Placenta - Membranes: Difference between revisions
mNo edit summary |
mNo edit summary |
||
| (12 intermediate revisions by the same user not shown) | |||
| Line 3: | Line 3: | ||
[[File:Placental_membranes.jpg|thumb|400px|Human Placental Membranes]] | [[File:Placental_membranes.jpg|thumb|400px|Human Placental Membranes]] | ||
[[File:Stage17 embryo and membranes05.jpg|thumb|alt=Stage17 embryo and membranes|Stage17 embryo and membranes]] | [[File:Stage17 embryo and membranes05.jpg|thumb|alt=Stage17 embryo and membranes|Stage17 embryo and membranes]] | ||
The placental membranes is a term often used to describe the all the fetal components of the placenta (Greek, ''plakuos'' = flat cake). | The {{placental membranes}} is a term often used to describe the all the fetal components of the placenta (Greek, ''plakuos'' = flat cake). | ||
This page will not cover the whole placenta, just the development of the extra-embryonic membranes that form the extra-embryonic coeloms (cavities or spaces); amnionic sac, chorionic sac, yolk sac and allantois. | This page will not cover the whole placenta, just the development of the extra-embryonic membranes that form the extra-embryonic coeloms (cavities or spaces); amnionic sac, chorionic sac, yolk sac and allantois. | ||
| Line 20: | Line 20: | ||
|} | |} | ||
<br> | |||
{{Placenta Links}} | <br> | ||
{{Placenta Links}} | |||
<br> | |||
[[Coelomic Cavity Development]] | |||
==Some Recent Findings== | ==Some Recent Findings== | ||
{| | {| | ||
|-bgcolor="F5FAFF" | |-bgcolor="F5FAFF" | ||
| | | | ||
* '''The embryo reunited with its membranes in Göttingen''' | * '''Function and failure of the fetal membrane: Modelling the mechanics of the chorion and amnion'''{{#pmid:28350838|PMID28350838}} "The fetal membrane surrounds the fetus during pregnancy and is a thin tissue composed of two layers, the chorion and the amnion. While rupture of this membrane normally occurs at term, preterm rupture can result in increased risk of fetal mortality and morbidity, as well as danger of infection in the mother. Although structural changes have been observed in the membrane in such cases, the mechanical behaviour of the human fetal membrane in vivo remains poorly understood and is challenging to investigate experimentally. Therefore, the objective of this study was to develop simplified finite element models to investigate the mechanical behaviour and rupture of the fetal membrane, particularly its constituent layers, under various physiological conditions. It was found that modelling the chorion and amnion as a single layer predicts remarkably different behaviour compared with a more anatomically-accurate bilayer, significantly underestimating stress in the amnion and under-predicting the risk of membrane rupture. Additionally, reductions in chorion-amnion interface lubrication and chorion thickness (reported in cases of preterm rupture) both resulted in increased membrane stress. Interestingly, the inclusion of a weak zone in the fetal membrane that has been observed to develop overlying the cervix would likely cause it to fail at term, during labour. Finally, these findings support the theory that the amnion is the dominant structural component of the fetal membrane and is required to maintain its integrity. The results provide a novel insight into the mechanical effect of structural changes in the chorion and amnion, in cases of both normal and preterm rupture." | ||
* '''The embryo reunited with its membranes in Göttingen'''{{#pmid:26286940|PMID26286940}} "An EMBO workshop entitled 'Embryonic-Extraembryonic Interfaces' took place in Göttingen, Germany, in May 2015. It showcased the enormous breadth of this area not only by touching on the molecular and cellular mechanisms of development, but also because of its coverage of particularly interesting evolutionary questions and of several medically related aspects. This Meeting Review discusses some highlights from the workshop and the emerging themes in the field." | |||
|} | |} | ||
{| class="wikitable mw-collapsible mw-collapsed" | {| class="wikitable mw-collapsible mw-collapsed" | ||
! More recent papers | ! More recent papers | ||
|- | |- | ||
| [[File:Mark_Hill.jpg|90px|left]] {{Most_Recent_Refs}} | | [[File:Mark_Hill.jpg|90px|left]] {{Most_Recent_Refs}} | ||
