File:Macklin-plate04.jpg|Plate 4 | ||
</gallery> | </gallery> | ||
Latest revision as of 09:18, 25 June 2018
Face Embryology
|
2013 Australian Chapter, American Academy of Craniofacial Pain (AACP) Meeting May 18 May 2013
|
I hope you enjoyed today's presentation. Please feel free to now come back and do some self-directed learning.
|
|


Introduction
| <html5media height="500" width="420">File:Face_001.mp4</html5media> |
Development of the FaceThis animation shows a ventral view of development of the human face from approximately week 5 through to neonate. The separate embryonic components that contribute to the face have been colour coded.
The stomodeum is the primordial mouth region and a surface central depression lying between the forebrain bulge and the heart bulge. At the floor of the stomodeum indentation is the buccopharyngeal membrane (oral membrane). Note the complex origin of the maxillary region (upper jaw) requiring the fusion of several embryonic elements, abnormalities of this process lead to cleft lip and cleft palate.
|
Key Concepts
Buccopharyngeal Membrane
These images of the Stage 11 embryo show the breakdown of the buccopharyngeal membrane.

Low power ventral view of the Buccopharyngeal Membrane

Higher power ventrolateral view of the Buccopharyngeal Membrane

Close up view of the degenerating Buccopharyngeal Membrane



The Pharynx



The cavity within the pharyngeal arches forms the pharynx.
- begins at the buccopharyngeal membrane (oral membrane), apposition of ectoderm with endoderm (no mesoderm between)
- expands behind pharyngeal arches
- narrows at glottis and bifurcation of gastrointestinal (oesophagus) and respiratory (trachea) systems
- regions on roof, walls and floor have important contributions to endocrine in oral and neck regions
- also contributes to tongue development
Pharyngeal Arches


Major features to identify for each: arch, pouch, groove and membrane. Contribute to the formation of head and neck and in the human appear at the 4th week. The first arch contributes the majority of upper and lower jaw structures.
- branchial arch (Greek. branchia = gill)
- arch consists of all 3 trilaminar embryo layers
- ectoderm- outside and neural crest
- mesoderm - core of mesenchyme
- endoderm - inside
Neural Crest
- Mesenchyme invaded by neural crest generating connective tissue components
- cartilage, bone, ligaments
- arises from midbrain and hindbrain region
|
|


Arch Cartilages



Meckel's cartilage - located within the first pharyngeal arch mandibular prominence, forms a cartilage "template" besides which the mandible develops by the process of intramembranous ossification. It is important to note that this cartilage template does not ossify (endochondral ossification) but provides a transient structure where the mandible will form, and later degenerates.
Week 3
Gestational Age (GA week 5)
These images of the Stage 11 embryo show the breakdown of the buccopharyngeal membrane.
Low power ventral view of the Buccopharyngeal Membrane
Higher power ventrolateral view of the Buccopharyngeal Membrane
Close up view of the degenerating Buccopharyngeal Membrane
Week 4 to 5
Gestational Age (GA week 6 to 7)
Begins week 4 centered around stomodeum, external depression at oral membrane
5 initial primordia from neural crest mesenchyme (week 4)
- single frontonasal prominence (FNP) - forms forehead, nose dorsum and apex
- nasal placodes develop later bilateral, pushed medially
- paired maxillary prominences - form upper cheek and upper lip
- paired mandibular prominences - lower cheek, chin and lower lip
Stage 11 (25 days)

Stage 12 (26 days)

Stage 13 (28 days)

Stage 14 (32 days)





