Uterus Development: Difference between revisions
mNo edit summary |
mNo edit summary |
||
| Line 20: | Line 20: | ||
|-bgcolor="F5FAFF" | |-bgcolor="F5FAFF" | ||
| | | | ||
* '''Review - The cell biology and molecular genetics of Müllerian duct development''' | * '''Review - The cell biology and molecular genetics of Müllerian duct development'''{{#pmid:29350886|PMID29350886}} "The Müllerian ducts are part of the embryonic urogenital system. They give rise to mature structures that serve a critical function in the transport and development of the oocyte and/or embryo. In most vertebrates, both sexes initially develop Müllerian ducts during embryogenesis, but they regress in males under the influence of testis-derived Anti-Müllerian Hormone (AMH)." | ||
* ''' | * '''Outcome of assisted reproduction in women with congenital uterine anomalies: a prospective observational study'''{{#pmid:29055072|PMID29055072}} "Consecutive women referred for subfertility between May 2009 and November 2015 who underwent assisted reproduction were included in the study. As part of the initial assessment, each woman underwent three-dimensional transvaginal sonography. Uterine morphology was classified using the modified American Fertility Society (AFS) classification of congenital uterine anomalies proposed by Salim et al. ...Congenital uterine anomalies as a whole, when defined using the modified AFS classification, do not affect clinical pregnancy or live-birth rates in women following assisted reproduction, but do increase the incidence of preterm birth. The presence of uterine abnormalities more severe than arcuate uterus significantly worsens all pregnancy outcomes." | ||
* ''' | * '''WNT4 coordinates directional cell migration and extension of the Müllerian duct essential for ontogenesis of the female reproductive tract'''{{#pmid:26721931|PMID26721931}} "The Müllerian duct (MD) is the anlage of the oviduct, uterus and upper part of the vagina, the main parts of the female reproductive tract. Several wingless-type mouse mammary tumor virus (MMTV) integration site family member (Wnt) genes, including Wnt4, Wnt5a and Wnt7a, are involved in the development of MD and its derivatives, with Wnt4 particularly critical, since the MD fails to develop in its absence. We use, here, Wnt4(EGFPCre)-based fate mapping to demonstrate that the MD tip cells and the subsequent MD cells are derived from Wnt4+ lineage cells. Moreover, Wnt4 is required for the initiation of MD-forming cell migration." [[Developmental_Signals_-_Wnt#WNT4|WNT4]] | ||
* '''The origin of the Mullerian duct in chick and mouse''' | * '''LHX1 is required in Müllerian duct epithelium for uterine development'''{{#pmid:24560999|PMID24560999}} "The female reproductive tract organs of mammals, including the oviducts, uterus, cervix and upper vagina, are derived from the Müllerian ducts, a pair of epithelial tubes that form within the mesonephroi. The Müllerian ducts form in a rostral to caudal manner, guided by and dependent on the Wolffian ducts that have already formed. Experimental embryological studies indicate that caudal elongation of the Müllerian duct towards the urogenital sinus occurs in part by proliferation at the ductal tip. The molecular mechanisms that regulate the elongation of the Müllerian duct are currently unclear. Lhx1 encodes a LIM-homeodomain transcription factor that is essential for male and female reproductive tract development. Lhx1 is expressed in both the Wolffian and Müllerian ducts. Wolffian duct-specific knockout of Lhx1 results in degeneration of the Wolffian duct and consequently the non-cell-autonomous loss of the Müllerian duct. To determine the role of Lhx1 specifically in the Müllerian duct epithelium, we performed a Müllerian duct-specific knockout study using Wnt7a-Cre mice. Loss of Lhx1 in the Müllerian duct epithelium led to a block in Müllerian duct elongation and uterine hypoplasia characterized by loss of the entire endometrium (luminal and glandular epithelium and stroma) and inner circular but not the outer longitudinal muscle layer. Time-lapse imaging and molecular analyses indicate that Lhx1 acts cell autonomously to maintain ductal progenitor cells for Müllerian duct elongation. These studies identify LHX1 as the first transcription factor that is essential in the Müllerian duct epithelial progenitor cells for female reproductive tract development." [https://www.genenames.org/cgi-bin/gene_symbol_report?hgnc_id=HGNC:6593 HGNC] | ||
* '''Essential roles of mesenchyme-derived beta-catenin in mouse Mullerian duct morphogenesis''' | |||
* '''The origin of the Mullerian duct in chick and mouse'''{{#pmid:17070514|PMID17070514}} "In vertebrates the female reproductive tracts derive from a pair of tubular structures called Mullerian ducts, which are composed of three elements: a canalised epithelial tube, mesenchymal cells surrounding the tube and, most externally, coelomic epithelial cells. ... We show that all Mullerian duct components derive from the coelomic epithelium in both species. Our data support a model of a Mullerian epithelial tube derived from an epithelial anlage at the mesonephros anterior end, which then segregates from the epithelium and extends caudal of its own accord, via a process involving rapid cell proliferation. This tube is surrounded by mesenchymal cells derived from local delamination of coelomic epithelium." | |||