Search term: [http://www.ncbi.nlm.nih.gov/pubmed/?term=Placental+Membrane+Development ''Placental Membrane Development''] | Search term: [http://www.ncbi.nlm.nih.gov/pubmed/?term=Placental+Membrane+Development ''Placental Membrane Development''] | [http://www.ncbi.nlm.nih.gov/pubmed/?term=Amniotic+Membrane+Development ''Amniotic Membrane Development''] | [http://www.ncbi.nlm.nih.gov/pubmed/?term=Chorionic+Membrane+Development ''Chorionic Membrane Development''] | [http://www.ncbi.nlm.nih.gov/pubmed/?term=Amniotic+Fluid ''Amniotic Fluid''] | ||
|} | |||
{| class="wikitable mw-collapsible mw-collapsed" | |||
! Older papers | |||
|- | |||
| {{Older papers}} | |||
* '''Complete chorion-amnion separation presenting as a stuck fetus'''{{#pmid:23647025|PMID23647025}} "During feto-placental development, chorion-amnion fusion occurs in early second trimester and persistent separation of the membranes beyond 17 weeks' gestation is considered abnormal. Several reports have shown that complete chorion-amnion separation, defined as the amnion being separated from the chorion on at least three sides of the gestational sac, is associated with prenatal invasive procedures including amniocentesis. We would like to call attention to a case of complete chorion-amnion separation that occurred without any invasive procedures." | |||
|} | |} | ||
==Reading== | ==Reading== | ||
| Line 67: | Line 75: | ||
|- | |- | ||
| width= | | width=510px|<html5media height="580" width="500">File:Chorion 001.mp4</html5media> | ||
| [[File:Chorion 001 icon.jpg|200px|right]] Animation shows the events following implantation and focuses on changes in the the spaces surrounding the embryonic disc, the extraembryonic coelom. Week 2 the blastoceol cavity is initially converted into a primary yolk sac by hypoblast layer. Week 2 to 3 then with gastrulation by endoderm and extra-embryonic mesoderm into two separate spaces: the yolk sac and the chorionic cavity. The third space lies above the epiblast, the amniotic cavity. | | [[File:Chorion 001 icon.jpg|200px|right]] Animation shows the events following implantation and focuses on changes in the the spaces surrounding the embryonic disc, the extraembryonic coelom. Week 2 the blastoceol cavity is initially converted into a primary yolk sac by hypoblast layer. Week 2 to 3 then with gastrulation by endoderm and extra-embryonic mesoderm into two separate spaces: the yolk sac and the chorionic cavity. The third space lies above the epiblast, the amniotic cavity. | ||
| Line 89: | Line 97: | ||
The amniotic sac (cavity) is initially lined by ectoderm and covered by extra-embryonic mesoderm. In the human embryo during week 3 to 4, folding of the embryonic disc draws the amniotic membrane ventrally over the embryo leading to the enclosing of the embryo within the amniotic sac. Embryonic and fetal development from this time onward occurs fully enclosed within the amniotic sac floating in the amniotic fluid. | The amniotic sac (cavity) is initially lined by ectoderm and covered by extra-embryonic mesoderm. In the human embryo during week 3 to 4, folding of the embryonic disc draws the amniotic membrane ventrally over the embryo leading to the enclosing of the embryo within the amniotic sac. Embryonic and fetal development from this time onward occurs fully enclosed within the amniotic sac floating in the amniotic fluid. | ||
The membrane consists of three layers - epithelial monolayer, acellular connective tissue and fibroblast layer, see review{{#pmid:26510939|PMID26510939}} | |||
===Epithelial Monolayer=== | |||
Cuboidal cell epithelium with a basement membrane. These cells are in direct contact with the amniotic fluid. | |||
Secrete | |||
* glycoproteins and collagen fibres to form the basal membrane. | |||
* variety of growth factors and cytokines - epidermal growth factor, vascular endothelial growth factor, keratinocyte growth factor, basic fibroblast growth factor, transforming growth factors alpha and beta (TGF-α and TGF-β), interleukin-8 (IL-8), angiogenin, dipeptidyl peptidase IV (DPPIV/CD26), serine protease inhibitor (serpin) E1, also known as type 1 plasminogen activator inhibitor (PAI-1), insulin-like growth factors. | |||
===Connective Tissue=== | |||
An underlying compact layer without cells of connective tissue bundles of collagen for membrane mechanical strength. | |||
===Fibroblast Layer=== | |||
Under the acellular CT layer lies a thick layer of fibroblast cells forming a stroma. | |||
[[File:Yolk sac and amniotic cavity volume graph.jpg|400px]] | [[File:Yolk sac and amniotic cavity volume graph.jpg|400px]] | ||