Cranial Ganglia



Week 6 to 7
Gestational Age (GA week 8 to 9)
| <html5media height="420" width="320">File:Stage16to18 face 01.mp4</html5media> |  Movie shows a quick animation of the ventral views of the human embryo face, between Carnegie stage 16 to stage 18 (Week 6 to Week 7). Animation based on Kyoto embryos.
|
Week 5 to 8
Gestational Age (GA week 7 to 10)
| <html5media height="400" width="380">File:Stage15to22 head 01.mp4</html5media> |
Movie shows a quick animation of the lateral view of the human embryo head, between Carnegie stage 15 to stage 22 (Week 5 to Week 8). Note that these stage images are not to scale.
|
Week 9
Gestational Age (GA week 11)
Secondary Palate Development
| <html5media height="350" width="350">File:Palate_001.mp4</html5media> | Animation shows an inferior view of the developmental sequence of secondary palate formation. The lower jaw has been removed and the view shows the roof of the oral cavity and the maxilla (upper jaw) and lip.
|
| <html5media height="350" width="350">File:Palate_002.mp4</html5media> | Animation shows an anterior view of the developmental sequence of secondary palate formation. The frontal region of the head has been removed to show the changes within the oral cavity. Secondary palate formation is the growth of the palatal shelves towards the midline, from top to bottom:
|
Week 10
Gestational Age (GA week 12)

hard palate |

soft palate |
- Fetal Palate Links: Hard and soft palate | Detail - hard and soft palate junction | Detail - hard palate seam | hard palate | hard palate labeled | soft palate | soft palate labeled | Fetal palate movie | MP4 version | GIF version | Palate Development
Image Source: Prof Virginia Diewert
Week 12
Gestational Age (GA week 14)

| Bone and Cartilage | |
|---|---|

|

|
| Medial view | Lateral view |
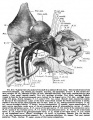
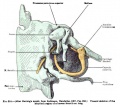
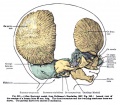
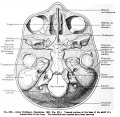
| Historic - cartilaginous and membranous skull | |
|---|---|

|

|
| Dorsal aspect of base of the adult skull. Bone ossified in cartilage stained blue. Modified from Spalteholz Atlas. | Lateral view of part of cartilaginous and membranous skull. The inner wall of the orbit and part of occipito-temporal region exposed by cutting away part of the membranous skull. |

|

|
| Chondrocranium and membrane bones. | Cartilage is colored blue, except figure 4, precartilage green, nerves yellow, muscles red; the blastema remains uncolored. |

Sagittal unlabeled

Sagittal labeled

Pituitary unlabeled

Pituitary labeled

Tongue




- 12 Week Images: Sagittal unlabeled | Sagittal labeled | Sagittal medial view | Sagittal lateral view | Pituitary unlabeled | Pituitary labeled | Tongue | Skull Development | Head Development
Week 14
Gestational Age (GA week 16)

|
|
Growth of Head Structures
Maxilla
- First pharyngeal arch - upper maxillary (pair) and lower mandibular prominences
- Late embryonic period - maxillary prominences fuse with frontonasal prominence forming upper jaw (maxilla and upper lip)



- EM Links: Image - stage 16 | Image - stage 17 | Image - stage 18 | Image - stage 19 | Palate Development
Temporal Bone and Mandible
| Image shows growth of both bones from the end of the embryonic period (week 8) through the fetal period of development (to 9 months).
|
|

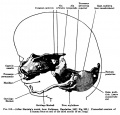
Inner Ear

| Week 5 | Week 8 | ||||
|---|---|---|---|---|---|

|

| ||||
Stage 13 embryo (week 5) showing otocyst that will form the inner ear.
|
Stage 22 embryo (week 8) showing the embryo near the end of the embryonic period.
|
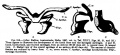
External Ear
|
Images of the lateral view of the human embryonic head from week 5 (stage 14) through to week 8 (stage 23) showing development of the auricular hillocks that will form the external ear. The adult ear is also shown indicating the part of the ear that each hillock contributes. Images are not to scale. |
|

Fetal Head Growth

Neonatal Skull
These computed tomography (CT) scans of the normal neonatal skull are shown as as 3D surface-rendered reconstructions.

