|
|
| (33 intermediate revisions by the same user not shown) |
| Line 1: |
Line 1: |
| {{Header}} | | {{Header}} |
| ==Introduction== | | ==Introduction== |
| [[File:Placental cord cross-section.jpg|thumb|Human placental cord cross-section]] | | [[File:HillH5 Stage 16 bf16.gif|right|HillH5 "Baxter" embryo (G.L.) CRL 9.5 mm ventral view detail animation (stereo pair [[:File:HillH5 Stage 16 bf07.jpg|right]] | [[:File:HillH5 Stage 16 bf08.jpg|left]])]] |
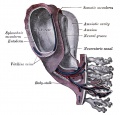
| The placenta (Greek, ''plakuos'' = flat cake) named on the basis of this organs appearance. The placental cord (umbilical cord) is the connecting region between the functional placenta and the embryo/fetal umbilical region. The human cord varies greatly in overall length increasing to about 60 to 70 cm at term. This extraembryonic structure contains the placental blood vessels and allantois. | | [[File:Placental cord cross-section.jpg|thumb|alt=Histology Human placental cord cross-section|Human placental cord cross-section]] |
| | The placenta (Greek, ''plakuos'' = flat cake) named on the basis of this organs appearance. The {{placental cord}} ({{umbilical cord}}) is the connecting region between the functional placenta and the embryo/fetal umbilical region. The human cord varies greatly in overall length increasing to about 60 to 70 cm at term. This extra-embryonic structure contains the main placental blood vessels (one vein and two arteries), the {{yolk stalk}} ({{omphalomesenteric duct}}), and the {{allantois}}. |
|
| |
|
| There are essentially 3 separate aortic/venous circulatory systems: umbilical, systemic and vitelline. The umbilical system is lost at birth, the vitelline contributes to the portal system and the systemic (embryonic) is extensively remodelled to fom the the cardiovascular system. | | |
| | There are essentially 3 separate aortic/venous circulatory systems: umbilical, systemic and vitelline. In the human cord, only the left placental (umbilical) vein persists, while the right placental (umbilical) vein degenerates. The initial segment of the cord at the "umbilicus" also contains the mid-gut herniation, present during the embryonic period of development. |
| | |
| | The umbilical system is lost at birth, the vitelline contributes to the portal system and the systemic (embryonic) is extensively remodelled to form the cardiovascular system. |
|
| |
|
|
| |
|
| Line 10: |
Line 14: |
|
| |
|
| == Some Recent Findings == | | == Some Recent Findings == |
| | | [[File:Stage17 model 02.jpg|thumb|alt=Model of the Human Embryo|Human Embryo Cord Model ([[Carnegie stage 17|stage 17]]]] |
| {| | | {| |
| |-bgcolor="F5FAFF" | | |-bgcolor="F5FAFF" |
| | | | | |
| * '''Human Chorionic Gonadotropin Induces Human Macrophages to Form Intracytoplasmic Vacuoles Mimicking Hofbauer Cells in Human Chorionic Villi'''<ref name="PMID23128164"><pubmed>23128164</pubmed></ref> The most characteristic morphological feature of macrophages in the stroma of placental villi, known as Hofbauer cells, is their highly vacuolated appearance. They also show positive immunostaining for human chorionic gonadotropin (hCG)." | | * '''Persistent right umbilical vein: a study using serial sections of human embryos and fetuses'''{{#pmid:30310717|PMID30310717}} "Persistent right umbilical vein (PRUV) is a common anomaly of the venous system. Although candidates for future PRUV were expected to occur more frequently in earlier specimens, evaluation of serial horizontal sections from 58 embryos and fetuses of gestational age 5-7 weeks found that only two of these embryos and fetuses were candidates for anomalies. In a specimen, a degenerating right umbilical vein (UV) joined the thick left UV in a narrow peritoneal space between the liver and abdominal cavity, and in the other specimen, a degenerating left UV joined a thick right UV in the abdominal wall near the liver. In these two specimens, the UV drained into the normal, umbilical portion of the left liver. These results strongly suggested that, other than the usual PRUV draining into the right liver, another type of PRUV was likely to consist of the right UV draining into the left liver." |
|
| |
|
| * '''Hofbauer cells in early human placenta: possible implications in vasculogenesis and angiogenesis'''<ref><pubmed>17350092</pubmed></ref> "The stroma of the placental villi contain numerous macrophages, so-called Hofbauer cells which are of mesenchymal origin and are thought to function in many processes. ...Double immunohistochemistry staining with CD31/PECAM1 and CD68 was applied to placental tissues. In placental villous core, majority of the Hofbauer cells were found to be either in close contact with angiogenic cell cords and primitive vascular tubes or located in between them. Moreover, the number of Hofbauer cells and vasculogenic structures were found to be significantly correlated. The findings of this study suggest for the first time that Hofbauer cells might be involved in the processes of vasculogenesis and angiogenesis in the placenta." | | * '''Human Chorionic Gonadotropin Induces Human Macrophages to Form Intracytoplasmic Vacuoles Mimicking Hofbauer Cells in Human Chorionic Villi'''{{#pmid:23128164|PMID23128164}} The most characteristic morphological feature of macrophages in the stroma of placental villi, known as Hofbauer cells, is their highly vacuolated appearance. They also show positive immunostaining for human chorionic gonadotropin (hCG)." |
|
| |
|
| |} | | |} |
| {| class="wikitable collapsible collapsed" | | {| class="wikitable mw-collapsible mw-collapsed" |
| ! More recent papers | | ! More recent papers |
| |- | | |- |
| | [[File:Mark_Hill.jpg|90px|left]] {{Most_Recent_Refs}} | | | [[File:Mark_Hill.jpg|90px|left]] {{Most_Recent_Refs}} |
|
| |
|
| Search term: [http://www.ncbi.nlm.nih.gov/pubmed/?term=Placental+Cord ''Placental Cord''] | | Search term: [http://www.ncbi.nlm.nih.gov/pubmed/?term=Placental+Cord ''Placental Cord''] | [http://www.ncbi.nlm.nih.gov/pubmed/?term=Umbilical+Cord ''Umbilical Cord''] | [http://www.ncbi.nlm.nih.gov/pubmed/?term=Placental+Artery ''Placental Artery''] | [http://www.ncbi.nlm.nih.gov/pubmed/?term=Placental+Vein ''Placental Vein''] | [http://www.ncbi.nlm.nih.gov/pubmed/?term=Hofbauer+cell ''Hofbauer cell''] | [http://www.ncbi.nlm.nih.gov/pubmed/?term=single+umbilical+artery ''single umbilical artery''] | [http://www.ncbi.nlm.nih.gov/pubmed/?term=Persistent+right+umbilical+vein ''Persistent right umbilical vein''] |
|
| |
|