Yolk sac and amniotic cavity volume week 2 to 3 (stage [[Carnegie stage 5|5]], [[Carnegie stage 6|6]], [[Carnegie stage 7|7]] and [[Carnegie stage 8|8]]). | Yolk sac and amniotic cavity volume week 2 to 3 (stage [[Carnegie stage 5|5]], [[Carnegie stage 6|6]], [[Carnegie stage 7|7]] and [[Carnegie stage 8|8]]). | ||
| Line 101: | Line 131: | ||
# contributes to respiratory and gastrointestinal development. | # contributes to respiratory and gastrointestinal development. | ||
# helps prevent infection. | # helps prevent infection. | ||
# can provide a short-term source of nutrients and fluid to the embryo. | # can provide a short-term source of nutrients and fluid to the embryo.{{#pmid:29666202|PMID29666202}} | ||
Amniotic fluid is often assessed for both quality and quantity. The volume increases as the fetus grows and rate of change varies during the pregnancy. | Amniotic fluid is often assessed for both quality and quantity. The volume increases as the fetus grows and rate of change varies during the pregnancy. | ||
* up to 8 weeks - increases at the rate of 10 ml/week | * up to 8 weeks - increases at the rate of 10 ml/week | ||
* 8 to 13 weeks - increases at the rate of 25 ml/week | * 8 to 13 weeks - increases at the rate of 25 ml/week | ||
| Line 117: | Line 148: | ||
* Replaced by fetal exhalation and urination. | * Replaced by fetal exhalation and urination. | ||
* Magnesium low levels associated with preeclampsia and diabetes. | * Magnesium low levels associated with preeclampsia and diabetes. | ||
** normal magnesium value at 16 weeks (GA) is 1.65 ± 0.16 mg/dL in amniotic fluid and 1.97 ± 0.23 mg/dL in serum. | ** normal magnesium value at 16 weeks (GA) is 1.65 ± 0.16 mg/dL in amniotic fluid and 1.97 ± 0.23 mg/dL in serum.{{#pmid:21672230|PMID21672230}} | ||
===Amniotic Fluid Swallowing=== | ===Amniotic Fluid Swallowing=== | ||
| Line 128: | Line 159: | ||
==Chorionic Sac== | ==Chorionic Sac== | ||
{{Chorionic sac}}, {{Chorionic cavity}} | |||
[[File:Gray0039.jpg|thumb]] | [[File:Gray0039.jpg|thumb]] | ||
| Line 135: | Line 167: | ||
==Yolk Sac== | ==Yolk Sac== | ||
{{Yolk sac}} | |||
[[File:Endoderm cartoon.jpg]] | [[File:Endoderm cartoon.jpg]] | ||
The ventral endoderm lines and extra-embryonic mesoderm covers the space called the yolk sac (yellow). Folding of the embryonic disc "pinches off" part of this yolk sac forming the first primitive gastrointestinal tract. | The ventral endoderm lines and extra-embryonic mesoderm covers the space called the {{yolk sac}} (yellow). Folding of the embryonic disc "pinches off" part of this yolk sac forming the first primitive gastrointestinal tract. | ||
[[File:Notch and yolk sac blood vessels model.jpg|400px]] | [[File:Notch and yolk sac blood vessels model.jpg|400px]] | ||
Notch and yolk sac blood vessels model | Notch and yolk sac blood vessels model{{#pmid:21352545|PMID21352545}} | ||
:'''Links:''' [[Yolk Sac]] | |||
==Allantois== | ==Allantois== | ||
| Line 150: | Line 186: | ||
A recent comparative study looking at allantois structure in mouse, pig, rabbit and man | A recent comparative study looking at allantois structure in mouse, pig, rabbit and man{{#pmid:28165148|PMID28165148}} found the following: | ||
# tissue interaction between endoderm and mesoderm required for allantoic development and vascular differentiation in species with a rudimentary allantoic diverticulum | # tissue interaction between endoderm and mesoderm required for allantoic development and vascular differentiation in species with a rudimentary allantoic diverticulum | ||
# allantoic mesothelium plays a role in chorioallantoic attachment, allantoic differentiation and vascularization | # allantoic mesothelium plays a role in chorioallantoic attachment, allantoic differentiation and vascularization | ||
| Line 176: | Line 212: | ||
The later the twinning event occurs, the less common are the initially separate placental membranes (diamniotic, dichorionic) and finally resulting in conjoined twins. | The later the twinning event occurs, the less common are the initially separate placental membranes (diamniotic, dichorionic) and finally resulting in conjoined twins. | ||
{ | {{Monoygotic Twinning Table}} | ||
Table based upon{{#pmid:12957099|PMID12957099}} | |||
Table based upon | |||
===Chorioamnionitis=== | ===Chorioamnionitis=== | ||
| Line 304: | Line 226: | ||
===Reviews=== | ===Reviews=== | ||
{{#pmid:20711983}} | |||
{{#pmid:11312634}} | |||
{{#pmid:8671414}} | |||
===Articles=== | ===Articles=== | ||
Latest revision as of 23:38, 1 June 2019
| Embryology - 28 May 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Introduction


