Paper - The Formation of the Pars Membranacea Septi (1916)
| Embryology - 30 Apr 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Frazer JE. The formation of the pars membranacea septi. (1916) J Anat. 51(1): 19-29. PMID 17103800
| Historic Disclaimer - information about historic embryology pages |
|---|
 |
The Formation of the Pars Membranacea Septi
{kind=link}
By J. Ernest Frazer, F.R.C.S., St Mary’s Hospital, Professor of Anatomy in the University of London. (1916)
Introduction
The pars membranacea is not only the thinnest portion of the interventricular septum, but is also in part of its extent a structure separating the right auricle from the cavity of the aortic vestibule; it cannot therefore be considered as merely a part of a structural system, more or less simple, which divides the heart into right and left sides, for the aortic vestibule is formed to the right of the plane of the interventricular septum, and is associated with the region of the earlier bulb.
Some little time ago it was suggested to me by Sir John Broadbent that a series of models showing the main points in cardiac development would be of value in demonstrating to clinical students the bearing of these points on certain lesions of the organ. I undertook to make such a series, and used the sections of embryos of 5 mm. and upwards which I possess, in the work. Many of the models were so cut up in endeavouring to follow the development as exemplified in them that they were useless for subsequent demonstration : this, however, caused me little regret, for I had determined at an early stage that the purpose with which the work had been undertaken would be served best by constructing “schematic” models — made with a free hand, founded on the actual reconstructions, but only showing the general and main conditions, so that they would bear to the real models the same relation that a scheme or diagram on paper bears to the structure or conception of which it is used as an illustration of some particular aspect or condition. Anyone who has worked with reconstruction models of the heart will agree, I think, that they are very difficult to read, after the earlier stages, owing to the rapidly growing complexity of detail and inability to see more than a small part of each cavity at once, and such models would certainly be quite useless for the purpose of teaching students.
The subject of the present paper presented itself as an important one early in the work, because it seemed that clear-cut ideas on the formation of the region were necessary for a proper understanding of development in the immediate neighbourhood. Three of the schematic models illustrate this subject, and I propose to utilise the plan of their construction in the description; they represent the bulbar and ventricular parts as simple smooth—walled cavities, opened and exposed by the removal of the ventral Wall, so that the continuous cavity, necessarily flatter than is actually the case, is seen from the atrial opening to the arterial extremity where the aortic stem begins.
A diagrammatic rendering of the state of things found at a relatively early stage is seen in fig. 1. The cavity of the bulb is still easily distinguished, being partly separated from that of the ventricle by the bulbo-ventricular ridge, elongated and spur-like on section; owing to the presence of this ridge, the cavities of bulb and ventricle become continuous to the right of the position occupied by the auriculo-ventricular opening. The interventricular septum is very low, leaving a wide passage between the two ventricles, and the lower end of the septum reaches the right tubercle of the lower a.-V. endocardial cushion, while its upper end runs into the bulbo-ventricular spur, near its base. The arterial endocardial cushions are shown at the upper end of the bulb ; it must not be forgotten that these figures are only schemes, and that the cushions‘ in an embryo whose ventricular development would be at about the stage seen in the drawing, would be merely indefinite thickenings. These cushions are four in number, and the two that are placed laterally are represented as not yet joined, so that a single opening exists between the anterior and posterior cushions leading from the undivided bulbar cavity to the single aortic stem.

Fig. 1. Diagram showing the relations at an early stage between the auriculo-ventricular opening and ventricles, the cavity of the bulb, and the bulbo-ventricular ridge. The distal cushions of the bulb are shown in a more differentiated state than they really exhibit at this stage.