| <pubmed limit=5>Placental Cord</pubmed>
| | |} |
| | {| class="wikitable mw-collapsible mw-collapsed" |
| | ! Older papers |
| | |- |
| | | {{Older papers}} |
| | * '''Hofbauer cells in early human placenta: possible implications in vasculogenesis and angiogenesis'''{{#pmid:17350092|PMID17350092}} "The stroma of the placental villi contain numerous macrophages, so-called Hofbauer cells which are of mesenchymal origin and are thought to function in many processes. ...Double immunohistochemistry staining with CD31/PECAM1 and CD68 was applied to placental tissues. In placental villous core, majority of the Hofbauer cells were found to be either in close contact with angiogenic cell cords and primitive vascular tubes or located in between them. Moreover, the number of Hofbauer cells and vasculogenic structures were found to be significantly correlated. The findings of this study suggest for the first time that Hofbauer cells might be involved in the processes of vasculogenesis and angiogenesis in the placenta." |
| |} | | |} |
| ==Hofbauer Cells== | | ==Hofbauer Cells== |
| | {| |
| | | [[File:Placenta_Hofbauer_cells_01.jpg|alt=Hofbauer Cells|300px]] |
| | Hofbauer Cells (red asterisks){{#pmid:22606231|PMID22606231}} |
| | | |
| * human villous macrophages | | * human villous macrophages |
| * highly vacuolated cells | | * highly vacuolated cells |
| Line 35: |
Line 48: |
| * possible paracrine role for early stages of placental vasculogenesis | | * possible paracrine role for early stages of placental vasculogenesis |
| * express angiogenic growth factors (VEGF) | | * express angiogenic growth factors (VEGF) |
| | |} |
| | {| class="wikitable mw-collapsible mw-collapsed" |
| | ! [[Embryology_History|Historic Embryology]] - Hofbauer Cells |
| | |- |
| | | [[Book_-_Contributions_to_Embryology_Carnegie_Institution_No.56-14|Chapter 14. Hofbauer Cells in Normal and Pathologic Conceptuses]] Contributions to Embryology Carnegie Institution No.56 (1921) |
| | <gallery> |
| | File:Mall_Meyer1921_fig235.jpg|Fig. 235. Transition forms between mesenchyme and Hofbauer cells. No. 645, slide 3. X330. |
| | File:Mall_Meyer1921_fig236.jpg|Fig. 236. Transition forms between mesenchyme and Hofbauer cells. No. 592, slide 1. X330. |
| | File:Mall_Meyer1921_fig237.jpg|Fig. 237. Transition forms between mesenchyme and Hofbauer cells. No. 645, slide 3b. X330. |
| | File:Mall_Meyer1921_fig238.jpg|Fig. 238. A phagocytic pseudo-Hofbauer cell. No. 645, slide 2. X650. |
| | File:Mall_Meyer1921_fig239.jpg|Fig. 239. Fusing Hofbauer cells forming a giant cell. No. 645, slide 2. X300. |
| | File:Mall_Meyer1921_fig240.jpg|Fig. 240. Fusing Hofbauer cells forming a giant cell. No. 985, slide 1. X300. |
| | File:Mall_Meyer1921_fig241.jpg|Fig. 241. Pseudo-Hofbauer cells in the ovary. No. 970. X650. |
| | </gallery> |
|
| |
|
| | {{Historic Disclaimer}} |
| | |} |
| ==Wharton's Jelly== | | ==Wharton's Jelly== |
| [[File:Placental_cord_cross-section.jpg|thumb|Placental cord cross-section]] | | {| |
| | | [[File:Placental cord 01.jpg|300px]] |
| | |
| | Placental cord cross-section showing Wharton's Jelly |
| | | First described and named after Thomas Wharton (1614–1673) an English physician and anatomist. |
| * placental cord connective tissue (''substantia gelatinea funiculi umbilicalis'') | | * placental cord connective tissue (''substantia gelatinea funiculi umbilicalis'') |
| * amorphous substance containing glycosaminoglycans, proteoglycans and hyaluronic acid. | | * amorphous substance containing glycosaminoglycans, proteoglycans and hyaluronic acid. |
| Line 43: |
Line 76: |
| * network of collagen that form canaliculi and perivascular spaces. | | * network of collagen that form canaliculi and perivascular spaces. |
| * maintain blood flow to the fetus during placental cord compression during pregnancy or delivery. | | * maintain blood flow to the fetus during placental cord compression during pregnancy or delivery. |
| | | |} |
| First described and named after Thomas Wharton (1614–1673) an English physician and anatomist.
| |
|
| |
|
| ==Placental Cord Histology== | | ==Placental Cord Histology== |
| Line 54: |
Line 86: |
| </gallery> | | </gallery> |
|
| |
|
| ==Persistent Right Umbilical Vein==
| | [[File:Hubrecht Homo73a cord 1.jpg|600px]] |
|
| |
|
| A fairly rare anomaly, a study of 15,237 obstetric ultrasound examinations performed after 15 weeks' gestation identified only 33 cases of persistent right umbilical vein.<ref><pubmed>7970470</pubmed></ref> Some studies have identified associated fetal anomalies with this condition.<ref><pubmed>20922781</pubmed></ref>
| | Human placental cord (3.5 month) cross-section. |
|
| |
|
| ==Cord Length== | | ==Cord Length== |
| Line 66: |
Line 98: |
|
| |
|
| ==Cord Coiling== | | ==Cord Coiling== |
| A recent review of the published literature on cord coiling.<ref><pubmed>16076615</pubmed></ref> | | |
| | A recent review of the published literature on cord coiling{{#pmid:24259031|PMID24259031}} states: "Previous studies that draw a link between abnormal cord coiling and clinical outcome are generally too small and/or selective to allow meaningful conclusions or applicability to low-risk populations." |
| | |
| | The following suggested associations{{#pmid:16076615|PMID16076615}} should therefore be reconsidered. |
| * '''Hypocoiling''' - associated with increased incidence of fetal demise, intrapartum fetal heart rate decelerations, operative delivery for fetal distress, anatomic-karyotypic abnormalities and chorio-amnionitis. | | * '''Hypocoiling''' - associated with increased incidence of fetal demise, intrapartum fetal heart rate decelerations, operative delivery for fetal distress, anatomic-karyotypic abnormalities and chorio-amnionitis. |
| * '''Hypercoiling''' - associated with increased incidence of fetal growth restriction, intrapartum fetal heart rate decelerations, vascular thrombosis and cord stenosis. | | * '''Hypercoiling''' - associated with increased incidence of fetal growth restriction, intrapartum fetal heart rate decelerations, vascular thrombosis and cord stenosis. |
| Line 73: |
Line 108: |
| [[File:Placental_cord_ultrasound_03.jpg]] | | [[File:Placental_cord_ultrasound_03.jpg]] |
|
| |
|
| There are a number of analyses that can be made by ultrasound scanning of the fetal placental cord. Some detected abnormalities (blood vessel number, blood flow<ref><pubmed>24277892</pubmed></ref>) have been associated with adverse developmental outcomes. | | There are a number of analyses that can be made by ultrasound scanning of the fetal placental cord. Some detected abnormalities (blood vessel number, blood flow{{#pmid:24277892|PMID24277892}}) have been associated with adverse developmental outcomes. |
