Abnormal Development - Cleft Lip and Palate
| Embryology - 26 Jul 2026 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
LA40 Cleft lip
| ICD-11 |
|---|
| Clefts of lip, alveolus or palate - LA40 Cleft lip - Isolated cleft lip is a fissure type embryopathy extending from the upper lip to the nasal base.
LA40.0 Cleft lip, unilateral | LA40.2 Cleft lip, median LA41 Cleft lip and alveolus - Cleft lip and alveolus is a fissure type embryopathy that involves the upper lip, nasal base and alveolar ridge in variable degrees. |
Introduction




The way in which the upper jaw (maxillae) forms from fusion of the smaller upper prominence of the first pharyngeal arch leads to a common congenital defect in this region called "clefting", which may involve either the upper lip, the palate or both structures.
The palate anatomically separates the nasal cavity from the oral cavity and structurally has a bony (hard) anterior component and a muscular (soft) posterior component ending with the uvula. The oral side of the palate is covered with a squamous stratified (pluristratified) epithelium. The surface of the hard palate of most mammalian species is further thrown into a series of transversal palatal ridges or rugae palatinae. Both the palatal ridge number and arrangement are also species specific.
Neural crest has a major contribution to the palate development and there are a number of molecular, mechanical and morphological steps in involving the fusion of contributing structures including a key epithelial to mesenchymal transition. In palate formation there are two main and separate times and events of development, during embryonic (primary palate) and an early fetal (secondary palate). This separation of events into embryonic and fetal period corresponds closely to the classification of associated palate abnormalities.
The primary palate is formed by two parts:
- maxillary components of the first pharyngeal arch (lateral)
- frontonasal prominence (midline)
The secondary palate can also be divided in two anatomical parts:
- anterior hard palate - ossified (contributions from the maxilla and palatine bones).
- posterior soft palate - muscular.
| Palate Links: palate | cleft lip and palate | cleft palate | head | Category:Palate |
Some Recent Findings
|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Cleft Lip and Palate | Cleft Lip |
| Older papers |
|---|
| These papers originally appeared in the Some Recent Findings table, but as that list grew in length have now been shuffled down to this collapsible table.
See also the Discussion Page for other references listed by year and References on this current page.
|
| Textbooks |
|---|
|

Movies
| Animations | Ultrasound | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
| |||||||||||||||
| Embryo | Fetus | Mouse | |||||||||||||||||
|
|
|
|
||||||||||||||||