Skull Sutures

The bones enclosing the brain have large flexible fibrous joints (sutures) which allow firstly the head to compress and pass through the birth canal and secondly to postnatally expand for brain growth. (More? Molecular Skull Sutures) These sutures gradually fuse at different times postnatally, firstly the metopic suture in infancy and the others much later. Abnormal fusion (synostosis) of any of the sutures will lead to a number of different skull defects, leading to disruption of brain development. (More? Abnormal Synostosis) In old age all these sutures are generally completely fused and ossified.
At the molecular level, accelerated suture intramembranous ossification can be mediated through a dual role of β-catenin in both the expansion of osteoprogenitors and the maturation of osteoblasts.[1] These researchers also show that disruption of Axin2/β-catenin signaling alters the regulation of the downstream transcription target, cyclin D1, in the canonical Wnt pathway.[2]
Cranial Base Synchondroses
In the base of the skull there can also be found a number of synchondrosis, "cartilage sutures", that are the last to close and have a role in the ongoing growth of the postnatal skull.
Synchondrosis is a type of cartilaginous joint in which the cartilage is usually converted into bone before adult life. It has been compared in appearance to a long bone growth plate, but is bipolar rather than unipolar in structure.
These sutures also lost at different times in postnatal development:
- Inter-sphenoidal – around birth
- Spheno-ethmoidal – 6-7 yrs
- Spheno-occipital – 12-15 yrs
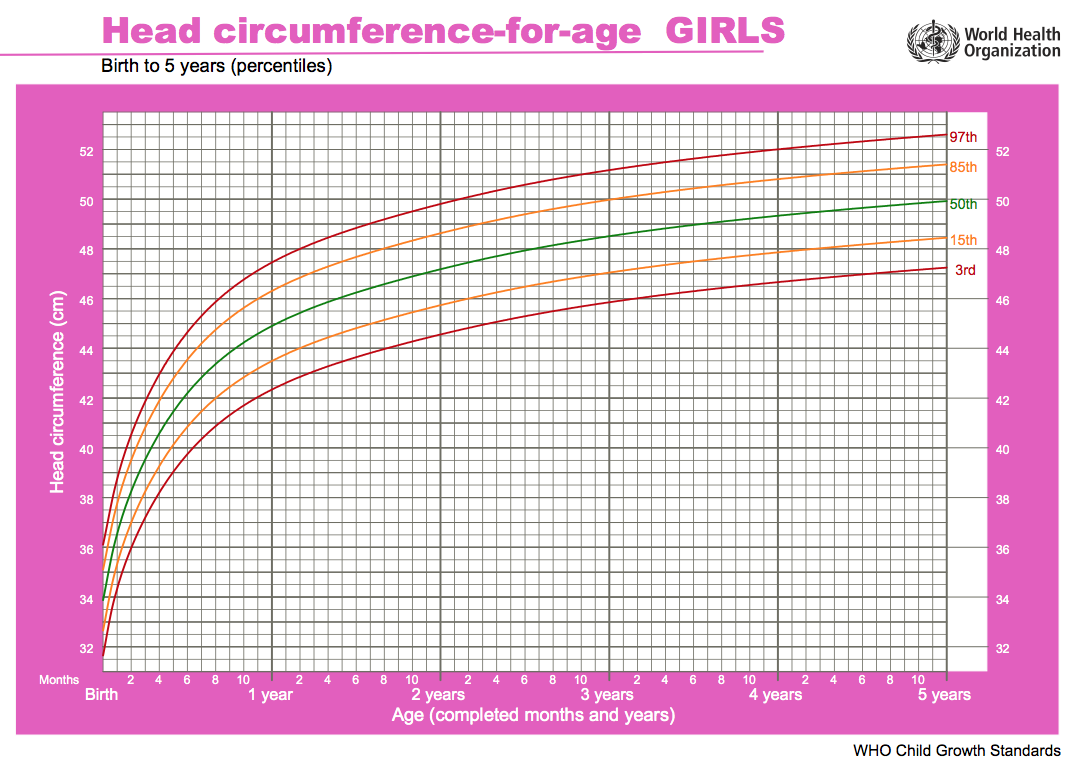
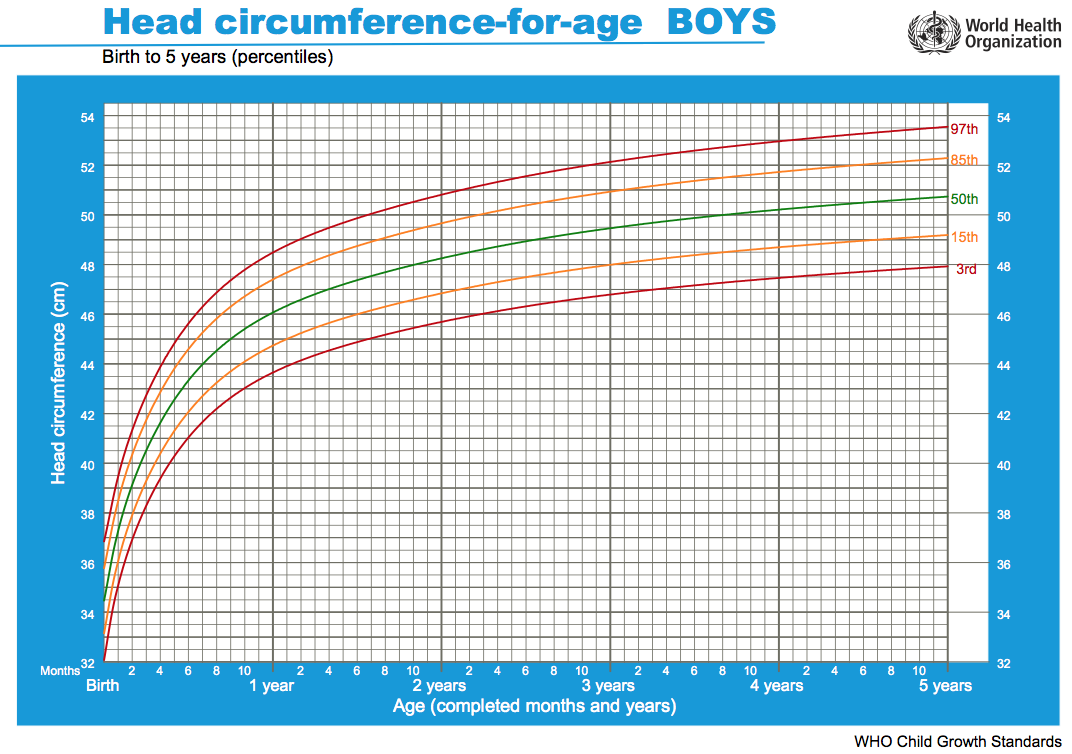
Head Growth
Slightly different charts for girls and boys. Given as head circumference-for-age Birth to: 13 weeks, 2 years, 5 years.
| Girls | Boys |
|---|---|