| * Quantification of cord length, diameter, structural abnormalities. | | * Quantification of cord length, diameter, structural abnormalities. |
| * Quantification of placental blood vessel number and size. | | * Quantification of placental blood vessel number and size. |
| Line 86: |
Line 121: |
| ===Cord Vessel Number=== | | ===Cord Vessel Number=== |
| [[File:Placental_cord_ultrasound_02.jpg|thumb|Cord with one artery and one vein]] | | [[File:Placental_cord_ultrasound_02.jpg|thumb|Cord with one artery and one vein]] |
| | |
| | ===Persistent Right Umbilical Vein=== |
| | |
| | Persistent right umbilical vein (PRUV) is a fairly rare anomaly, that can be diagnosed using a transverse section of the fetal abdomen or by three-dimensional ultrasound. A study of 15,237 obstetric ultrasound examinations performed after 15 weeks' gestation identified only 33 cases.{{#pmid:7970470|PMID7970470}} While a recent Australian study{{#pmid:29498037|PMID29498037}} in their population was 12/2360 = 0.5%, and was also higher than in other retrospective studies. |
| | |
| | |
| | Some studies have identified associated fetal anomalies with this condition{{#pmid:20922781|PMID20922781}}, including {{cardiac abnormalities}}.{{#pmid:26635256|PMID26635256}} |
| | |
|
| |
|
| ===Cord Knotting=== | | ===Cord Knotting=== |
| Line 95: |
Line 138: |
| Cord knotting can also occur (1%) in most cases these knots have no effect, in some cases of severe knotting this can prevents the passage of placental blood. | | Cord knotting can also occur (1%) in most cases these knots have no effect, in some cases of severe knotting this can prevents the passage of placental blood. |
|
| |
|
| ===Umbilical cord torsion=== | | ===Umbilical Cord Torsion=== |
| | |
| | Rare umbilical cord torsion, even without knot formation can also affect placental blood flow, even leading to fetal demise.{{#pmid:7966052|PMID7966052}} |
| | |
| | ===Fetal Umbilical Vein Varix=== |
| | |
| | Fetal intra-abdominal umbilical vein varix (FIUV, umbilical vein varix) is a focal dilatation of the umbilical venous diameter at the level of cord insertion. The dilatation diameter has been shown to increase linearly with gestational age. Represent about 4% of umbilical cord abnormalities with an incidence of about 2.8 per 1,000 pregnancies.{{#pmid:24883288|PMID24883288}} There is also a rarer form of extra-abdominal varices, where the focal dilatation lies outside the fetal body wall.{{#pmid:31061189|PMID31061189}} |
|
| |
|
| Rare umbilical cord torsion, even without knot formation can also affect placental blood flow, even leading to fetal demise.<ref><pubmed>7966052 </pubmed></ref>
| | {| |
| | |+ '''Fetal intra-abdominal umbilical vein varix'''{{#pmid:24883288|PMID24883288}} |
| | | colspan=2|[[File:Fetal intra-abdominal umbilical vein varix ultrasound 01.jpg|600px]] |
| | |- |
| | ! (A) Ultrasound transverse view of the lower fetal abdomen |
| | ! (B) Color Doppler |
| | |- |
| | | Showing an umbilical vein varix that was approximately 16.9 mm at 33 weeks of gestation. |
| | | Shows some turbulence in the intravascular area and differentiates from other cystic lesions. BL, bladder; VAR, fetal umbilical vein varix. |
| | |} |
|
| |
|
| ===Cord Length=== | | ===Cord Length=== |
| Line 105: |
Line 163: |
|
| |
|
| ===Reviews=== | | ===Reviews=== |
| | {{#pmid:29498037}} |
| | |
| | |
|
| |
|
| ===Articles=== | | ===Articles=== |
| Line 117: |
Line 178: |
|
| |
|
| ==Additional Images== | | ==Additional Images== |
| | [[:Category:Placenta|see all online Placental materials]] |
| | |
| | ===Historic=== |
| | {{Historic Disclaimer}} |
|
| |
|
| [[:Category:Placenta|see all online Placental materials]] | | {{Ref-Cullen1916}} [[Book - Umbilicus (1916) 1|Chapter I. Embryology of the Umbilical Region]] |
| | |
| | <gallery caption="Cross-section of the Cord"> |
| | File:Cullen1916 fig16.jpg|Fig. 16 Embryo 6.5 cm |
| | File:Cullen1916 fig17.jpg|Fig. 17 Embryo 7.5 cm |
| | File:Cullen1916 fig18.jpg|Fig. 18 Embryo 9.0 cm |
| | File:Cullen1916 fig19.jpg|Fig. 19 Embryo 10.0 cm |
| | File:Cullen1916 fig20.jpg|Fig. 20 Embryo 12.0 cm |
| | File:Cullen1916 fig21.jpg|Fig. 21 Embryo 12.0 cm |
| | File:Cullen1916 fig22.jpg|Fig. 22 Embryo 12.0 cm |
| | File:Cullen1916 fig23.jpg|Fig. 23 Embryo 12.0 cm |
| | File:Cullen1916 fig24.jpg|Fig. 24 Embryo 15.0 cm |
| | File:Cullen1916 fig32.jpg|Fig. 32 Term Fetus Cord and Placenta |
| | File:Cullen1916 fig33.jpg|Fig. 33 Term Fetus Umbilical Region |
| | </gallery> |
|
| |
|
| <gallery> | | <gallery> |
| Line 128: |
Line 207: |
| File:Gray0038.jpg | | File:Gray0038.jpg |
| File:Gray0039.jpg | | File:Gray0039.jpg |
| | File:Gray0502.jpg|Fetal circulation overview |
| | </gallery> |
| | |
| | <gallery> |
| File:Fetal membrane and placenta cartoon.jpg | | File:Fetal membrane and placenta cartoon.jpg |
| File:Uterine and placental vasculature.jpg | | File:Uterine and placental vasculature.jpg |
| File:Gray0502.jpg|Fetal circulation overview
| |
| File:Fetalblood.jpg | | File:Fetalblood.jpg |
| File:Placental_cord_cross-section.jpg | | File:Placental_cord_cross-section.jpg |
| </gallery> | | </gallery> |
| | | <br> |
| | | {{Placenta terms}} |
|
| |
|
| {{Glossary}} | | {{Glossary}} |
|
| |
|
| |
|
| |
|
| {{Footer}} | | {{Footer}} |
| | | [[Category:Placenta]][[Category:System Development]] |
| [[Category:Placenta]] [[Category:System Development]] | |
Introduction
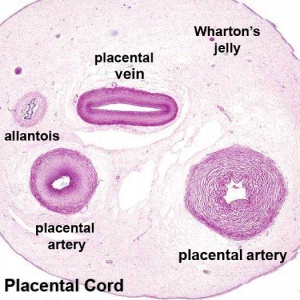
Human placental cord cross-section
The placenta (Greek, plakuos = flat cake) named on the basis of this organs appearance. The placental cord (umbilical cord) is the connecting region between the functional placenta and the embryo/fetal umbilical region. The human cord varies greatly in overall length increasing to about 60 to 70 cm at term. This extra-embryonic structure contains the main placental blood vessels (one vein and two arteries), the yolk stalk (omphalomesenteric duct), and the allantois.
There are essentially 3 separate aortic/venous circulatory systems: umbilical, systemic and vitelline. In the human cord, only the left placental (umbilical) vein persists, while the right placental (umbilical) vein degenerates. The initial segment of the cord at the "umbilicus" also contains the mid-gut herniation, present during the embryonic period of development.