* '''Essential roles of mesenchyme-derived beta-catenin in mouse Mullerian duct morphogenesis'''{{#pmid:17532316|PMID17532316}} | |||
|} | |} | ||
{| class="wikitable mw-collapsible mw-collapsed" | {| class="wikitable mw-collapsible mw-collapsed" | ||
| Line 41: | Line 43: | ||
The Müllerian duct (= paramesonephric duct, preferred terminology) paired ducts that form the epithelial lining of female reproductive organs: utererine tube, uterus, upper vaginal canal. The term "paramesonephric" duct means beside the mesonephric (Wolffian) duct, which is its anatomical location in early development. Mullerian refers to Johannes Peter Müller (1801-1858) a German scientist who specialised in comparative anatomy. These ducts initially form and then degenerate in the male. | The Müllerian duct (= paramesonephric duct, preferred terminology) paired ducts that form the epithelial lining of female reproductive organs: utererine tube, uterus, upper vaginal canal. The term "paramesonephric" duct means beside the mesonephric (Wolffian) duct, which is its anatomical location in early development. Mullerian refers to Johannes Peter Müller (1801-1858) a German scientist who specialised in comparative anatomy. These ducts initially form and then degenerate in the male. | ||
A recent study using both chicken and mouse embryos has shown that these initially paired tubular structures derive from the coelomic epithelium. | A recent study using both chicken and mouse embryos has shown that these initially paired tubular structures derive from the coelomic epithelium.{{#pmid:17070514|PMID17070514}} | ||
:"Müllerian epithelial tube derived from an epithelial anlage at the mesonephros anterior end, which then segregates from the epithelium and extends caudal of its own accord, via a process involving rapid cell proliferation. This tube is surrounded by mesenchymal cells derived from local delamination of coelomic epithelium." | :"Müllerian epithelial tube derived from an epithelial anlage at the mesonephros anterior end, which then segregates from the epithelium and extends caudal of its own accord, via a process involving rapid cell proliferation. This tube is surrounded by mesenchymal cells derived from local delamination of coelomic epithelium." | ||
| Line 57: | Line 59: | ||
===Initiation=== | ===Initiation=== | ||
Coelomic epithelium Lim1 expressing cells are specified to a duct fate. | Coelomic epithelium Lim1 expressing cells are specified to a duct fate.{{#pmid:14695376|PMID14695376}} | ||
* Lim - proteins named for 'LIN11, ISL1, and MEC3,' are defined by the possession of a highly conserved double zinc finger motif called the LIM domain. | * Lim - proteins named for 'LIN11, ISL1, and MEC3,' are defined by the possession of a highly conserved double zinc finger motif called the LIM domain. | ||
| Line 106: | Line 108: | ||
|} | |} | ||
The data below gives an overview of the timecourse of embryonic human uterine development. | The data below gives an overview of the timecourse of embryonic human uterine development.{{#pmid:12740945|PMID12740945}} | ||
:'''Carnegie stage 18''' - Mullerian duct to the coelomic cavity was formed as the result of an invagination of the coelomic epithelium - [[Carnegie_stage_18|stage 18]] | :'''Carnegie stage 18''' - Mullerian duct to the coelomic cavity was formed as the result of an invagination of the coelomic epithelium - [[Carnegie_stage_18|stage 18]] | ||
| Line 129: | Line 131: | ||
== Fetal Uterus Growth == | == Fetal Uterus Growth == | ||
[[File:Fetal_uterus_growth.jpg|left]] Graph shows the growth during the fetal period of the uterus between week 19 and 38. | [[File:Fetal_uterus_growth.jpg|left]] Graph shows the growth during the fetal period of the uterus between week 19 and 38.{{#pmid:10374123|PMID10374123}} During this time the uterine circumferunce increases from about 20 mm to just under 60mm and the width increases from less than 10mm to just over 20 mm. | ||
Uterine horn fimbrial development begins after week 20 and continues after birth. | Uterine horn fimbrial development begins after week 20 and continues after birth. | ||
| Line 186: | Line 188: | ||
* '''Wnt5a''' - expressed in the mesenchyme | * '''Wnt5a''' - expressed in the mesenchyme | ||
In [[Mouse_Timeline_Detailed|mice]], this development sequence occurs between postnatal day (PND) 5 to 7 and involves Wnt up-regulation of Lymphoid Enhancing Factor 1 (Lef1). | In [[Mouse_Timeline_Detailed|mice]], this development sequence occurs between postnatal day (PND) 5 to 7 and involves Wnt up-regulation of Lymphoid Enhancing Factor 1 (Lef1).{{#pmid:22792274|PMID22792274}} | ||
Postnatally both prolactin and estradiol-17 beta (and their receptors) regulate gland development. There are some gland species gestational differences, in both sheep and pigs the glands provide additional histotrophic support by undergoing extensive hyperplasia and hypertrophy.{{#pmid:11673245|PMID11673245}} | |||
:'''Links:''' [[Developmental_Signals_-_Wnt|Wnt]] | [[Developmental_Mechanism_-_Epithelial_Mesenchymal_Interaction|Epithelial Mesenchymal Interaction]] | :'''Links:''' [[Developmental_Signals_-_Wnt|Wnt]] | [[Developmental_Mechanism_-_Epithelial_Mesenchymal_Interaction|Epithelial Mesenchymal Interaction]] | ||
| Line 212: | Line 212: | ||
== Abnormalities == | == Abnormalities == | ||
