Gastrointestinal Tract - Mesentery Development
| Embryology - 6 May 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Introduction
The adult gastrointestinal tract (GIT) is attached along its length between the stomach and anus by a dorsal mesentery originally formed from splanchnic mesoderm. The majority of the ventral mesentery is developmentally lost at the level of the midgut and only the dorsal mesentery remains in the adult, through which blood vessels, nerves and lymph connects to the gastrointestinal wall.
Recently mouse mesentery has been used as a transplantation site for human intestinal organoid study.[1]
Some Recent Findings
|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Mesentery Embryology <pubmed limit=5>Mesentery Embryology</pubmed> |
| Older papers |
|---|
|
Movies
|
|
Small Intestine
Intestinal Functions
Small Intestine
- absorption of nutrients and minerals found in food
- Duodenum -principal site for iron absorption
Colon
- absorbs fluid, water and salts, from solid wastes
Embryonic Development
Week 4
|
Colour code:
|
Week 7

Human embryo small intestine secondary loops (week 7 to 8).[6]
Week 8
|


Late embryonic small intestine commencing at the duodenum, continuing as ventrally herniated and returning to join the colon.

rectum and bladder

rectum and bladder labeled

rectum

rectum labeled





Small intestine tertiary loops week 8.[6]
- Links: Carnegie stage 22 | Week 8
Rotation
A recent 3 dimensional study[6] has suggested a modified “en-bloc rotation” of the small intestine, compared the the earlier simplified description of 270 degree rotation.
Fetal Intestine Length

|

|
| Fetal small Intestine length growth | Fetal Large Intestine length growth |

Data from[4]
Small Intestine Length
Small intestine growth in length is initially linear (first half pregnancy to 32 cm CRL), followed by rapid growth in the last 15 weeks doubling the overall length. Growth continues postnatally but after 1 year slows again to a linear increase to adulthood.[9]
| Age (weeks GA gestational age) | Average Length (cm) |
| 20 | 125 |
| 30 | 200 |
| term | 275 |
| 1 year postnatal | 380 |
| 5 years | 450 |
| 10 years | 500 |
| 20 years | 575 |
| Table data based upon 8 published reports of necropsy measurement of 1010 guts.[9] | |
Hindgut
Anatomically the distal third of the transverse colon and the splenic flexure, the descending colon, sigmoid colon and rectum. The developmental timing of the anus and rectum formation[10] in human embryos of the Carnegie Collection has been previously carried out (1974). A more recent study[11] has also been made of the Kyoto Collection embryos.
There has been some recent controversy over the "anal membrane" formation.
A recent study hindgut and anorectum development in human embryos shows that WNT5a is active in this region prior to anus formation, when it is down-regulated.[12]
Other studies - [13][14][15][16][17] (rat)
Abnormalities
Intestinal malrotation[18]
Midgut Volvulus[19]
Molecular Factors
Histology
The adult mesentery consists of loose irregular connective tissue, areolar connective tissue, collagen fibres, elastic fibres. There are also numerous mast cells (granulocytes) containing histamine and other substances released during inflammatory and allergic reactions.
| Low power (x10) | High power (x40) |
|---|---|