The umbilical system is lost at birth, the vitelline contributes to the portal system and the systemic (embryonic) is extensively remodelled to form the cardiovascular system.
Some Recent Findings
- Persistent right umbilical vein: a study using serial sections of human embryos and fetuses[1] "Persistent right umbilical vein (PRUV) is a common anomaly of the venous system. Although candidates for future PRUV were expected to occur more frequently in earlier specimens, evaluation of serial horizontal sections from 58 embryos and fetuses of gestational age 5-7 weeks found that only two of these embryos and fetuses were candidates for anomalies. In a specimen, a degenerating right umbilical vein (UV) joined the thick left UV in a narrow peritoneal space between the liver and abdominal cavity, and in the other specimen, a degenerating left UV joined a thick right UV in the abdominal wall near the liver. In these two specimens, the UV drained into the normal, umbilical portion of the left liver. These results strongly suggested that, other than the usual PRUV draining into the right liver, another type of PRUV was likely to consist of the right UV draining into the left liver."
- Human Chorionic Gonadotropin Induces Human Macrophages to Form Intracytoplasmic Vacuoles Mimicking Hofbauer Cells in Human Chorionic Villi[2] The most characteristic morphological feature of macrophages in the stroma of placental villi, known as Hofbauer cells, is their highly vacuolated appearance. They also show positive immunostaining for human chorionic gonadotropin (hCG)."
|
| Older papers
|
| These papers originally appeared in the Some Recent Findings table, but as that list grew in length have now been shuffled down to this collapsible table.
See also the Discussion Page for other references listed by year and References on this current page.
- Hofbauer cells in early human placenta: possible implications in vasculogenesis and angiogenesis[3] "The stroma of the placental villi contain numerous macrophages, so-called Hofbauer cells which are of mesenchymal origin and are thought to function in many processes. ...Double immunohistochemistry staining with CD31/PECAM1 and CD68 was applied to placental tissues. In placental villous core, majority of the Hofbauer cells were found to be either in close contact with angiogenic cell cords and primitive vascular tubes or located in between them. Moreover, the number of Hofbauer cells and vasculogenic structures were found to be significantly correlated. The findings of this study suggest for the first time that Hofbauer cells might be involved in the processes of vasculogenesis and angiogenesis in the placenta."
|
Hofbauer Cells

Hofbauer Cells (red asterisks)[4]
|
- human villous macrophages
- highly vacuolated cells
- located the core of placental villi
- macrophages with micropinocytotic activity and phagocytosis ability
- possible paracrine role for early stages of placental vasculogenesis
- express angiogenic growth factors (VEGF)
|
| Historic Embryology - Hofbauer Cells
|
Chapter 14. Hofbauer Cells in Normal and Pathologic Conceptuses Contributions to Embryology Carnegie Institution No.56 (1921)
Fig. 235. Transition forms between mesenchyme and Hofbauer cells. No. 645, slide 3. X330.
Fig. 236. Transition forms between mesenchyme and Hofbauer cells. No. 592, slide 1. X330.
Fig. 237. Transition forms between mesenchyme and Hofbauer cells. No. 645, slide 3b. X330.
Fig. 238. A phagocytic pseudo-Hofbauer cell. No. 645, slide 2. X650.
Fig. 239. Fusing Hofbauer cells forming a giant cell. No. 645, slide 2. X300.
Fig. 240. Fusing Hofbauer cells forming a giant cell. No. 985, slide 1. X300.
Fig. 241. Pseudo-Hofbauer cells in the ovary. No. 970. X650.
| Historic Disclaimer - information about historic embryology pages
|
| Pages where the terms "Historic" (textbooks, papers, people, recommendations) appear on this site, and sections within pages where this disclaimer appears, indicate that the content and scientific understanding are specific to the time of publication. This means that while some scientific descriptions are still accurate, the terminology and interpretation of the developmental mechanisms reflect the understanding at the time of original publication and those of the preceding periods, these terms, interpretations and recommendations may not reflect our current scientific understanding. (More? Embryology History | Historic Embryology Papers)
|
|
Wharton's Jelly
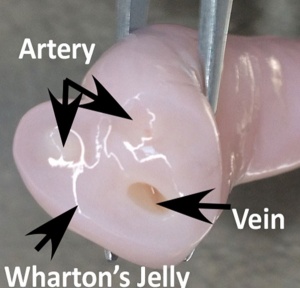
Placental cord cross-section showing Wharton's Jelly
|
First described and named after Thomas Wharton (1614–1673) an English physician and anatomist.
- placental cord connective tissue (substantia gelatinea funiculi umbilicalis)
- amorphous substance containing glycosaminoglycans, proteoglycans and hyaluronic acid.
- cells similar to smooth muscle that allows a contractile function.
- network of collagen that form canaliculi and perivascular spaces.
- maintain blood flow to the fetus during placental cord compression during pregnancy or delivery.
|
Placental Cord Histology
Placental cord cross-section
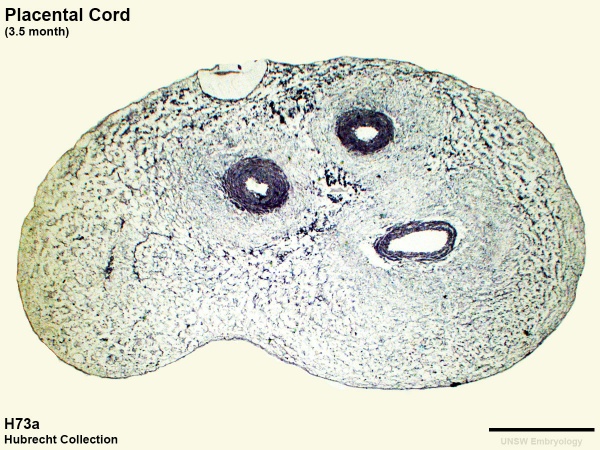
Human placental cord (3.5 month) cross-section.
Cord Length
The following are lengths and classifications at term.
- Normal range - 50 to 60 cm.
- Short cord - less than 35 cm.
- Long cords - over 70 cm can be associated with wrapping around the fetus and other abnormalities.[5]
Cord Coiling
A recent review of the published literature on cord coiling[6] states: "Previous studies that draw a link between abnormal cord coiling and clinical outcome are generally too small and/or selective to allow meaningful conclusions or applicability to low-risk populations."
The following suggested associations[7] should therefore be reconsidered.
- Hypocoiling - associated with increased incidence of fetal demise, intrapartum fetal heart rate decelerations, operative delivery for fetal distress, anatomic-karyotypic abnormalities and chorio-amnionitis.
- Hypercoiling - associated with increased incidence of fetal growth restriction, intrapartum fetal heart rate decelerations, vascular thrombosis and cord stenosis.