It is plain that no direct passage can be made between the left ventricle and the aortic end of the bulb so long as the ridge exists between the bulbar and ventricular cavities, and this ridge now commences to atrophy, or at any rate to disappear, as is well known. I think that the process is more than a passive one, as is perhaps usually taught, and that, although there may be merely a failure in growth at first, there is an actual degeneration coming into play very soon: such, at least, is the opinion I have formed from the examination of sections, and the assumption appears to be necessary to account for the practically complete disappearance of the ridge and wall in its neighbourhood. But, whatever may be the nature of the agency bringing it about, there is no doubt of the fact of the disappearance of the ridge, and, with this, new possibilities open up for further development of the bulbo—ventricular complex.
The stage of its formation on which the heart enters now is illustrated in fig. 2; here the cavity of the “bulb” no longer opens downwards into the ventricle to the right of the a.-v. orifice, but directly over its righthand portion. This new relationship is not attained by any special extension of the a.-v. opening towards the right: the opening has become wider with the increasing ventricular width, but that this growth is purely proportionate is evident when we look at the situation of the interventricular septum. It is, then, the disappearance of the intervening bulbo—ventricular ridge which allows the lower opening of the bulbar region of the cavity to present a wider lumen and to become continuous with the ventricle much more to the left than is possible in the earlier stages. The remains of the ridge are shown in the diagram as a low crest between the right end of the a.-v. opening and the posterior arterial cushion. The direction of the ridge, like the somewhat upturned extremity of the a.-v. opening, is perhaps to be referred to the combined effects of the growth of the right ventricle, and the disappearance of all but the basal portion of the ridge.
A change is seen in the arterial endocardial cushions, in that the two lateral cushions are now shown as fused across the centre of the lumen of this part of the bulb, thus dividing it into two openings, anterior and posterior. which are continuous in their turn with the two distinct arteries into which the arterial stem has been divided by the aortic septum. The aortic septum is not indicated in the figure: it would meet and become continuous with the upper aspect of the fused cushions if it were put in, so that the aorta would reach the posterior opening and the pulmonary artery the anterior one. The course which must be taken by the aortic blood from the left ventricle is indicated by the arrow: its channel must be still further hollowed by the complete disappearance of the bulboventricular ridge, and the fusion of the a.v. cushions will afford a continuous floor for it, separating it from the cavity of the right auricle and constituting therefore the upper part of the pars membranacea septi. In the meantime, other changes are taking place in this region, concerned with the closing in of the aortic channel and its separation from the corresponding aditus to the pulmonary artery. These are shown in the figure in the shape of two “ bulbar ” ridges: the left ridge is on the dorsal and left wall at its upper end and on the ventral and left wall below, while the right ridge is on the right wall, rather ventral in its upper part and decidedly more dorsal below, where it reaches the right side of the a.—v. opening. The ridges are continued above into the arterial cushions, which are fused, so that, when they meet, the ridges would form a roof to the aortic channel continuous with the spiral septum formed by the arterial cushions and the arterial septum above these.

Fig. 2. To illustrate the intermediate stages of the formation of the two channels and pars membranacea. R. B. R., L. B.R., right and left bulbar ridges. The arrow marks the situation and direction of the aortic channel.
The lower end of the left ridge is at first separated from the upper part of the interventricular septum by the remains of the bulbo-ventricular ridge, but as this disappears the two structures become continuous, the left ridge, however, reaching the right side of the septum, as might naturally be expected, seeing that it is developed in the bulbar region. These two ridges are, of course, the “proximal bulbar swellings” of Tandler’s description. It is, perhaps, hardly necessary to point out that they and the whole bulbar region have been shown in the diagram as more elongated, for the sake of clearness, than they appear in the actual condition. Also, for similar reasons, the original direction of the arterial end of the heart has been preserved; actually, the ventral and dextral growth of the right ventricle leads, with the atrophy of the dorsal and left wall of the bulbar region, to an increasing obliquity, dorsally and to the left, of the arterial portion of the heart, but these are all non—essential points in the description of the mode of formation of the pars membranacea, septi.