[[File:Female genital and ureter abnormality 02.jpg|thumb|Uterine didelphys, obstructed hemivagina, and ectopic ureter on MR imaging in a 17-year-old girl. | [[File:Female genital and ureter abnormality 02.jpg|thumb|Uterine didelphys, obstructed hemivagina, and ectopic ureter on MR imaging in a 17-year-old girl.{{#pmid:19924410|PMID19924410}}]] | ||
There are at least two clinical society classifications for female genital tract abnormalities: | There are at least two clinical society classifications for female genital tract abnormalities: | ||
# European Society of Human Reproduction and Embryology—European Society for Gynaecological Endoscopy (ESHRE-ESGE){{#pmid:23894234|PMID23894234}} | |||
# European Society of Human Reproduction and Embryology—European Society for Gynaecological Endoscopy (ESHRE-ESGE) | # American Society for Reproductive Medicine (ASRM) {{#pmid:3371491|PMID3371491}} | ||
===ESHRE-ESGE Classification=== | ===ESHRE-ESGE Classification=== | ||
European Society for Gynaecological Endoscopy (ESHRE-ESGE) | European Society for Gynaecological Endoscopy (ESHRE-ESGE){{#pmid:23894234|PMID23894234}} | ||
Uterine anatomical deviations deriving from the same embryological origin: | Uterine anatomical deviations deriving from the same embryological origin: | ||
| Line 258: | Line 258: | ||
Uterine residual septum classification: | Uterine residual septum classification: | ||
# American Society for Reproductive Medicine (ASRM) criterion with an internal fundal indentation length equal or greater than 1 cm | # American Society for Reproductive Medicine (ASRM) criterion with an internal fundal indentation length equal or greater than 1 cm{{#pmid:20052665|PMID20052665}} | ||
# European Society of Human Reproduction and Embryology—European Society for Gynaecological Endoscopy (ESHRE-ESGE) classification of female genital tract congenital anomalies with an internal indentation at the fundal midline greater than 50% myometrial thickness. | # European Society of Human Reproduction and Embryology—European Society for Gynaecological Endoscopy (ESHRE-ESGE) classification of female genital tract congenital anomalies with an internal indentation at the fundal midline greater than 50% myometrial thickness.{{#pmid:23894234|PMID23894234}} | ||
[[File:Septate uterus ultrasound 01.jpg|alt=Septate uterus ultrasound|800px]] | [[File:Septate uterus ultrasound 01.jpg|alt=Septate uterus ultrasound|800px]] | ||
Septate Uterus Ultrasound | Septate Uterus Ultrasound{{#pmid:24838703|PMID24838703}} | ||
===Uterine Duplication=== | ===Uterine Duplication=== | ||
| Line 271: | Line 271: | ||
===Uterus/Vaginal=== | ===Uterus/Vaginal=== | ||
Mayer-Rokitansky-Kuster-Hauser syndrome (MRKH, MRK anomaly, Rokitansky-Kuster-Hauser syndrome, RKH syndrome, RKH) consists of congenital aplasia of the uterus and the upper part of vagina due to anomalous development of Müllerian ducts, either isolated or associated with other congenital malformations, including renal, skeletal, hearing and heart defects. Has an incidence of approximately 1 in 4500 newborn girls and has been associated with a microdeletion at 17q12. | Mayer-Rokitansky-Kuster-Hauser syndrome (MRKH, MRK anomaly, Rokitansky-Kuster-Hauser syndrome, RKH syndrome, RKH) consists of congenital aplasia of the uterus and the upper part of vagina due to anomalous development of Müllerian ducts, either isolated or associated with other congenital malformations, including renal, skeletal, hearing and heart defects. Has an incidence of approximately 1 in 4500 newborn girls and has been associated with a microdeletion at 17q12.{{#pmid:19889212|PMID19889212}} | ||
| Line 317: | Line 317: | ||
===Reviews=== | ===Reviews=== | ||
{{#pmid:16208476}} | |||
{{#pmid:15467266}} | |||
===Articles=== | ===Articles=== | ||
{{#pmid:17532316}} | |||
{{#pmid:17070514}} | |||
{{#pmid:12740945}} | |||
===Search PubMed=== | ===Search PubMed=== | ||
| Line 365: | Line 364: | ||
* '''rectouterine pouch''' - (Pouch of Douglas or rectovaginal) Anatomical description of the female peritoneal cavity lying between the back wall of the uterus and rectum. | * '''rectouterine pouch''' - (Pouch of Douglas or rectovaginal) Anatomical description of the female peritoneal cavity lying between the back wall of the uterus and rectum. | ||
* '''sonohysterography''' - A clinical diagnostic technique used to visualise the uterine cavity by ultrasound. Firstly, fluid is injected through the cervix into the uterus, then ultrasound is carried out to image the uterine cavity. | * '''sonohysterography''' - A clinical diagnostic technique used to visualise the uterine cavity by ultrasound. Firstly, fluid is injected through the cervix into the uterus, then ultrasound is carried out to image the uterine cavity. | ||
==External Links== | ==External Links== | ||
| Line 370: | Line 370: | ||
* Blue Histology [http://www.lab.anhb.uwa.edu.au/mb140/CorePages/FemaleRepro/femalerepro.htm#LabOvid Female Reproductive Tract] | * Blue Histology [http://www.lab.anhb.uwa.edu.au/mb140/CorePages/FemaleRepro/femalerepro.htm#LabOvid Female Reproductive Tract] | ||
| Line 377: | Line 376: | ||
{{Footer}} | {{Footer}} | ||
[[Category:Uterus]][[Category:Female]] | [[Category:Uterus]][[Category:Female]] | ||
Revision as of 17:41, 15 February 2018
| Embryology - 10 Jun 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |

Introduction

This page introduces the uterus as part of the internal female reproductive tract development. Two paramesonephric ducts form from coelomic epithelium extending beside the mesonephric ducts. In the absence of Mullerian Inhibitory Factor these ducts proliferate and grow extending from the vaginal plate on the wall of the urogenital sinus to lie beside the developing ovary. The paired ducts begin to fuse from the vaginal plate end, forming the primordial body of the uterus and the unfused lateral arms form the uterine tubes. Recent research points to the paramesonephric ducts also being the entire embryonic origin of the vagina.
- Johannes Peter Müller (1801 - 1858) in 1830 was the first to describe the duct historically named after him, the "Müllerian duct". The current terminology is the "paramesonephric duct".
For the pregnant uterus see Implantation and Maternal Decidua.
| Menstrual Cycle Links: Introduction | menstrual histology | ovary | corpus luteum | oocyte | uterus | Uterine Gland | estrous cycle | pregnancy test | ||
|
| Implantation | Maternal Decidua | Category:Uterus
Some Recent Findings
|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Uterus Development <pubmed limit=5>Uterus Development</pubmed> |
Paramesonephric Duct
The Müllerian duct (= paramesonephric duct, preferred terminology) paired ducts that form the epithelial lining of female reproductive organs: utererine tube, uterus, upper vaginal canal. The term "paramesonephric" duct means beside the mesonephric (Wolffian) duct, which is its anatomical location in early development. Mullerian refers to Johannes Peter Müller (1801-1858) a German scientist who specialised in comparative anatomy. These ducts initially form and then degenerate in the male.
A recent study using both chicken and mouse embryos has shown that these initially paired tubular structures derive from the coelomic epithelium.[5]
- "Müllerian epithelial tube derived from an epithelial anlage at the mesonephros anterior end, which then segregates from the epithelium and extends caudal of its own accord, via a process involving rapid cell proliferation. This tube is surrounded by mesenchymal cells derived from local delamination of coelomic epithelium."
Mullerian ducts have three elements:
- a canalised epithelial tube
- mesenchymal cells surrounding the tube
- coelomic epithelial cells
Duct Molecular Development
The paired paramesonephic ducts (Müllerian ducts) go through a series of developmental changes recently identified as regulated by a number of molecular factors.
Initiation
Coelomic epithelium Lim1 expressing cells are specified to a duct fate.[7]
- Lim - proteins named for 'LIN11, ISL1, and MEC3,' are defined by the possession of a highly conserved double zinc finger motif called the LIM domain.
- LIM domain-binding factors - interact with the LIM domains of nuclear proteins are capable of binding to a variety of transcription factors.
Invagination
Duct invagination induced by Wnt4 to reach the mesonephric (Wolffian)
Elongation
Cells at the leading tip proliferate and form the duct elongating to reach the cloaca (urogenital sinus). Mesonephric secretes WNT9b to guide duct elongation. Pax2 also acts in elongation and duct maintenance.
- WNT9b - member of the WNT protein family that encode cysteine-rich secreted glycoproteins that act as extracellular signaling factors.
- Pax2 - member of the paired box protein family.
- Links: OMIM - WNT9b | OMIM - Pax2 | OMIM - paired box gene
Uterine Development Movie
| Anterior view of development of the female uterus and vagina between Week 9 and 20.
The paramesonephric ducts (red) fuse in the midline to form the genital canal. The urogenital sinus (yellow), in contact with the paramesonephric duct, thickens to form the sinusal tubercle which extends as a solid vaginal plate, then becomes hollow as the sinovaginal bulb, finally forming the vagina.
|
Development Overview

|

|
| Internal Genital Tract Differentiation |
The data below gives an overview of the timecourse of embryonic human uterine development.[8]
- Carnegie stage 18 - Mullerian duct to the coelomic cavity was formed as the result of an invagination of the coelomic epithelium - stage 18
- Carnegie stages 19 - 23 - duct grows independently from the invagination - stage 19
- Week 20 - uterine horn fimbrial development begins and continues after birth - second trimester
Fetal Uterus
|
|

|
| Urogenital sinus of female human embryo of eight and a half to nine weeks old (From model by Keibel) (Image: Gray's Anatomy) | (Image modified from: Drews U, Sulak O, Schenck PA. Androgens and the development of the vagina.Biol Reprod. 2002 Oct;67(4):1353-9. PMID: 12297555) |
Fetal Uterus Growth