Placental Cord Ultrasound
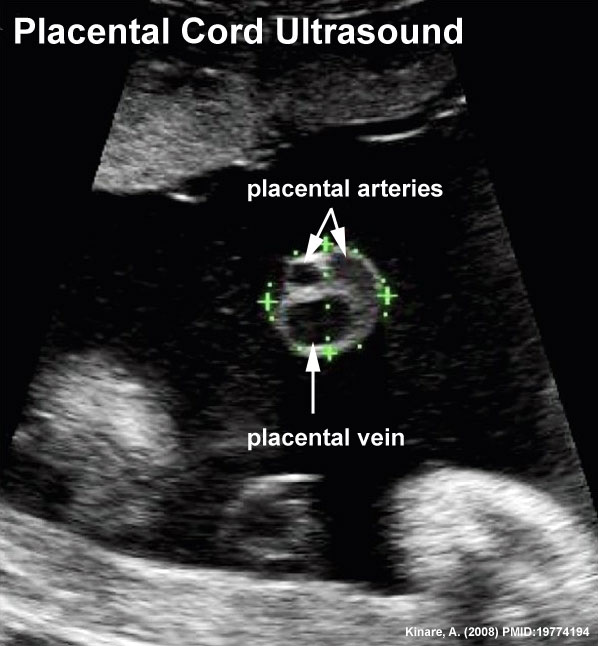
There are a number of analyses that can be made by ultrasound scanning of the fetal placental cord. Some detected abnormalities (blood vessel number, blood flow[8]) have been associated with adverse developmental outcomes.
- Quantification of cord length, diameter, structural abnormalities.
- Quantification of placental blood vessel number and size.
- Quantification of uterine artery blood flow (doppler analysis).
Ultrasound image of transverse scan through the cord show the method of estimation of the cross-sectional area.

Cord Abnormalities
Cord Vessel Number

Cord with one artery and one vein
Persistent Right Umbilical Vein
Persistent right umbilical vein (PRUV) is a fairly rare anomaly, that can be diagnosed using a transverse section of the fetal abdomen or by three-dimensional ultrasound. A study of 15,237 obstetric ultrasound examinations performed after 15 weeks' gestation identified only 33 cases.[9] While a recent Australian study[10] in their population was 12/2360 = 0.5%, and was also higher than in other retrospective studies.
Some studies have identified associated fetal anomalies with this condition[11], including Template:Cardiac abnormalities.[12]
Cord Knotting
There are few abnormalities associated with umbilical cord development, other that abnormally short or long cords, which in most cases do not cause difficulties.
In some cases though, long cords can wrap around limbs or the fetus neck, which can then restrict blood flow or lead to tissue or nerve damage, and therefore effect develoment.
Cord knotting can also occur (1%) in most cases these knots have no effect, in some cases of severe knotting this can prevents the passage of placental blood.
Umbilical Cord Torsion
Rare umbilical cord torsion, even without knot formation can also affect placental blood flow, even leading to fetal demise.[13]
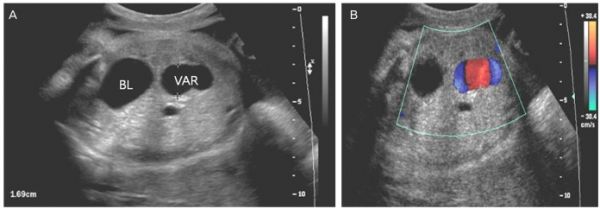
Fetal Umbilical Vein Varix
Fetal intra-abdominal umbilical vein varix (FIUV, umbilical vein varix) is a focal dilatation of the umbilical venous diameter at the level of cord insertion. The dilatation diameter has been shown to increase linearly with gestational age. Represent about 4% of umbilical cord abnormalities with an incidence of about 2.8 per 1,000 pregnancies.[14] There is also a rarer form of extra-abdominal varices, where the focal dilatation lies outside the fetal body wall.[15]
Fetal intra-abdominal umbilical vein varix[14]
|
| (A) Ultrasound transverse view of the lower fetal abdomen
|
(B) Color Doppler
|
| Showing an umbilical vein varix that was approximately 16.9 mm at 33 weeks of gestation.
|
Shows some turbulence in the intravascular area and differentiates from other cystic lesions. BL, bladder; VAR, fetal umbilical vein varix.
|
Cord Length
References
- ↑ Kim JH, Jin ZW, Murakami G, Chai OH & Rodríguez-Vázquez JF. (2018). Persistent right umbilical vein: a study using serial sections of human embryos and fetuses. Anat Cell Biol , 51, 218-222. PMID: 30310717 DOI.
- ↑ Yamaguchi M, Ohba T, Tashiro H, Yamada G & Katabuchi H. (2013). Human chorionic gonadotropin induces human macrophages to form intracytoplasmic vacuoles mimicking Hofbauer cells in human chorionic villi. Cells Tissues Organs (Print) , 197, 127-35. PMID: 23128164 DOI.
- ↑ Seval Y, Korgun ET & Demir R. (2007). Hofbauer cells in early human placenta: possible implications in vasculogenesis and angiogenesis. Placenta , 28, 841-5. PMID: 17350092 DOI.
- ↑ Lorenzi T, Turi A, Lorenzi M, Paolinelli F, Mancioli F, La Sala L, Morroni M, Ciarmela P, Mantovani A, Tranquilli AL, Castellucci M & Marzioni D. (2012). Placental expression of CD100, CD72 and CD45 is dysregulated in human miscarriage. PLoS ONE , 7, e35232. PMID: 22606231 DOI.
- ↑ <pubmed>11178630</pubmed>
- ↑ Jessop FA, Lees CC, Pathak S, Hook CE & Sebire NJ. (2014). Umbilical cord coiling: clinical outcomes in an unselected population and systematic review. Virchows Arch. , 464, 105-12. PMID: 24259031 DOI.
- ↑ de Laat MW, Franx A, van Alderen ED, Nikkels PG & Visser GH. (2005). The umbilical coiling index, a review of the literature. J. Matern. Fetal. Neonatal. Med. , 17, 93-100. PMID: 16076615 DOI.
- ↑ Shwarzman P, Waintraub AY, Frieger M, Bashiri A, Mazor M & Hershkovitz R. (2013). Third-trimester abnormal uterine artery Doppler findings are associated with adverse pregnancy outcomes. J Ultrasound Med , 32, 2107-13. PMID: 24277892 DOI.
- ↑ Hill LM, Mills A, Peterson C & Boyles D. (1994). Persistent right umbilical vein: sonographic detection and subsequent neonatal outcome. Obstet Gynecol , 84, 923-5. PMID: 7970470
- ↑ Krzyżanowski A, Swatowski D, Gęca T, Kwiatek M, Stupak A, Woźniak S & Kwaśniewska A. (2019). Prenatal diagnosis of persistent right umbilical vein - Incidence and clinical impact. A prospective study. Aust N Z J Obstet Gynaecol , 59, 77-81. PMID: 29498037 DOI.
- ↑ Weichert J, Hartge D, Germer U, Axt-Fliedner R & Gembruch U. (2011). Persistent right umbilical vein: a prenatal condition worth mentioning?. Ultrasound Obstet Gynecol , 37, 543-8. PMID: 20922781 DOI.
- ↑ Lide B, Lindsley W, Foster MJ, Hale R & Haeri S. (2016). Intrahepatic Persistent Right Umbilical Vein and Associated Outcomes: A Systematic Review of the Literature. J Ultrasound Med , 35, 1-5. PMID: 26635256 DOI.