The essential matters are the apposition and junction of the upper and lower a.-v. cushions and the disappearance of the bulbo-ventricular ridge, so that the dorsal and left arterial cushions are brought very near to the right end of the a.-v. region. At the same time, or probably usually just before this, the aortic channel is separated from the pulmonary subdivision by the meeting of the bulbar ridges, the extension of the fused (lateral) arterial cushions, and the junction of this compound septum with that between the ventricles: it will perhaps be most convenient to deal shortly with this first—the septum between the right and left channels.
In fig. 3 the larger drawing represents the elements which enter into the composition of the septum between the two channels, in the way in which they are shown in the schematic model. The lower parts of the bulbar ridges meet, but they are separated above by the down-growth of the fused lateral arterial cushions : the right ridge grows across the auriculo—ventricular opening[1] to join with the other ridge, and shortly after this the lower free edge of the septum formed in this way fuses with the free margin of the interventricular septum, with which the left ridge is, as has been seen, already continuous. The smaller drawing is from a model of a heart from an embryo of 16 mm. length, showing only this region, dissected to exhibit the composition of the dividing septum: in this the proper obliquity of the parts is, of course, a factor in the appearance, the pulmonary orifice looking almost directly toward the observer, and the aorta, where it is cut, being far above the level of the aortic valves. It is evident that, when the division between right and left sides is completed in this way, there is no closure of the true interventricular foramen, for the structures concerned in the separation between the two channels reach the margin of the foramen and leave its lumen patent, affording passage to the blood from the left ventricle to the aortic channel.

Fig. 3. A. Diagram to illustrate the further growth of the bulbar ridges and arterial cushions to complete the division into two channels. B. View of the infundibular aspect of the dividing septum, from the “ dissected ” reconstruction model, 16 mm.
While this, then, is the Way in which the aortic channel is being cut off from the rest of the region, the floor is formed in the manner indicated or foreshadowed in fig. 2. The fused a.-v. cushions make the main part of the bed of the channel, the bulbo-ventricular ridge has completely disappeared, and consequently the region of the arterial cushions lies just above the right end of the fused a.-v. cushions. fig. 4- is from a reconstruction model (16 1nm.), and shows the position of the cushions. A is the upper a.-v. cushion, and B the lower one, larger and better marked than the other in the model. The interventricular septum is partly cut away, but its area of contact" with the lower cushion is indicated by interrupted lines: the same method is used to show the position of the right bulbar ridge, the base of which only is visible in the illustration. Evidently the right ridge, when it crosses the line of the right a.—v. opening, rests on the upper surface of the right tubercle of the lower cushion, the front part of which projects slightly below it (of. fig. 2). Thus it is along this cushion that the right ridge comes into relation with the interventricular septum.
The bed of the aortic channel is seen to be made from a part of the lower cushion and the whole thickness of the right portion of the upper cushion. The right tubercle of the upper cushion is marked :6, and just above this is seen the posterior arterial cushion. The proximity of the two structures is accounted for by the total disappearance of the bulboventricular ridge, and probably of the left dorsal wall immediately adjacent to it. The right tubercle, w, is thus left with only a very narrow strip of tissue between it and the posterior arterial cushion.

Fig. 4. The floor or dorsal wall of the aortic vestibule, from the 16 mm model, simplified. A, B, upper and lower auriculo-ventricular cushions : z, right tubercle of upper cushion ; r.a.v., right a.-v. opening; l.a.v., left. opening.
The model from which the last figure was drawn is one of two made from embryos of 13 and 16 mm. respectively, which were constructed with a View to showing the final position of the various parts described above. In these embryos junction of the several parts has occurred, but the lines of junction are still nearly altogether apparent. In the 16-mm. specimen the sections are particularly clear and good, and the model made from it gave the figures shown in figs./L and 3, B. The “ suture lines” were drawn and cut with the rest of the sections in which they occurred, with the result that, when the models were made, the component parts were shown very clearly. The 13-mm. embryo was treated in the same way, and the model cut up afterwards: although the sections of this specimen are very good, yet an excessive amount of blood in the heart made it necessary to refer continuously to the higher powers of the microscope to decide doubtful points in the drawings, wherefore a larger model was not made from it; but the results obtained were practically the same as in the other case—in some ways even more definite. In an embryo of 18 mm. the sections did not exhibit the original divisions of the parts with enough clearness to lead one to make a similar kind of model.