Graph shows the growth during the fetal period of the uterus between week 19 and 38.[9] During this time the uterine circumferunce increases from about 20 mm to just under 60mm and the width increases from less than 10mm to just over 20 mm.
Uterine horn fimbrial development begins after week 20 and continues after birth.
Uterine growth continues postnatally, increasing outer muscle thickness and cyclic changes in the lining with puberty.
Adult external uterine orifice to the fundus is approximately 6.25 cm.
Newborn Uterus

| Growth of the Uterus in the Postfetal Period | ||||
|---|---|---|---|---|
| Age | Length of corpus (mm) | Length of isthmus (mm) | Length of cervix (mm) | Total length (mm) |
| Fetus of 7 months | 22 | |||
| Child of 5 weeks | 27 | |||
| 1 year | 10 | 23 | ||
| 14 months | 10 | 5 | 12 | 27 |
| 2.5 years | 8 | 6 | 12 | 26 |
| 3 years | 9-10 | 5-6 | 10 | 25 |
| 3.5 years | 6 | 5 | 16 | 27 |
| 9 years | 9 | 4.5 | 13 | 27 |
| 11 years | 12 | 6 | 19 | 37 |
| 13 years | 27 | 56 | ||
| 15 years | 59 | |||
| 16 years | 41 | 12 | 25 | 78 |
| 17 years | 27 | 6 | 22 | 55 |
| 17 years | 20 | 4 | 16 | 40 |
| 18 years | 36 | 5 | 31 | 72 |
| 19 years | 27 | 5 | 28 | 60 |
| 19 years | 28 | 6 | 27 | 61 |
| 19 years | 24 | 8 | 21 | 53 |
| 20 years | 30 | 6 | 16 | 52 |
| 20 years | 30 | 7 | 21 | 58 |
| 22 years | 35 | 5 | 29 | 69 |
| 28 years | 40 | 10 | 28 | 78 |
| 29 years (nulliparous wife) | 34 | 10 | 34 | 78 |
| 30 years (virgin) | 38 | 7 | 29 | 74 |
| Data compiled from Hegar (1908) | Uterus Growth Table | Collapsible Table | Uterus Development | ||||
Uterine Tubes


The unfused portion of the paramesonephric ducts will form the uterine tubes. Note that there are several synonyms used for the paired uterine tubes or Fallopian tubes or oviducts or uterine horns.
In the adult, the uterine tube has been described in 4 anatomical regions.
- Infundibulum - funnel-shaped open end of the uterine tube with fimbriae (finger-like extensions), which are closely associated with the ovary. Opens into the peritoneal cavity (abdominal ostium, ostium abdominale)
- Ampulla - uterine tube with highly folded structure with plicae (mucosal folds) and secondary folds dividing the lumen, usual site for fertilization.
- Isthmus - narrow portion of the uterine tube with fewer mucosal folds and a thick muscularis layer.
- Intramural - uterine tube which passes through the muscular wall of the uterus. (an alternative interpretation is that it is an extension of the body of the uterus)
Mucosa
- formed by a ciliated and secretory epithelium resting on a very cellular lamina propria.
- The number of ciliated cells and non-ciliated secretory cells varies along the oviduct.
- Secretory activity varies during the menstrual cycle, and resting secretory cells are also referred to as peg-cells.
- Some of the secreted substances are thought to nourish the oocyte and the very early embryo.
Muscularis
- inner circular muscle layer and an outer longitudinal layer.
- An inner longitudinal layer is present in the isthmus and the intramural part of the oviduct.
- Peristaltic muscle action seems to be more important for the transport of sperm and oocyte than the action of the cilia.

Uterine tube (monkey) histology overview

Uterine tube (monkey) epithelium and underlying histology



Uterine Blood Supply

Uterine Glands

Uterine adenogenesis is the term used to describe the formation of uterine glands from the epithelial lining of the uterus that begins prenatal in humans. In other species, the overt development occurs postnatally and has been described through a 3 step the sequence:
- differentiation and budding of the glandular epithelium.
- invagination and tubular coiling of the epithelium.
- branching of the glandular elements and their expansion throughout the endometrial stroma toward the myometrium.
Epithelial-mesenchymal interaction occurs through Wnt signalling during this process:
- Wnt7a - expressed in the luminal epithelium
- Wnt5a - expressed in the mesenchyme
In mice, this development sequence occurs between postnatal day (PND) 5 to 7 and involves Wnt up-regulation of Lymphoid Enhancing Factor 1 (Lef1).[10]
Postnatally both prolactin and estradiol-17 beta (and their receptors) regulate gland development. There are some gland species gestational differences, in both sheep and pigs the glands provide additional histotrophic support by undergoing extensive hyperplasia and hypertrophy.[11]
- Links: Wnt | Epithelial Mesenchymal Interaction
Postnatal Growth
| Growth of the Uterus in the Postfetal Period | ||||
|---|---|---|---|---|
| Age | Length of corpus (mm) | Length of isthmus (mm) | Length of cervix (mm) | Total length (mm) |
| Fetus of 7 months | 22 | |||
| Child of 5 weeks | 27 | |||
| 1 year | 10 | 23 | ||
| 14 months | 10 | 5 | 12 | 27 |
| 2.5 years | 8 | 6 | 12 | 26 |
| 3 years | 9-10 | 5-6 | 10 | 25 |
| 3.5 years | 6 | 5 | 16 | 27 |
| 9 years | 9 | 4.5 | 13 | 27 |
| 11 years | 12 | 6 | 19 | 37 |
| 13 years | 27 | 56 | ||
| 15 years | 59 | |||
| 16 years | 41 | 12 | 25 | 78 |
| 17 years | 27 | 6 | 22 | 55 |
| 17 years | 20 | 4 | 16 | 40 |
| 18 years | 36 | 5 | 31 | 72 |
| 19 years | 27 | 5 | 28 | 60 |
| 19 years | 28 | 6 | 27 | 61 |
| 19 years | 24 | 8 | 21 | 53 |
| 20 years | 30 | 6 | 16 | 52 |
| 20 years | 30 | 7 | 21 | 58 |
| 22 years | 35 | 5 | 29 | 69 |
| 28 years | 40 | 10 | 28 | 78 |
| 29 years (nulliparous wife) | 34 | 10 | 34 | 78 |
| 30 years (virgin) | 38 | 7 | 29 | 74 |
| Data compiled from: Hegar K. Anatomical investigations on the nullipara uterus with special consideration of isthmus (Anatomische Untersuchungen am nullipara Uterus mit besonderer Berücksichtigung der Isthmus). (1908) Beitraae zur Geburtsh. u. Gynak., vol. 13, 1908. reference list | Uterus Growth Table | Collapsible Table | Uterus Development | ||||
Uterus Histology
See also Menstrual Cycle - Histology
Uterine tube histology overview showing epithelium and underlying muscular layers
Uterine tube epithelium histology showing secretory and ciliated cells