The placental membranes is a term often used to describe the all the fetal components of the placenta (Greek, plakuos = flat cake).
This page will not cover the whole placenta, just the development of the extra-embryonic membranes that form the extra-embryonic coeloms (cavities or spaces); amnionic sac, chorionic sac, yolk sac and allantois.
In monozygotic twinning, depending upon when the twinning event occurred, each embryo will either share or have completely separate set of placental membranes.
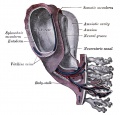
|
Connecting stalk (body stalk) shown to the right linking to the developing placenta. |
Some Recent Findings
|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Placental Membrane Development | Amniotic Membrane Development | Chorionic Membrane Development | Amniotic Fluid |
| Older papers |
|---|
| These papers originally appeared in the Some Recent Findings table, but as that list grew in length have now been shuffled down to this collapsible table.
See also the Discussion Page for other references listed by year and References on this current page.
|
Reading

- Human Embryology (2nd ed.) Larson Chapter 7 p151-188 Heart, Chapter 8 p189-228 Vasculature
- The Developing Human: Clinically Oriented Embryology (6th ed.) Moore and Persaud Chapter 14: p304-349
- Before we Are Born (5th ed.) Moore and Persaud Chapter 12; p241-254
- Essentials of Human Embryology Larson Chapter 7 p97-122 Heart, Chapter 8 p123-146 Vasculature
- Human Embryology Fitzgerald and Fitzgerald Chapter 13-17: p77-111