|

|
| Chart PDF | WHO - Girls | Chart PDF | WHO - Boys |
Abnormalities
Pharyngeal Abnormalities

There are typically four different terms for the different types of pharyngeal abnormalities, all of these except clefting are relatively rare.
- Sinuses - a pharyngeal groove defect, when a portion of the groove persists and opens to the skin surface, located laterally on the neck.
- Fistula - a pharyngeal membrane defect, a tract extends from pharynx (tonsillar fossa) beween the carotid arteries (internal and external) to open on side of neck.
- Cysts -a cervical sinus defect, remants of the cervical sinus remains as a fluid-filled cyst lined by an epithelium.
- Vestiges - a cartilaginous or bony developmental remnants that lie under the skin on side of neck.
- Clefting - the way in which the upper jaw forms from fusion of the smaller upper prominence of the first pharyngeal arch leads to a common congenital defect in this region called "clefting", which may involve either the upper lip, the palate or both structures.
Cleft Lip and Palate
- 300+ different abnormalities, different cleft forms and extent, upper lip and ant. maxilla, hard and soft palate

|

|

|
| cleft palate | unilateral cleft lip and palate | bilateral cleft lip and palate |
| Statistics | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
[[File:Australian_abnormalities_81-92_git.jpg|thumb|Cleft Lip and Palate - Australia (1981-1992)[3]
VictoriaThe ten most frequently reported birth defects in Victoria between 2003-2004.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
International Classification of Diseases - Cleft PalateCleft lip and cleft palate (Q35-Q37) Use additional code (Q30.2), if desired, to identify associated malformations of the nose. Excludes Robin's syndrome ( Q87.0 )
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ultrasound Cleft Lip and Palate | |||||||
|---|---|---|---|---|---|---|---|
|
|