- ↑ Hallak M, Pryde PG, Qureshi F, Johnson MP, Jacques SM & Evans MI. (1994). Constriction of the umbilical cord leading to fetal death. A report of three cases. J Reprod Med , 39, 561-5. PMID: 7966052
- ↑ 14.0 14.1 Lee SW, Kim MY, Kim JE, Chung JH, Lee HJ & Yoon JY. (2014). Clinical characteristics and outcomes of antenatal fetal intra-abdominal umbilical vein varix detection. Obstet Gynecol Sci , 57, 181-6. PMID: 24883288 DOI.
- ↑ Cassidy-Vu L, Clark S & Cuka N. (2019). Extra-abdominal umbilical vein varix in a newborn. BMJ Case Rep , 12, . PMID: 31061189 DOI.
Reviews
Krzyżanowski A, Swatowski D, Gęca T, Kwiatek M, Stupak A, Woźniak S & Kwaśniewska A. (2019). Prenatal diagnosis of persistent right umbilical vein - Incidence and clinical impact. A prospective study. Aust N Z J Obstet Gynaecol , 59, 77-81. PMID: 29498037 DOI.
Articles
Search PubMed
May 2010 search "Placental Cord Development]" All (650) Review (91) Free Full Text (119)
Search Pubmed: Placental Cord | Umbilical Cord | Placental Cord Development | Umbilical Cord Development | Hofbauer cells
Additional Images
see all online Placental materials
Historic
| Historic Disclaimer - information about historic embryology pages
|
| Pages where the terms "Historic" (textbooks, papers, people, recommendations) appear on this site, and sections within pages where this disclaimer appears, indicate that the content and scientific understanding are specific to the time of publication. This means that while some scientific descriptions are still accurate, the terminology and interpretation of the developmental mechanisms reflect the understanding at the time of original publication and those of the preceding periods, these terms, interpretations and recommendations may not reflect our current scientific understanding. (More? Embryology History | Historic Embryology Papers)
|
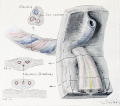
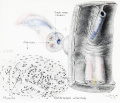
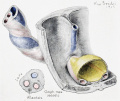
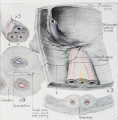
Cullen TS. Embryology, anatomy, and diseases of the umbilicus together with diseases of the urachus. (1916) W. B. Saunders Company, Philadelphia And London. Chapter I. Embryology of the Umbilical Region
- Cross-section of the Cord
Fig. 32 Term Fetus Cord and Placenta
Fig. 33 Term Fetus Umbilical Region
Fetal circulation overview
| Placenta Terms (expand to view)
|
- after-birth - term used to describe the delivery of placenta and placental membranes following birth of the child.
- allantois - An extraembryonic membrane, endoderm in origin extension from the early hindgut, then cloaca into the connecting stalk of placental animals, connected to the superior end of developing bladder. In reptiles and birds, acts as a reservoir for wastes and mediates gas exchange. In mammals is associated/incorporated with connecting stalk/placental cord fetal-maternal interface.
- amniocentesis - Clinical term for a prenatal diagnostic test where an ultrasound guided needle is used to extract a sample of the amniotic fluid. Amniocentesis
- anastomosis - Term used to describe the connection between two tubes. Applied to describe the connection between peripheral blood vessels without an intervening capillary bed.
- anchoring villi - (stem villi) describes the placental villi (embryonic) that attach to the decidua (maternal) tissue. The tip of the villi consists of a column of trophoblast cells attached to an epithelial plaque.
- angioblasts form clusters or blood islands on surface of yolk sac.
- angiogenesis - Term describing the development of new vessels from already existing vessels, this process is secondary to vasculogenesis which is the initial formation of first blood vessels by differentiation of pluripotent mesenchymal cells (extraembryonic mesoderm).
- capsularis - portion of maternal decidua that covers the conceptus facing towards the uterine cavity.
- cerebroplacental ratio - (CPR) a doppler ultrasound measurement calculated as the simple ratio between the middle cerebral artery pulsatility index (MCA‐PI) and the umbilical artery pulsatility index (UA‐PI). Fetuses with an abnormal ratio are thought to be a predictor of adverse pregnancy outcome.
- chorioamnionitis - (CA) An intraamniotic puerperal infection described as having 3 forms: histologic, clinical (clinical chorioamnionitis, IAI), and subclinical. Intraamniotic infection is a common (2-4%) event in labor and the systemic inflammatory response can also lead to preterm birth and neonatal complications.
- chorion - The extraembryonic membrane generated from trophoblast and extraembryonic mesoderm that forms placenta. chorion and amnion are made by the somatopleure. The chorion becomes incorporated into placental development. The avian and reptilian chorion lies beside the egg shell and allows gas exchange.
- chorionic cavity - The fluid-filled extraembryonic coelom (cavity) formed initially from trophoblast and extraembryonic mesoderm that forms placenta. chorion and amnion are made by the somatopleure. The chorion becomes incorporated into placental development. The avian and reptilian chorion lies beside the egg shell and allows gas exchange. In humans, this cavity is lost during week 8 when the amniotic cavity expands and fuses with the chorion.
- chorion frondosum - (frondosum = leafy) The chorion found on conceptus oriented towards maternal blood supply where the majority of villi form and proliferate, will contribute the fetal component of the future placenta.
- chorion laeve - (laeve = smooth) The smooth chorion found on conceptus away from maternal blood supply (towards uterine epithelium and cavity) with very few villi present.
- chorionic somatomammotropin - (CSH, human lactogen) A hormone synthesized within the placenta by syncytiotrophoblast cells. This protein hormone (190 amino acid) has a structure is similar to pituitary growth hormone.
- chorionic villus sampling - (CVS) The taking a biopsy of the placenta, usually at the end of the second month of pregnancy, to test the fetus for genetic abnormalities.
- coelocentesis - A sampling of extracoelomic fluid usually for an early prenatal diagnostic technique.
- connecting stalk - the original extra-embryonic mesoderm structure attaching the embryonic disc to the chorion. The placental blood vessels form within this structure.
- cord blood - (human umbilical cord blood, HUCB) A term used to describe blood collected from the placenta usually after birth. Has been identified as a source of stem cells with potential therapeutic uses and is stored in Cord Blood Banks throughout the world.
- cord knotting Term describing umbilical or placental cord knotting. This occurs in about 1% prevents the passage of placental blood, pseudoknots also occur usually with no effect.
- cord presentation - A term used to describe at birth the presence of the umbilical cord between the fetal presenting part and the cervix, with or without membrane rupture.
- cord prolapse - A term used to describe at birth the descent of the umbilical cord through the cervix alongside (occult) or past (overt) the presenting part in the presence of ruptured membranes (incidence of 0.1% to 0.6%).
- cotyledon - (Greek, kotyle = a deep cup) In the embryos of seed plants, the "seed leaves," in which nutrients are stored for use after germination. In placental animals, the term is also to describe the leaf-like structure of the placenta surface.
- cytotrophoblast - The "cellular" trophoblast layer surrounding (forming a "shell") the early implanting conceptus. Beginning at uterine adplantation, proliferation and fusion of these cells is thought to form a second outer trophoblast layer, the syncytiotrophoblast. The cytotrophoblast layer contributes to formation of the placental villi, the functional component of the fetal placenta.