|

|
References
- ↑ Cortez AR, Poling HM, Brown NE, Singh A, Mahe MM & Helmrath MA. (2018). Transplantation of human intestinal organoids into the mouse mesentery: A more physiologic and anatomic engraftment site. Surgery , 164, 643-650. PMID: 30072255 DOI.
- ↑ Hikspoors JPJM, Kruepunga N, Mommen GMC, Peeters JPWU, Hülsman CJM, Eleonore Köhler S & Lamers WH. (2018). The development of the dorsal mesentery in human embryos and fetuses. Semin. Cell Dev. Biol. , , . PMID: 30142441 DOI.
- ↑ Ueno S, Yamada S, Uwabe C, Männer J, Shiraki N & Takakuwa T. (2016). The Digestive Tract and Derived Primordia Differentiate by Following a Precise Timeline in Human Embryos Between Carnegie Stages 11 and 13. Anat Rec (Hoboken) , 299, 439-49. PMID: 26995337 DOI.
- ↑ 4.0 4.1 Ben-Nun MS, Ben-Shlush A & Raviv Zilka L. (2018). Growth of the colon and rectum throughout gestation: evaluation with fetal MRI. Acta Radiol Open , 7, 2058460118761206. PMID: 29531795 DOI.
- ↑ Wells JM & Spence JR. (2014). How to make an intestine. Development , 141, 752-60. PMID: 24496613 DOI.
- ↑ 6.0 6.1 6.2 Soffers JH, Hikspoors JP, Mekonen HK, Koehler SE & Lamers WH. (2015). The growth pattern of the human intestine and its mesentery. BMC Dev. Biol. , 15, 31. PMID: 26297675 DOI.
- ↑ FitzSimmons J, Chinn A & Shepard TH. (1988). Normal length of the human fetal gastrointestinal tract. Pediatr Pathol , 8, 633-41. PMID: 3244599
- ↑ Archie JG, Collins JS & Lebel RR. (2006). Quantitative standards for fetal and neonatal autopsy. Am. J. Clin. Pathol. , 126, 256-65. PMID: 16891202 DOI.
- ↑ 9.0 9.1 Weaver LT, Austin S & Cole TJ. (1991). Small intestinal length: a factor essential for gut adaptation. Gut , 32, 1321-3. PMID: 1752463
- ↑ de Vries PA. and Friedland GW. The staged sequential development of the anus and rectum in human embryos and fetuses. (1974) J. Pediatr. Surg., 9(5): 755-69 PMID 4424274
- ↑ Hashimoto R. (2013). Development of the human tail bud and splanchnic mesenchyme. Congenit Anom (Kyoto) , 53, 27-33. PMID: 23480355 DOI.
- ↑ Li FF, Zhang T, Bai YZ, Yuan ZW & Wang WL. (2011). Spatiotemporal expression of Wnt5a during the development of the hindgut and anorectum in human embryos. Int J Colorectal Dis , 26, 983-8. PMID: 21431850 DOI.
- ↑ van der Putte SC. (2009). The development of the human anorectum. Anat Rec (Hoboken) , 292, 951-4. PMID: 19496155 DOI.
- ↑ Kromer P. (1999). Further study of the urorectal septum in staged human embryos. Folia Morphol. (Warsz) , 58, 53-63. PMID: 10504783
- ↑ Nievelstein RA, van der Werff JF, Verbeek FJ, Valk J & Vermeij-Keers C. (1998). Normal and abnormal embryonic development of the anorectum in human embryos. Teratology , 57, 70-8. PMID: 9562679 <70::AID-TERA5>3.0.CO;2-A DOI.
- ↑ Kromer P. (1996). Development of the urorectal septum and differentiation of the urogenital sinus in human embryos of stages 13 to 19. Folia Morphol. (Warsz) , 55, 362-3. PMID: 9243909
- ↑ Kluth D, Fiegel HC & Metzger R. (2011). Embryology of the hindgut. Semin. Pediatr. Surg. , 20, 152-60. PMID: 21708335 DOI.
- ↑ Ezer SS, Oguzkurt P, Temiz A, Ince E, Gezer HO, Demir S & Hicsonmez A. (2016). Intestinal malrotation needs immediate consideration and investigation. Pediatr Int , 58, 1200-1204. PMID: 27353636 DOI.
- ↑ Coste AH & Bhimji SS. (2018). Midgut Volvulus. , , . PMID: 28722991
Reviews
Wells JM & Spence JR. (2014). How to make an intestine. Development , 141, 752-60. PMID: 24496613 DOI.
Noah TK, Donahue B & Shroyer NF. (2011). Intestinal development and differentiation. Exp. Cell Res. , 317, 2702-10. PMID: 21978911 DOI.