By adopting these means, actual confirmation became possible of the impressions gained from the earlier stages as to the mode of formation of the membranous part of the septum. It was seen that the upper cushion— perhaps in association with the smaller growth of this part of the ventricle, and even, it may be, the atrophy towards the right——-is much less extensive than the lower one, the size of which may possibly be connected with the greater growth of the lower parts of the ventricles. Moreover, it became evident that, to make a proper channel for the stream to the aorta, the ventricular surfaces of the cushions were rendered concave and hollowed in an oblique direction, the hollow (fig. 4«) affecting the lower cushion more toward the left and the upper one more toward the right. This part of the channel wall is separated, therefore, on the left of the middle line from the left auricle, and further on from the right auricle, by the endocardial cushions. It is only that part which comes into relation with the right auricle, i.e. the part made by the right end of the upper cushion, which forms a portion of the described pars membranacea; but this limitation is in all likelihood due to the conception of the pars membranacea as a portion of the dividing septum between right and left sides, whereas it would perhaps be more reasonable to look on the separating wall between auricular and ventricular region as being of the same value on each side, made from the same structures, and to describe both these areas as continuous, mla the lower cushion, with the proper interventricular septum.
When the a.-V. cushions fuse, the right and left openings remain as subvertical slits, bounded on their inner sides by the upper and lower tubercles of the corresponding cushions. When the right bulbar ridge grows across the right opening (fig. 4:) it cuts oil’ the upper part of this, and leaves the definite opening formed only from the lower portion of the vertical slit, that part which is bordered by the lower portion of the lower cushion. The upper part, beside the upper tubercle, closes and thus completes the bed of the channel, but the closure would appear to be subsequent to the formation of the roof of the channel: in the 13-mm. embryo a communication can still be followed between the channel and the auricle ; in the 16—mm. specimen the track is closed at its aortic end for the thickness of some sections, while in the embryo of 18 mm. no indication of its former position could be recognised with any certainty. I could not be certain whether the upper part of the left opening persisted or not.
It is advisable, perhaps, to call attention again to the fact that not only are the figures illustrating the earlier modes of formation purely schematic but even the figures drawn from the actual model have had to be simplified to some extent to make them of use for the purposes of this paper—for the intricacies which make the models so hard to read when one can turn them about in the hand would render the drawings of their actual state quite unintelligible, in all probability, to the reader who has no opportunity of handling them. It might not be considered out of place, therefore, if a little consideration were given to some of the points which are not illustrated by the diagrams.
To take, for example, the two, bulbar ridges. As has been already pointed out, these are not so long as they are represented in the diagrams, and they are, moreover, much thicker, so that their lower ends form, where they meet, a thick but low mass projecting somewhat into the cavity of the right ventricle (fig. 4-). Thus a relatively thick septum exists between the two channels. The upper parts of the ridges are separated by the down-growth of the fused (lateral) arterial cushions, which makes a mass of remarkable thickness: the prolongation downwards of the cushion-mass is in the form of a double tongue, each tongue fitting it between the pulmonary or aortic surface, as the case may be, of the ridges. Thus, in fig. 4, B, the tongue seen foreshortened between the upper parts of the ridges is only one of the down-growths, for a corresponding formation lies between the ridges on their deep or aortic aspect, and the two tongues are separated for some distance by a cleft passing upwards between them, filled by the basal portions of the ridges. Moreover, the axis of each tongue passes in a different direction; that of the deep down-growth, compared with that of the other, is directed markedly to the left. Thus the whole mass exhibits a twist in conformity with the general spiral seen in the structures which separate the aortic and pulmonary vessels and channels.