Day 8 to 9 early (Week 2) extra-embryonic coeloms (cavities)
Movies
|
|
|
|
- Links: Movies
Initial Conceptus Cavities
| <html5media height="580" width="500">File:Chorion 001.mp4</html5media> | blue - epiblast layer yellow - hypoblast layer red cells - extraembryonic mesoderm layer green - trophoblast layer red spaces - blood-filled spaces, maternal lacunae white cells - (left) endometrial gland (right) endometrial epithelium |
Amnionic Sac

The amniotic sac (cavity) is initially lined by ectoderm and covered by extra-embryonic mesoderm. In the human embryo during week 3 to 4, folding of the embryonic disc draws the amniotic membrane ventrally over the embryo leading to the enclosing of the embryo within the amniotic sac. Embryonic and fetal development from this time onward occurs fully enclosed within the amniotic sac floating in the amniotic fluid.
The membrane consists of three layers - epithelial monolayer, acellular connective tissue and fibroblast layer, see review[4]
Epithelial Monolayer
Cuboidal cell epithelium with a basement membrane. These cells are in direct contact with the amniotic fluid.
Secrete
- glycoproteins and collagen fibres to form the basal membrane.
- variety of growth factors and cytokines - epidermal growth factor, vascular endothelial growth factor, keratinocyte growth factor, basic fibroblast growth factor, transforming growth factors alpha and beta (TGF-α and TGF-β), interleukin-8 (IL-8), angiogenin, dipeptidyl peptidase IV (DPPIV/CD26), serine protease inhibitor (serpin) E1, also known as type 1 plasminogen activator inhibitor (PAI-1), insulin-like growth factors.
Connective Tissue
An underlying compact layer without cells of connective tissue bundles of collagen for membrane mechanical strength.
Fibroblast Layer
Under the acellular CT layer lies a thick layer of fibroblast cells forming a stroma.

Yolk sac and amniotic cavity volume week 2 to 3 (stage 5, 6, 7 and 8).
Amniotic Fluid
The amniotic fluid has been described as having several functions:
- cushions the fetus against physical trauma.
- allows fetal growth free from restriction or distortion by the adjacent structures.
- provides a thermally stable environment.
- contributes to respiratory and gastrointestinal development.
- helps prevent infection.
- can provide a short-term source of nutrients and fluid to the embryo.[5]
Amniotic fluid is often assessed for both quality and quantity. The volume increases as the fetus grows and rate of change varies during the pregnancy.
- up to 8 weeks - increases at the rate of 10 ml/week
- 8 to 13 weeks - increases at the rate of 25 ml/week
- 13 to 21 weeks - increases at the rate of 60 ml/week
- 21 to 33 weeks - amniotic volume increase starts decreasing and eventually plateaus.
- 34 weeks (GA) - peaks at about 800 mL.
- 40 weeks (GA) - about 600 mL at term.
Fluid Facts
- Circulated by fetal inhaling and swallowing.
- Replaced by fetal exhalation and urination.
- Magnesium low levels associated with preeclampsia and diabetes.
- normal magnesium value at 16 weeks (GA) is 1.65 ± 0.16 mg/dL in amniotic fluid and 1.97 ± 0.23 mg/dL in serum.[6]
Amniotic Fluid Swallowing
In early embryonic development both the buccopharyngeal and cloacal membranes degenerated, allowing the GIT to be filled with amniotic fluid. Towards the end of the fetal period the fetus is now swallowing approximately 500 ml of amniotic fluid / day.
This swallowed amniotic fluid moves through the GIT from esophagus, to stomach, to small intestine, stopping at the large bowel. In the large bowel the majority of fluid (water) is absorbed, along with electrolytes, glucose, urea and hormones. This process may contribute to fetal nutrition and prepare the GIT for its postnatal function. The process of swallowing amniotic fluid has been suggested to also help regulate fluid volume.
- Links: Amniocentesis
Chorionic Sac
chorionic sac, chorionic cavity

The chorionic sac (cavity) is lined by extra-embryonic mesoderm and covered in trophoblast cells forming villi. In the human embryo during week 3 this space forms outside the yolk sac and surrounding the amniotic sac.
This forms a transient fluid-filled space that is lost by expansion of the amniotic sac, which eventually fuses to the chorionic membrane.
Yolk Sac

The ventral endoderm lines and extra-embryonic mesoderm covers the space called the yolk sac (yellow). Folding of the embryonic disc "pinches off" part of this yolk sac forming the first primitive gastrointestinal tract.