- decidua basalis - The term given to the uterine endometrium at the site of implantation where signaling transforms the uterine stromal cells (fibroblast-like) into decidual cells. This forms the maternal component of the placenta, the decidualization process gradually spreads through the remainder of the uterus, forming the decidua parietalis.
- decidua basalis reaction - Term describing the maternal endometrial changes that occur initially at the site of, and following, blastocyst implantation. Seen as a deposition of glycogen, fibrin and proliferation of blood vessels. See also decidualization.
- decidua capsularis - The term given to the uterine endometrium which has been converted to decidua surrounding the conceptus on the smooth chorion side.
- decidua parietalis - The term given to the remainder of the uterine endometrium, away from the site of implantation, that gradually becomes comverted to decidua.
- decidual cell - The uterine stromal cells (fibroblast-like) that differentiate in response to both steroid hormones (progesterone) and embryonic signals. These cells then alter uterine environment to support further embryonic development as well as producing cytokines related to prolactin (PRL) and have an innate immune function.
- decidual reaction - maternal endometrial reaction invoked in order to block the rapid extension of the implanting syncytium.
- decidualization - (decidualisation, decidual reaction) The process by which uterine stromal cells differentiate in response to both steroid hormones and embryonic signals into large epitheliod decidual cells. This process is essential for the progress of implantation and establishing fetal-maternal communication.
- DHEA - (dehydroepiandrosterone, androstenolone) precursor of sex steroid hormones and is converted to testosterone and estradiol. Postnatally, an abundant circulating steroid produced in the adrenal gland. The fetal adrenal cortex produces dehydroepiandrosterone sulfate (DHEA-S) used by the placenta to produce estrogens. DHEA, androstenedione, and testosterone can be metabolized to epiandrosterone, and etiocholanolone. PMID 15635500
- fetal drug addiction - occurs when drugs used maternally cross the placental barrier and can establish neural/physiological addiction in the unborn fetus. drugs
- fetal erythroblastosis - (Haemolytic Disease of the Newborn) A clinical term describing an immune response between fetal and maternal blood groups; from fetus Rh+ / maternal Rh-. The leakage of blood from fetus, particularly at birth, causes maternal anti-Rh antibodies, which is then dangerous for a 2nd or future pregnancies.
- fetal intra-abdominal umbilical vein varix - (FIUV, umbilical vein varix) focal dilatation of the umbilical venous diameter at the level of cord insertion, the dilatation diameter increases linearly with gestational age. Represent about 4% of umbilical cord abnormalities
with an incidence of about 2.8 per 1,000 pregnancies, there is also a rarer form of extra-abdominal varices.PMID 24883288
- fibrinoid layer - (Nitabuch's layer) A layer formed at maternal/fetal interface during placentation and is thought to act to prevent excessively deep conceptus implantation. Fibrin-type fibrinoid (maternal blood-clot product) and matrix-type fibrinoid (secreted by invasive extravillous trophoblast cells).
- floating chorionic villi - Term used to describe the placental microanatomy structure of chorionic villi that are not attached to the maternal decidua and float in the maternal blood-filled space (lacunae). Structurally the same as anchoring chorionic villi conceptus side that are attached to the maternal decidua.These villi go through the same stages of development: primary villi - secondary villi - tertiary villi
- hemotrophic nutrition - Term used to describe in late placenta development the transfer of blood-borne nutrition from maternal to embryo/fetuscompared to early histiotrophic nutrition.
- heterotopic pregnancy - (Greek, heteros = other) Clinical term for a very rare pregnancy of two or more embryos, consisting of both a uterine cavity embryo implantation and an ectopic implantation.
- histiotrophic nutrition - Term used to describe in early placenta development the intital transfer of nutrition from maternal to embryo (histiotrophic nutrition) compared to later blood-borne nutrition (hemotrophic nutrition). Histotroph is the nutritional material accumulated in spaces between the maternal and fetal tissues, derived from the maternal endometrium and the uterine glands. This nutritional material is absorbed by phagocytosis initially by blastocyst trophectoderm and then by trophoblast of the placenta. in later placental development nutrition is by the exchange of blood-borne materials between the maternal and fetal circulations, hemotrophic nutrition.
- Hofbauer cells - Cells found within placental villi connective tissue. Have a role as macrophages of mesenchymal origin with potentially additional functions (remodeling, vasculogenesis, regulation of stromal water content).
- Human chorionic corticotropin - (hCACTH) placental derived hormone equivilant to corticotropin (ACTH) from the pituitary.
- Human chorionic gonadotrophin - (hCG) like leutenizing hormone, supports corpus luteum, originally secreted by trophoblast cells.
- Human chorionic somatommotropin - (hCS, placental lactogen) hormone level increases in maternal blood through pregnancy, decreases maternal insulin sensitivity (raising maternal blood glucose levels and decreasing maternal glucose utilization) aiding fetal nutrition.
- Template:Hydatiform mole - A uterine tumour with "grape-like" placenta appearance without enclosed embryo formation, arises mainly from a haploid sperm fertilizing an egg without a female pronucleus. It is one form of gestational trophoblastic disease(GTD), a number of abnormalities including hydatiform mole, invasive mole, choriocarcinoma and placental site trophoblastic tumor (PSTT).
- hysterectomy – clinical term for the surgical removal of the uterus.
- Langhans layer - cytotrophoblast cell layer.
- maternal antibodies - antibodies from the mother's immune system that are capable of crossing placental barrier. They can provide immune protection to the embryo, but may also participate in immune disease (fetal erythroblastosis).
- maternal sinusoids - placental spaces around chorionic villi that are filled with maternal blood. This is the closest maternal/fetal exchange site.
- Nitabuch's layer - (fibrinoid layer) The layer formed at maternal/fetal interface during placentation and is thought to act to prevent excessively deep conceptus implantation. Fibrin-type fibrinoid (maternal blood-clot product) and matrix-type fibrinoid (secreted by invasive extravillous trophoblast cells).
- Morbidly adherent placenta (MAP) A general clinical term used to describe the different forms of abnormal placental implantation (Accreta, Increta and Percreta).
- oligohydramnios - Clinical term for the accumulation a deficiency of amniotic fluid during pregnancy. See also polyhydramnios, an excess of amniotic fluid.
- persistent right umbilical vein - (PRUV) A placental cord abnormality associated with fetal abnormalities and poor neonatal prognosis. The estimated incidence of persistent right umbilical vein in a low-risk population is 1 : 526. PMID 12047534
- polyhydramnios - Clinical term for the accumulation of excess amniotic fluid during pregnancy. See also oligohydramnios, a deficiency of amniotic fluid.
- placenta - (Greek, plakuos = flat cake) The developmental organ formed from maternal and fetal contributions in animals with placental development. In human, the placenta at term is a discoid shape "flat cake" shape; 20 cm diameter, 3 cm thick and weighs 500-600 gm. Placenta are classified by the number of layers between maternal and fetal blood (Haemochorial, Endotheliochorial and Epitheliochorial) and shape (Discoid, Zonary, Cotyledenary and Diffuse). The placenta has many different functions including metabolism, transport and endocrine.