Cleft Palate
- Cleft palate has the International Classification of Diseases code 749.0.
- In Australia the national rate (1982-1992) for this abnormalitity in births was 4.8 - 6/10,000 births, which represented 1,530 infants 5.5% were stillborn and 11.5% liveborn died during neonatal period and slightly more common in twin births than singleton.
Cleft Lip
- The International Classification of Diseases code 749.1 for isolated cleft lip and 749.2 for cleft lip with cleft palate.
- In Australia the national rate (1982-1992) for this abnormalitity was 8.1 - 9.9 /10,000 births. Of 2,465 infants 6.2% were stillborn and 7.8% liveborn died during neonatal period and the rate was similar in singleton and twin births.
- Links: Palate Development
Skull
Cephalic (Greek, kephale = head) are a group of abnormalities that relate to a wide range of skeletal (skull) and neural (brain) associated defects.
| Abnormal Neonatal Skull (CT) | ||
|---|---|---|

Dolichocephaly and Scaphocephaly |

Coronal Synostosis |

Anterior Plagiocephaly |

Turricephaly |

Posterior Plagiocephaly |

Deformational Plagiocepahly |

Trigonocephaly |

Oxycephaly |
- Skull CT Images: Normal overview | Normal vertex and lateral | Normal endocranial and vertex | Normal Vertex - Fontanels | Dolichocephaly and Scaphocephaly | Coronal Synostosis | Anterior Plagiocephaly | Turricephaly | Posterior Plagiocephaly | Deformational Plagiocepahly | Trigonocephaly | Oxycephaly | Computed Tomography
Genetic Syndromes
First Arch Syndrome - There are 2 major types of associated first arch syndromes, Treacher Collins (Mandibulofacial dysostosis) and Pierre Robin (Pierre Robin complex or sequence), both result in extensive facial abnormalites.
Treacher Collins Syndrome

- a rare autosomal dominant craniofacial disorder (1:50,000)
- TCOF1 gene encoding Treacle protein
- caused by frameshift deletions or duplications
- located chromosome 5
- encodes a serine/alanine-rich nucleolar phospho-protein
Features
- hypoplasia of the mandible and zygomatic complex
- down-slanting palpebral fissures
- coloboma of the lower eyelid
- absence of eyelashes medial to the defect
- external and middle ear malformation
- conductive hearing loss
Pierre Robin Syndrome
Also called Pierre Robin sequence.
- Hypoplasia of the mandible, cleft palate, eye and ear defects.
- micrognathia - Initial defect is small mandible resulting in posterior displacement of tongue and a bilateral cleft palate.
- retroglossia
- U-shaped posterior cleft palate


Frontal and lateral views of an infant with Pierre Robin sequence.[5]
DiGeorge Syndrome
- absence of thymus and parathyroid glands, 3rd and 4th pouch do not form
- disturbance of cervical neural crest migration
Mandibular Hypoplasia

One of the most common malformations of the facial skeleton usually associated with a deficient gonial angle, ascending ramus, and mandibular corpus.
- gonial angle - (angle of the jaw, angle of the mandible) the angle formed by the junction of the posterior and lower borders of the human lower jaw.
- ascending ramus - the more or less vertical part of the jaw which carries the joint with the skull.
- mandibular corpus - the horizontal or tooth-bearing portion of the mandible.
Choanal Atresia

- Choanal atresia is the most common form of congenital nasal obstruction, usually diagnosed at birth.[6]
- failure of the posterior nasal cavity (choanae) to communicate with the nasopharynx.
- Thought to be secondary to an abnormality during the rupture of the buccopharyngeal membrane in the embryological period.
- Links: Smell Development
Fetal Alcohol Syndrome