Uterine body endometrium and myometrium during the proliferative phase of the menstrual cycle overview

Uterine body endometrium during the proliferative phase of the menstrual cycle

Uterine body endometrium during the secretory phase of the menstrual cycle overview

Uterine body endometrium during the secretory phase of the menstrual cycle



Abnormalities

There are at least two clinical society classifications for female genital tract abnormalities:
- European Society of Human Reproduction and Embryology—European Society for Gynaecological Endoscopy (ESHRE-ESGE)[13]
- American Society for Reproductive Medicine (ASRM) [14]
ESHRE-ESGE Classification
European Society for Gynaecological Endoscopy (ESHRE-ESGE)[13]
Uterine anatomical deviations deriving from the same embryological origin:
- U0 - normal uterus
- U1 - dysmorphic uterus
- U2 - septet uterus
- U3 - bicorporeal uterus
- U4 - hemi-uterus
- U5 - aplastic uterus
- U6 - for still unclassified cases
Main classes have been divided into sub-classes expressing anatomical varieties with clinical significance. Cervical and vaginal anomalies are classified independently into sub-classes having clinical significance.
| ESHRE/ESGE Classification of Uterine Anomalies | |
|---|---|
European Society of Human Reproduction and Embryology (ESHRE) and the European Society for Gynaecological Endoscopy (ESGE)
|

|
| <pubmed>23894234</pubmed>
See also ICD10 Congenital malformations of genital organs (Q50-Q56) | |
Uterine Duplication

|
A range of uterine and vaginal anatomical anomalies based upon the abnormal development and fusion of the paramesonephric ducts and vaginal plate development.
| |||

|
Unicornate Uterus - failure of the paramesonephric ducts to fuse. A single paramesomnephric duct has fused with the vaginal plate and now opens into the vagina, while the other forms a diverticulum.
|

Bicornuate uterus containing conceptus chorionic sac with placental cord on one side.
Septate Uterus
Uterine residual septum classification:
- American Society for Reproductive Medicine (ASRM) criterion with an internal fundal indentation length equal or greater than 1 cm[15]
- European Society of Human Reproduction and Embryology—European Society for Gynaecological Endoscopy (ESHRE-ESGE) classification of female genital tract congenital anomalies with an internal indentation at the fundal midline greater than 50% myometrial thickness.[13]

Septate Uterus Ultrasound[16]
Uterine Duplication
(uterus didelphys, double uterus, uterus didelphis) A rare uterine developmental abnormality where the paramesonephric ducts (Mullerian ducts) completely fail to fuse generating two separate uterus parts each connected to the cervix and having an ovary each.
Uterus/Vaginal
Mayer-Rokitansky-Kuster-Hauser syndrome (MRKH, MRK anomaly, Rokitansky-Kuster-Hauser syndrome, RKH syndrome, RKH) consists of congenital aplasia of the uterus and the upper part of vagina due to anomalous development of Müllerian ducts, either isolated or associated with other congenital malformations, including renal, skeletal, hearing and heart defects. Has an incidence of approximately 1 in 4500 newborn girls and has been associated with a microdeletion at 17q12.[17]
Cervical: cervical agenesis, cervical duplication
Environmental Abnormalities
DES Diethylstilbestrol or diethylstilbetrol, is a drug that was prescribed to women from 1938-1971 to prevent miscarriage in high-risk pregnancies. The drug acted as a potent estrogen (mimics natural hormone) and therefore could also act as a potential endocrine disruptor. This led to a number of developing fetal reproductive tract and other abnormalities. In the female fetus, it increased risk of abnormal reproductive tract and also carcinogenic (cancer forming). In the male fetus, it increased the occurance of abnormal genitalia. The drug was banned by FDA (USA) in 1979 as a teratogen, it had previously also been used as livestock growth promoter and could have potentially entered the human food chain. (More? [endocrine2.htm Endocrine Abnormalities] | Abnormal Development - Drugs)
- Links: Endocrine Abnormalities | Abnormal Development - Drugs | Childrens Hospital Boston - Congenital Anomalies of the Uterus | Medical Education Image Link - Cervical agenesis | OMIM - Rokitansky-Kuster-Hauser syndrome |
Broad Ligament
| The broad ligament is found associated with the internal human female genital tract. It forms a mesentery consisting of a double fold of the peritoneum that connects the uterus to the peritoneal floor and walls.
Anatomically it has three parts:
Abnormalities include peritoneal endometriosis. |