Notch and yolk sac blood vessels model[7]
- Links: Yolk Sac
Allantois
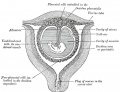
An extra-embryonic membrane, endoderm in origin as an extension from the early hindgut, then cloaca into the connecting stalk of placental animals, connected to the superior end of developing bladder.
In reptiles and birds, acts as a reservoir for wastes and mediates gas exchange. In mammals is associated/incorporated with connecting stalk/placental cord fetal-maternal interface.
A recent comparative study looking at allantois structure in mouse, pig, rabbit and man[8] found the following:
- tissue interaction between endoderm and mesoderm required for allantoic development and vascular differentiation in species with a rudimentary allantoic diverticulum
- allantoic mesothelium plays a role in chorioallantoic attachment, allantoic differentiation and vascularization
- a pronounced diversity in the extraembryonic migratory pathways of primordial germ cells among mammals

Allantois from hindgut

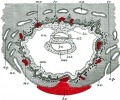
Placental cord cross-section

Placental allantois


Term Membranes

Cannabinoid Receptor 1 (CB1)

Cannabinoid Receptor 2 (CB2)
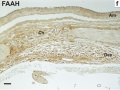
Fatty acid amide hydrolase (FAAH)



Abnormalities
Monoygotic Twinning
Monoygotic twins (identical) produced from a single fertilization event (one fertilised egg and a single spermatazoa, form a single zygote), these twins therefore share the same genetic makeup. Occurs in approximately 3-5 per 1000 pregnancies, more commonly with aged mothers.
The later the twinning event occurs, the less common are the initially separate placental membranes (diamniotic, dichorionic) and finally resulting in conjoined twins.
| Week | Week 1 (GA week 3) | Week 2 (GA week 4) | |||||||||||||
| Day | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 |
| Cell Number | 1 | 1 | 2 | 16 | 32 | 128 | bilaminar | ||||||||
| Event | Ovulation | Fertilization | First cell division | Morula | Early blastocyst | Late blastocyst
Hatching |
Implantation starts | X inactivation | |||||||