(FAS) Due to alcohol in early development (week 3+) leading to both facial and neurological abnormalities. This disorder was clinically described (USA) in humans about 30 years ago (1973), while historically alcohol's teratogenic effects were identified in the early 20th century in a mix with the prohibition cause of the period. Similar effects without the obvious alterations to appearance, but with nervous system effects, are sometimes identified as Fetal Alcohol Effects (FAE). Alcohol is able to cross the placenta from maternal circulation through the placenta into fetal circulation.
FAS Features:
- lowered ears, small face, mild+ retardation
- Microcephaly - leads to small head circumference
- Short Palpebral fissure - opening of eye
- Epicanthal folds - fold of skin at inside of corner of eye
- Flat midface
- Low nasal bridge
- Indistinct Philtrum - vertical grooves between nose and mouth
- Thin upper lip
- Micrognathia - small jaw
Exposure of embryos in vitro to ethanol simulates premature differentiation of prechondrogenic mesenchyme of the facial primordia (1999)
Movies
|
|
|
|
| |||||||||||||||
|
|
|
|
| Adult Skull MRI | Links: | Skull Development | - MRI | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
References
- ↑ Liu B, Yu HM & Hsu W. (2007). Craniosynostosis caused by Axin2 deficiency is mediated through distinct functions of beta-catenin in proliferation and differentiation. Dev. Biol. , 301, 298-308. PMID: 17113065 DOI.
- ↑ Mirando AJ, Maruyama T, Fu J, Yu HM & Hsu W. (2010). β-catenin/cyclin D1 mediated development of suture mesenchyme in calvarial morphogenesis. BMC Dev. Biol. , 10, 116. PMID: 21108844 DOI.
- ↑ Lancaster P & Pedisich E 1995. Congenital malformations Australia 1981-1992. Birth defects series no. 1. Cat. no. AIHW 213. Canberra: AIHW | NPESU | ISSN 13218352.
- ↑ Morokuma S, Anami A, Tsukimori K, Fukushima K & Wake N. (2010). Abnormal fetal movements, micrognathia and pulmonary hypoplasia: a case report. Abnormal fetal movements. BMC Pregnancy Childbirth , 10, 46. PMID: 20716376 DOI.
- ↑ Sesenna E, Magri AS, Magnani C, Brevi BC & Anghinoni ML. (2012). Mandibular distraction in neonates: indications, technique, results. Ital J Pediatr , 38, 7. PMID: 22300418 DOI.
- ↑ 6.0 6.1 Al-Noury K & Lotfy A. (2011). Role of multislice computed tomography and local contrast in the diagnosis and characterization of choanal atresia. Int J Pediatr , 2011, 280763. PMID: 21772853 DOI.
Related Pages
Historic
As I mentioned in my presentation, I have included here links to some beautiful illustrations and plates from historic embryology sources.
1910 Manual of Human Embryology
Keibel F. and Mall FP. Manual of Human Embryology I. (1910) J. B. Lippincott Company, Philadelphia. - The The Skull, Hyoid Bone, and Larynx

308

309

310
311
312

313
314

315
316

317

318

319

320
321
322

323

324















1920 Contributions to Embryology Carnegie Institution No.39
Lewis WH. The cartilaginous skull of a human embryo twenty-one millimeters in length. (1920) Contrib. Embryol., Carnegie Inst. Wash. Publ. 272, 9: 299-324.

Plate 1

Plate 2

Plate 3

Plate 4

Plate 5




1921 Contributions to Embryology Carnegie Institution No.48
Macklin CC. the skull of a human fetus of 43 millimeters greatest length. (1921) Contrib. Embryol., Carnegie Inst. Wash. Publ., 48, 10:59-102.

Plate 1

Plate 2

Plate 3

Plate 4



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, June 16) Embryology AACP Meeting 2013 - Face Embryology. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/AACP_Meeting_2013_-_Face_Embryology
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G