- placenta accreta - The abnormal placental adherence, either in whole or in part of the placenta with absence of decidua basalis, leading to retention as an after-birth to the underlying uterine wall. The incidence of placenta accreta also significantly increases in women with previous cesarean section compared to those without a prior surgical delivery.
- placental arteries - (umbilical arteries) In placental animals, the blood vessels which develop within the placental cord carrying relatively deoxygenated blood from the embryo/fetus to the placenta. In humans, there are two placental arteries continuous with the paired internal iliac arteries (hypogastric arteries) arising off the dorsal aortas. At birth this vessel regresses and form the remnant medial umbilical ligament.
- placental cord - (umbilical cord) The placental cord is the structure connecting the embryo/fetus to the placenta. It is initially extra-embryonic mesoderm forming the connecting stalk within which the placental blood vessels (arteries and veins) form. In human placental cords the placental blood vessels are initially paired, later in development only a single placental vein remains with a pair of placental arteries. This structure also contains the allantois, an extension from the hindgut cloaca then urogenital sinus. Blood collected from the placental cord following delivery is a source of cord blood stem cells.)
- placental diameter - is measured in the transverse section by calculating the maximum dimensions of the chorionic surface.
- placental growth factor - (PlGF) A growth factor of the vascular endothelial growth factor (VEGF) family, released from the placental trophoblast cells and other sources that stimulates blood vessel growth.
- placental malaria - The malarial infection of the placenta by sequestration of the infected red blood cells. This condition can be common in regions where malaria is endemic with women carrying their first pregnancy (primigravida).
- placenta membranacea - rare placental abnormality characterized by the presence of chorionic villi directly attached to and covering the fetal membranes. Placenta Membranacea
- placenta previa - placenta overlies internal os of uterus, abnormal bleeding, may require cesarian delivery.
- placental thickness - is measured at its mid-portion from the chorionic plate to the basilar plate, on a longitudinal plane (less than 4 cm at term). Excludes any abnormalities (fibroids, myometrial contractions, or venous lakes). The placental thickness approximates in millimeters to the weeks of gestation.
- placental vein - (umbilical vein) In placental animals, the blood vessels which develop within the placental cord carrying relatively oxygenated blood from the placenta to the embryo/fetus. In humans, there are initially two placental veins which fuse to form a single vein. The resence of paired veins in the placental cord can be indicative of developmental abnormalities.
- placentophagia - Term used to descrbe the maternal ingestion of afterbirth materials (placental membranes and amniotic fluid) that can occur following mammalian parturition (birth).
- primary villi - (primary chorionic villi) Term describing the earliest stage of embryonic placenta development. In humans, the conceptus during week 2 this first stage of chorionic villi development consists of only the trophoblastic shell cells (syncitiotrophoblasts and cytotrophoblasts) forming finger-like extensions into maternal decidua. Initially these finger-like projections cover the entire surface of chorionic sac and later become restricted to the placental surface. The villi stages are ongoing as the placenta continues to grow through both the embryonic and fetal development.
- pre-eclampsia - During pregnancy a combination of high blood pressure, protein in urine and fluid retention resulting in maternal sudden excessive swelling of the face, hands and feet. Eclampsia is the subsequent development of convulsions, kidney failure, liver failure, clotting problems or mortality.
- Rh alloimmunization - feto-maternal haemorrhage generally in late pregnancy results in an Rh-negative woman becoming sensitised to Rh-positive fetal cells that enter her circulation. Clinically treated with anti-D immune globulin prophylaxis, alloimmunization occurs in 9–10% of at-risk pregnancies. immune
- secondary villi - (secondary chorionic villi) Term describing the second stage of embryonic placenta development. In humans, the conceptus during week 3 onward this stage of chorionic villi development consists of the trophoblastic shell cells (syncytiotrophoblast and cytotrophoblasts) filled with extraembryonic mesoderm forming finger-like extensions into maternal decidua. Initially these finger-like projections cover the entire surface of chorionic sac and later become restricted to the placental surface. The villi stages are ongoing as the placenta continues to grow through both the embryonic and fetal development. Placental villi stages: primary villi - secondary villi - tertiary villi
- syncytiotrophoblast - A multinucleated cell currently thought to form by the fusion of another trophoblast cell the cytotrophoblasts, within the trophoblast layer (shell) of the implanting conceptus. In early development, these cells mediate implantation of the conceptus into the uterine wall and secrete the hormone (Template:Human Chorionic Gonadotrophin, hCG) responsible for feedback maintainance of the corpus luteum (in maternal ovary) and therefore maintaining early pregnancy.
- trophoblast - (trophectoderm, Greek, trophe = "nutrition" and blast = a primordial cell) cells that firstly support adplantation, implantation and endocrine support of pregnancy. Contribute to the extraembryonic tissues, fetal placenta and membranes. Initially form 2 populations individual cytotrophoblast cells and their fused multinucleate syncytiotrophoblast cells.
- Twin-twin transfusion syndrome - (TTTS) in monozygotic twins with monochorionic and diamniotic placenta, with intrauterine blood transfusion from one twin (donor) to another twin (recipient) where there is an imbalance of blood flow from the donor twin to the recipient twin. Clinically diagnosed by the alternate presence of polyhydramnios in one fetus and oligohydramnios in the co-twin, occurs in about 10% of monochorionic twins.
- umbilical cord (placental cord) fetal attachment cord 1-2 cm diameter, 30-90cm long, covered with amniotic attached to chorionic plate, umbilical vessels (artery, vein) branch into chorionic vessels. Vessels anastomose within the placenta.
- umbilical vein varix - (fetal intra-abdominal umbilical vein varix, FIUV) focal dilatation of the umbilical venous diameter at the level of cord insertion, the dilatation diameter increases linearly with gestational age. Represent about 4% of umbilical cord abnormalities
with an incidence of about 2.8 per 1,000 pregnancies, there is also a rarer form of extra-abdominal varices. PMID 24883288
- vasculogenesis - formation of first blood vessels by differentiation of pluripotent mesenchymal cells (extraembryonic mesoderm) followed by angiogenesis which is the development of new vessels from already existing vessels.
- vasculosyncytial membranes - localised areas of the placental villous membrane where the barrier thickness separating maternal and fetal circulations is reduced to as little as 1-2 microns. PMID 1287078
- villi - Plural of villus, which is a thin projection from a surface. The term in development is used to describe the individual functional units together of the fetal placenta.
- virus - small infectious agents that may cross the placental barrier. Can infect embryo and/or placenta and cause developmental abnormalities. (e.g. cytomegalovirus, rubella, measles).
- Wharton's jelly - placental cord (umbilical cord) gelatinous connective tissue composed of myofibroblast-like stromal cells, collagen fibers, and proteoglycans. Increases in volume (myxomatous, connective tissue embedded in mucus) at parturition (birth) to assist closure of placental blood vessels. Matrix cells from Wharton's jelly have recently been identified as a potential source of mesenchymal stem cells (MSC), also called mesenchymal stromal cell. This placental cord substance is named after Thomas Wharton (1614-1673) an English physician and anatomist who first described this placental tissue.
|
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, June 15) Embryology Placenta - Cord. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Placenta_-_Cord
- What Links Here?
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G