|

|

|

|
||||||||||||
| Monoygotic
Twin Type |
Diamniotic
Dichorionic |
Diamniotic
Monochorionic |
Monoamniotic
Monochorionic |
Conjoined | |||||||||||
Table based upon recent a recent twinning review.[9] Links: twinning
Table based upon[9]
Chorioamnionitis
(CA) An intraamniotic puerperal infection described as having 3 forms: histologic, clinical (clinical chorioamnionitis, IAI), and subclinical. Intraamniotic infection is a common (2-4%) event in labor and the systemic inflammatory response can also lead to preterm birth and neonatal complications.
- Links: Placenta - Abnormalities
References
- ↑ Verbruggen SW, Oyen ML, Phillips AT & Nowlan NC. (2017). Function and failure of the fetal membrane: Modelling the mechanics of the chorion and amnion. PLoS ONE , 12, e0171588. PMID: 28350838 DOI.
- ↑ Stern C. (2015). The embryo reunited with its membranes in Göttingen. Development , 142, 2727-9. PMID: 26286940 DOI.
- ↑ Kasuga Y, Miyakoshi K, Ikenoue S, Kadohira I, Matsumoto T, Minegishi K & Yoshimura Y. (2013). Complete chorion-amnion separation presenting as a stuck fetus. Acta Obstet Gynecol Scand , 92, 990-1. PMID: 23647025 DOI.
- ↑ Favaron PO, Carvalho RC, Borghesi J, Anunciação AR & Miglino MA. (2015). The Amniotic Membrane: Development and Potential Applications - A Review. Reprod. Domest. Anim. , 50, 881-92. PMID: 26510939 DOI.
- ↑ Hall NJ, Drewett M & Burge D. (2019). Nutritional role of amniotic fluid: clues from infants with congenital obstruction of the digestive tract. Arch. Dis. Child. Fetal Neonatal Ed. , 104, F199-F201. PMID: 29666202 DOI.
- ↑ Bocos Terraz JP, Izquierdo Álvarez S, Bancalero Flores JL, González López A & Escanero Marcén JF. (2011). Magnesium concentration in amniotic fluid in the early weeks of the second trimester of pregnancy. BMC Res Notes , 4, 185. PMID: 21672230 DOI.
- ↑ Copeland JN, Feng Y, Neradugomma NK, Fields PE & Vivian JL. (2011). Notch signaling regulates remodeling and vessel diameter in the extraembryonic yolk sac. BMC Dev. Biol. , 11, 12. PMID: 21352545 DOI.
- ↑ Hassan W & Viebahn C. (2017). A correlative study of the allantois in pig and rabbit highlighting the diversity of extraembryonic tissues in four mammalian species, including mouse and man. J. Morphol. , 278, 600-620. PMID: 28165148 DOI.
- ↑ 9.0 9.1 Hall JG. (2003). Twinning. Lancet , 362, 735-43. PMID: 12957099 DOI.
Reviews
Tavian M, Biasch K, Sinka L, Vallet J & Péault B. (2010). Embryonic origin of human hematopoiesis. Int. J. Dev. Biol. , 54, 1061-5. PMID: 20711983 DOI.
Burton GJ, Hempstock J & Jauniaux E. (2001). Nutrition of the human fetus during the first trimester--a review. Placenta , 22 Suppl A, S70-7. PMID: 11312634 DOI.
Docherty SM, Iles RK, Wathen N & Chard T. (1996). The temporary anatomical structures prominent in the first trimester may be fulfilling exchange functions assigned to the placenta in the second and third trimester. Hum. Reprod. , 11, 1157-61. PMID: 8671414
Articles
Search PubMed
Search April 2010
- Placental Membranes - All (10083) Review (748) Free Full Text (1728)
Search Pubmed: Placental Membranes | amniotic sac development | chorionic sac development | yolk sac development | allantois development
Additional Images
see all online Placental materials

Placenta and Fetus

Placenta Fetal Side

Placenta Maternal Side





Fetal membrane and placenta cartoon

Placenta spiral artery conversion

Uterine and placental vasculature

Fetal circulation overview

Placental trophospongium

Placenta anchoring villi
Fetal blood
Placental cord cross-section

Placenta_abnormalities

Mouse placenta E16.5

Mouse placenta E16.5

Human placenta viewed from the fetal side

Cord with one artery and one vein

Placenta gene expression




















Terms
| Placenta Terms (expand to view) |
|---|
with an incidence of about 2.8 per 1,000 pregnancies, there is also a rarer form of extra-abdominal varices.PMID 24883288
with an incidence of about 2.8 per 1,000 pregnancies, there is also a rarer form of extra-abdominal varices. PMID 24883288
|
| Other Terms Lists |
|---|
| Terms Lists: ART | Birth | Bone | Cardiovascular | Cell Division | Endocrine | Gastrointestinal | Genital | Genetic | Head | Hearing | Heart | Immune | Integumentary | Neonatal | Neural | Oocyte | Palate | Placenta | Radiation | Renal | Respiratory | Spermatozoa | Statistics | Tooth | Ultrasound | Vision | Historic | Drugs | Glossary |
External Links
External Links Notice - The dynamic nature of the internet may mean that some of these listed links may no longer function. If the link no longer works search the web with the link text or name. Links to any external commercial sites are provided for information purposes only and should never be considered an endorsement. UNSW Embryology is provided as an educational resource with no clinical information or commercial affiliation.
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, May 28) Embryology Placenta - Membranes. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Placenta_-_Membranes
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G