|
Molecular
Wnt genes - Wnt4, Wnt5a, and Wnt7a implicated in the formation and morphogenesis of the Müllerian duct.
Wnt7a - mediates the patterning of the oviduct and differentiation of the uterus.
beta-catenin - manufactured in the mesenchyme is a downstream effector of Wnt7a.
Bmp2 - decidualization regulator of gene expression and function (shown in mouse uterus).
Lim1, Lhx9, Emx, Pax-2, Hox-A9, Hox-A10, Hox-A11, Hox-A13, WT1, SF-1, GATA-4. TGF-beta
References
- ↑ Roly ZY, Backhouse B, Cutting A, Tan TY, Sinclair AH, Ayers KL, Major AT & Smith CA. (2018). The cell biology and molecular genetics of Müllerian duct development. Wiley Interdiscip Rev Dev Biol , , . PMID: 29350886 DOI.
- ↑ Prior M, Richardson A, Asif S, Polanski L, Parris-Larkin M, Chandler J, Fogg L, Jassal P, Thornton JG & Raine-Fenning NJ. (2018). Outcome of assisted reproduction in women with congenital uterine anomalies: a prospective observational study. Ultrasound Obstet Gynecol , 51, 110-117. PMID: 29055072 DOI.
- ↑ Prunskaite-Hyyryläinen R, Skovorodkin I, Xu Q, Miinalainen I, Shan J & Vainio SJ. (2016). Wnt4 coordinates directional cell migration and extension of the Müllerian duct essential for ontogenesis of the female reproductive tract. Hum. Mol. Genet. , 25, 1059-73. PMID: 26721931 DOI.
- ↑ Huang CC, Orvis GD, Kwan KM & Behringer RR. (2014). Lhx1 is required in Müllerian duct epithelium for uterine development. Dev. Biol. , 389, 124-36. PMID: 24560999 DOI.
- ↑ 5.0 5.1 Guioli S, Sekido R & Lovell-Badge R. (2007). The origin of the Mullerian duct in chick and mouse. Dev. Biol. , 302, 389-98. PMID: 17070514 DOI.
- ↑ Deutscher E & Hung-Chang Yao H. (2007). Essential roles of mesenchyme-derived beta-catenin in mouse Müllerian duct morphogenesis. Dev. Biol. , 307, 227-36. PMID: 17532316 DOI.
- ↑ Kobayashi A, Shawlot W, Kania A & Behringer RR. (2004). Requirement of Lim1 for female reproductive tract development. Development , 131, 539-49. PMID: 14695376 DOI.
- ↑ Hashimoto R. (2003). Development of the human Müllerian duct in the sexually undifferentiated stage. Anat Rec A Discov Mol Cell Evol Biol , 272, 514-9. PMID: 12740945 DOI.
- ↑ Soriano D, Lipitz S, Seidman DS, Maymon R, Mashiach S & Achiron R. (1999). Development of the fetal uterus between 19 and 38 weeks of gestation: in-utero ultrasonographic measurements. Hum. Reprod. , 14, 215-8. PMID: 10374123
- ↑ Shelton DN, Fornalik H, Neff T, Park SY, Bender D, DeGeest K, Liu X, Xie W, Meyerholz DK, Engelhardt JF & Goodheart MJ. (2012). The role of LEF1 in endometrial gland formation and carcinogenesis. PLoS ONE , 7, e40312. PMID: 22792274 DOI.
- ↑ Gray CA, Bartol FF, Tarleton BJ, Wiley AA, Johnson GA, Bazer FW & Spencer TE. (2001). Developmental biology of uterine glands. Biol. Reprod. , 65, 1311-23. PMID: 11673245
- ↑ Wang ZJ, Daldrup-Link H, Coakley FV & Yeh BM. (2010). Ectopic ureter associated with uterine didelphys and obstructed hemivagina: preoperative diagnosis by MRI. Pediatr Radiol , 40, 358-60. PMID: 19924410 DOI.
- ↑ 13.0 13.1 13.2 Grimbizis GF, Gordts S, Di Spiezio Sardo A, Brucker S, De Angelis C, Gergolet M, Li TC, Tanos V, Brölmann H, Gianaroli L & Campo R. (2013). The ESHRE-ESGE consensus on the classification of female genital tract congenital anomalies. Gynecol Surg , 10, 199-212. PMID: 23894234 DOI.
- ↑ . (1988). The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil. Steril. , 49, 944-55. PMID: 3371491
- ↑ Bermejo C, Martínez Ten P, Cantarero R, Diaz D, Pérez Pedregosa J, Barrón E, Labrador E & Ruiz López L. (2010). Three-dimensional ultrasound in the diagnosis of Müllerian duct anomalies and concordance with magnetic resonance imaging. Ultrasound Obstet Gynecol , 35, 593-601. PMID: 20052665 DOI.
- ↑ Ludwin A, Ludwin I, Pityński K, Banas T & Jach R. (2014). Role of morphologic characteristics of the uterine septum in the prediction and prevention of abnormal healing outcomes after hysteroscopic metroplasty. Hum. Reprod. , 29, 1420-31. PMID: 24838703 DOI.
- ↑ Bernardini L, Gimelli S, Gervasini C, Carella M, Baban A, Frontino G, Barbano G, Divizia MT, Fedele L, Novelli A, Béna F, Lalatta F, Miozzo M & Dallapiccola B. (2009). Recurrent microdeletion at 17q12 as a cause of Mayer-Rokitansky-Kuster-Hauser (MRKH) syndrome: two case reports. Orphanet J Rare Dis , 4, 25. PMID: 19889212 DOI.
Reviews
Farage M & Maibach H. (2006). Lifetime changes in the vulva and vagina. Arch. Gynecol. Obstet. , 273, 195-202. PMID: 16208476 DOI.
Cummings AM & Kavlock RJ. (2004). Function of sexual glands and mechanism of sex differentiation. J Toxicol Sci , 29, 167-78. PMID: 15467266
Articles
Deutscher E & Hung-Chang Yao H. (2007). Essential roles of mesenchyme-derived beta-catenin in mouse Müllerian duct morphogenesis. Dev. Biol. , 307, 227-36. PMID: 17532316 DOI.
Guioli S, Sekido R & Lovell-Badge R. (2007). The origin of the Mullerian duct in chick and mouse. Dev. Biol. , 302, 389-98. PMID: 17070514 DOI.
Hashimoto R. (2003). Development of the human Müllerian duct in the sexually undifferentiated stage. Anat Rec A Discov Mol Cell Evol Biol , 272, 514-9. PMID: 12740945 DOI.
Search PubMed
Search May 2007 "embryonic uterine development" 3,025 reference articles of which 491 were reviews.
Search Pubmed: Uterus Development | embryonic uterine development | Paramesonephric Duct | Mullerian Duct | Endocrine Disruptors | uterine+adenogenesis
Additional Images