In the diagrams the interventricular septum is shown reaching the lower a.-v. cushion, close to the right tubercle, but I do not think it would be correct to look on the solid septum proper as actually reaching the cushion. It seems to reach its lower edge and, above this, only to be connected with it by loose trabecular structure, through which a partly interrupted passage can be traced between the ventricles. Even when the Whole system is closing in, this arrangement seems to hold, and here, then, the septum is formed presumably by the aggregation of looser trabeculae, and perhaps by part of the cushion above this. The addition of loose trabecular tissue to the septum would also appear to take place on its surface, particularly on the left side: the 13—mm. model shows such tissue, seemingly pushed against this surface of the septum by the pressure of the blood—stream passing to the aortic channel, and probably the thick septum seen in later stages owes some of its size to the addition of this trabecular structure to its surfaces as the ventricular cavities get more defined and the channels opened out.
It has also been pointed out that the arterial stem is really directed more obliquely than shown in the drawings. This is due to the degeneration and disappearance of the left and dorsal wall of the bulbar region. As a. result this part of its wall necessarily shortens, and in fact its wall in this part practically disappears except in its distal portion, where the cushions lie which form the semilunar valves: in this way these (dorsal and left) valves come to lie just above the pars membranacea. But the atrophy does not affect the front and right walls of the bulb, so that in this part more of the original cavity of the bulb might be expected to persist; but whether the wall of this part is invaded by the ventricular musculature or is’ pushed up by it as it grows seems a difficult question to answer satisfactorily. It is sufficient for present purposes to recognise that the disappearance of the bulb-wall is most marked dorsally and on the left, in the region of the left channel, with resulting obliquity of the part: the floor of the aortic channel becomes very short, the septum between the two channels is longer, and the front wall of the infundibulum longer still.
Summing up shortly the results which I have endeavoured to set forth in the preceding pages, it may be said that the pars membranacea is made from the fused a.-V. cushions, the auriculo-vestibular part from the right end of the upper cushion, the interventricular part from the lower one with some trabecular structure joining this with the proper interventricular septum. The disappearance of the bulbo-ventricular ridge is a necessary preliminary to the formation of the aortic vestibule, and is also the cause of the shortness of the dorsal wall or floor of the vestibule, and the proximity of the pars membranacea and the dorsal and left aortic valves. The true interventricular foramen does not close, but remains patent as the opening into the aortic vestibule from the left ventricle. The septum separating the cavities of the aortic vestibule and the infundibulum is made by the junction of two bulbar ridges, which join the free edge of the interventricular foramen below, and are separated above by a marked down-growth of the fused lateral endocardial cushions of the arterial end of the bulb. Only the lower portion of the right auriculo-ventricular opening remains as the permanent right opening, the upper part being closed and lying in the floor of the aortic vestibule: this upper moiety is cut off from the lower by the growth of the right bulbar ridge across the opening to meet the margin of the interventricular septum. It is doubtful Whether the permanent left opening is the Whole or only a part of the earlier one.
- ↑ This existence of a new transversely directed upper limit to the right a.-v. opening may afford an explanation of the presence of three cusps in the valve of this side, contrasting with the simpler original form of the left opening : this, however, is only a suggestion, in conformity with the disposition of the cusps on each side, for I have not investigated the matter further.
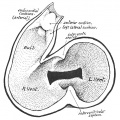
Fig. 1. Diagram showing the relations at an early heart stage
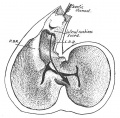
Fig. 2. Intermediate stages of the formation of the two channels and pars membranacea
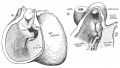
Fig. 3. Growth of the bulbar ridges and arterial cushions
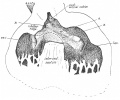
Fig. 4. The floor or dorsal wall of the aortic vestibule from the 16 mm model
Cite this page: Hill, M.A. (2024, April 30) Embryology Paper - The Formation of the Pars Membranacea Septi (1916). Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Paper_-_The_Formation_of_the_Pars_Membranacea_Septi_(1916)
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G