Burns AJ, Roberts RR, Bornstein JC & Young HM. (2009). Development of the enteric nervous system and its role in intestinal motility during fetal and early postnatal stages. Semin. Pediatr. Surg. , 18, 196-205. PMID: 19782301 DOI.
Articles
Cho BH, Kim JH, Jin ZW, Wilting J, Rodríguez-Vázquez JF & Murakami G. (2018). Topographical anatomy of the intestines during in utero physiological herniation. Clin Anat , 31, 583-592. PMID: 29044646 DOI.
Nerurkar NL, Mahadevan L & Tabin CJ. (2017). BMP signaling controls buckling forces to modulate looping morphogenesis of the gut. Proc. Natl. Acad. Sci. U.S.A. , 114, 2277-2282. PMID: 28193855 DOI.
Soffers JH, Hikspoors JP, Mekonen HK, Koehler SE & Lamers WH. (2015). The growth pattern of the human intestine and its mesentery. BMC Dev. Biol. , 15, 31. PMID: 26297675 DOI.
Coffey JC, Culligan K, Walsh LG, Sehgal R, Dunne C, McGrath D, Walsh D, Moore M, Staunton M, Scanlon T, Dewhurst C, Kenny B, O'Riordan C, O'Brien JM, Quondamatteo F & Dockery P. (2016). An appraisal of the computed axial tomographic appearance of the human mesentery based on mesenteric contiguity from the duodenojejunal flexure to the mesorectal level. Eur Radiol , 26, 714-21. PMID: 26186959 DOI.
Davis NM, Kurpios NA, Sun X, Gros J, Martin JF & Tabin CJ. (2008). The chirality of gut rotation derives from left-right asymmetric changes in the architecture of the dorsal mesentery. Dev. Cell , 15, 134-45. PMID: 18606147 DOI.
Cascio S, Tien AS, Agarwal P & Tan HL. (2006). Dorsal mesenteric agenesis without small bowel atresia: a rare cause of midgut volvulus in children. J. Pediatr. Surg. , 41, E5-7. PMID: 16952580 DOI.
Search Pubmed
Search Bookshelf Mesentery Development
Search Pubmed Now: Mesentery Embryology | Mesentery Development
Additional Images
Historic Images
| Historic Disclaimer - information about historic embryology pages |
|---|
|
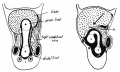
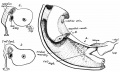
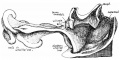
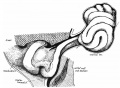
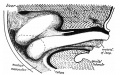
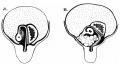
Frazer JE. and Robbins RH. On the factors concerned in causing rotation of the intestine in man. (1915) J Anat. 50(1): 75-110. PMID 17233053
- Intestine Development

1 embryo 5 mm
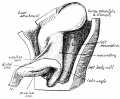
2 embryo 8 mm
3 vitello-umbilical anastomosis

4 proximal limb of loop

5 curve of the duodenum
6 embryo 7.5 mm

7 mesentery

8 embryo 35 mm
9 embryo 28 mm
10 embryo 35 mm
11 embryo 22 mm
12 liver lobes and bowel

13 returning proximal limb of loop

14 embryo 45 mm

15 before and after bowel return

16 fetus 63 mm

17 left abdomen

18 colon at different periods


















{kind=link}
External Links
External Links Notice - The dynamic nature of the internet may mean that some of these listed links may no longer function. If the link no longer works search the web with the link text or name. Links to any external commercial sites are provided for information purposes only and should never be considered an endorsement. UNSW Embryology is provided as an educational resource with no clinical information or commercial affiliation.
- NIH PubMed Health Short Bowel Syndrome
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, May 6) Embryology Gastrointestinal Tract - Mesentery Development. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Gastrointestinal_Tract_-_Mesentery_Development
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G