Human uterine tube ciliated epithelium SEM

Urogenital indifferent

Urogenital female
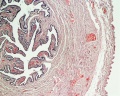
Mouse - paramesonephric duct

Ultrasound uterine and ovarian vascularity

Unicornate uterus

Historic drawing of the uterine tube (Reinier De Graaf)

Cervical mucus plug






Terms
Note some of these terms relate to the adult or the maternal uterus during pregnancy.
- cervical cerclage - A clinical birth procedure involving circumferential banding or suture of the cervix early (between 12 -14 weeks) or when required to prevent or treat passive dilation prior to completion of pregnancy (37 weeks), described as cervical insufficiency.
- cervical insufficiency - (CI) A clinical term describing a painless and progressive dilatation and effacement of the cervix that may lead to second trimester abortions or preterm delivery. It has also been described as inability of the uterine cervix to retain a pregnancy in the absence of uterine contractions. The condition may in some instances treated clinically by cervical cerclage. The biological basis is currently undetermined with some evidence showing a genetic relationship.
- cervical length - There is some data that shows the risk of spontaneous preterm labour and delivery increases in women who have a short cervix PMID 8569824.
- cervical mucus plug - (CMP) During early pregnancy, maternal glands located at the cervical junction between vagina and uterus secrete mucus that forms a plug or barrier between these two structures.
- cervical pregnancy - A rare type of ectopic pregnancy with implantation at the cervical canal, occurring with an incidence ranging between 1:1,000 and 1:18,000 pregnancies. Clinically, when an associated haemorrhage occurs a hysterectomy is usually performed.
- cervical ripening - Clinical birth term describing the hormonal softening of the cervix to allow expansion in preparation for birth.
- cervix - (Latin, cervix = neck) The female anatomical region of the uterus forming a canal that opens and connects to the vagina.
- fallopian tube obstruction - (tubal occlusion) A blockage of the uterine tube that can affect fertility due to a pathologic occlusion, spasm or plugging and also be either unilateral (single tube) or bilateral (both tubes). Described anatomically as in the proximal, the mid or the distal part of the tube.
- fundus - (Latin, fundus = "bottom") Top part of the uterus body lying between the two uterine tubes and a common implantation site.
- hysterosalpingography - A clinical diagnostic technique used to visualise the uterine cavity by X-ray.
- hysteroscopy - A clinical diagnostic technique used to visualise the uterine cavity by a camera or video.
- Pouch of Douglas - (rectouterine pouch or rectovaginal) Anatomical description of the female peritoneal cavity lying between the back wall of the uterus and rectum.
- rectouterine pouch - (Pouch of Douglas or rectovaginal) Anatomical description of the female peritoneal cavity lying between the back wall of the uterus and rectum.
- sonohysterography - A clinical diagnostic technique used to visualise the uterine cavity by ultrasound. Firstly, fluid is injected through the cervix into the uterus, then ultrasound is carried out to image the uterine cavity.
External Links
External Links Notice - The dynamic nature of the internet may mean that some of these listed links may no longer function. If the link no longer works search the web with the link text or name. Links to any external commercial sites are provided for information purposes only and should never be considered an endorsement. UNSW Embryology is provided as an educational resource with no clinical information or commercial affiliation.
- Blue Histology Female Reproductive Tract
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, June 10) Embryology Uterus Development. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Uterus_Development
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G