Clinical Images
| Uniateral Cleft Lip |
|---|
 
|
| Complete Unilateral cleft lip and palate |
 
|
| Complete bilateral cleft lip and palate |
 
|
Clinical image source[7]
Statistics

Australia
Australian Palate Abnormalities (2002-2003)[9]
| Cleft lip with or without cleft palate (9.2 per 10,000 births) ICD-10 Q36.0, Q36.1, Q36.9, Q37.0–Q37.5, Q37.8, Q37.9 |
A congenital anomaly characterised by a partial or complete clefting of the upper lip, with or without clefting of the alveolar ridge or the hard palate. Excludes a midline cleft of the upper or lower lip and an oblique facial fissure (going towards the eye).
|
| Australian Palate Abnormalities (2002-2003) |
|---|
| Cleft lip with or without cleft palate (9.2 per 10,000 births) ICD-10 Q36.0, Q36.1, Q36.9, Q37.0–Q37.5, Q37.8, Q37.9 |
A congenital anomaly characterised by a partial or complete clefting of the upper lip, with or without clefting of the alveolar ridge or the hard palate. Excludes a midline cleft of the upper or lower lip and an oblique facial fissure (going towards the eye).
|
| Cleft palate without cleft lip (8.1 per 10,000 births) ICD-10 Q35.0–Q35.9 |
A congenital anomaly characterised by a closure defect of the hard and/or soft palate behind the foramen incisivum without a cleft lip. This anomaly includes sub-mucous cleft palate, but excludes cleft palate with a cleft lip, a functional short palate and high narrow palate.
|
|
Victorian Perinatal Data Collection Unit (2003-2004) Top 10 abnormalities, cleft lip and palate was number 10 on the list and the condition occurred with another defect in 33.7% of cases.
Ten most frequently reported Birth Anomalies
- Hypospadias (More? Male movie | Genital Abnormalities - Hypospadia)
- Obstructive Defects of the Renal Pelvis (More? Renal System - Abnormalities)
- Ventricular Septal Defect (More? Cardiovascular Abnormalities - Ventricular Septal Defect)
- Congenital Dislocated Hip (More? Musculoskelal Abnormalities - Congenital Dislocation of the Hip (CDH))
- Trisomy 21 or Down syndrome - (More? Trisomy 21)
- Hydrocephalus (More? Hydrocephalus)
- Cleft Palate (More? Palate_Development)
- Trisomy 18 or Edward Syndrome - multiple abnormalities of the heart, diaphragm, lungs, kidneys, ureters and palate 86% discontinued (More? (More? Trisomy 18)
- Renal Agenesis/Dysgenesis - reduction in neonatal death and stillbirth since 1993 may be due to the more severe cases being identified in utero and being represented amongst the increased proportion of terminations (approximately 31%). (More? Renal System - Abnormalities)
- Cleft Lip and Palate - occur with another defect in 33.7% of cases.(More? Palate Development | Head Development)
(From the Victorian Perinatal Data Collection Unit in the Australian state of Victoria between 2003-2004)
USA
| Male preponderance | Female preponderance |
|---|---|
|
|
| Cardiac defects | |
|
|
| Table data[10] Links: abnormal development | cardiovascular abnormalities | USA | Male | Female | cleft lip and palate | |
Development Overview
- week 4 - pharyngeal arch formation, first pharngeal arch contributes mandible and maxilla.
- week 6 - 7 - primary palate formation maxillary processes and frontonasal prominence.
- week 9 - secondary palate shelves fuse, separating oral and nasal cavities.
Embryonic Period
- (week 4) - pharyngeal arch formation in rostrocaudal sequence (1, 2, 3, 4 and 6)
- First pharyngeal arch - upper maxillary (pair) and lower mandibular prominences
- Late embryonic period - maxillary prominences fuse with frontonasal prominence forming upper jaw (maxilla and upper lip)



Fetal Period
|
|
Neural Crest
- Mesenchyme invaded by neural crest generating connective tissue components
- cartilage, bone, ligaments
- arises from midbrain and hindbrain region
Face Development

Begins week 4 centered around stomodeum, external depression at oral membrane
5 initial primordia from neural crest mesenchyme
- single frontonasal prominence (FNP) - forms forehead, nose dorsum and apex
- nasal placodes develop later bilateral, pushed medially
- paired maxillary prominences - form upper cheek and upper lip
- paired mandibular prominences - lower cheek, chin and lower lip
Frontonasal Process
The frontonasal process (FNP) forms the majority of the superior part of the early face primordia. It later fuses with the maxillary component of the first pharyngeal arch to form the upper jaw. Failure of this fusion event during the embryonic period leads to cleft lip. Under the surface ectoderm the process mesenchyme consists of two cell populations; neural crest cells, forming the connective tissues; and the mesoderm forming the endothelium of the vascular network.
Embryonic Palate
|
Human primary palate |

|
- EM Links: [[:File:Stage16 em01.jpg|Image - stage 16]] | [[:File:Stage17 em01.jpg|Image - stage 17]] | [[:File:Stage18 em01.jpg|Image - stage 18]] | [[:File:Stage19 em01.jpg|Image - stage 19]] | Palate Development
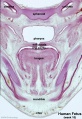
Fetal Palate
Secondary palate, fusion in the human embryo in week 9. This requires the early palatal shelves growth, elevation, and fusion. There are many fusion events occurring during this period between each palatal shelf, to the primary palate, and also to the nasal septum.
palatal shelf elevation | secondary palate

Hard and soft palate

hard palate

hard palate labeled
soft palate
soft palate labeled
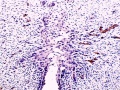
Detail - hard and soft palate junction

Detail - hard palate seam








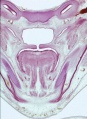
Ventral aspect of hard palate of human embryo of 80 mm
Neonatal Palate

Surgical repair of the lip (cheiloplasty).[7]
Feeding
Both cleft lip and palate provide issues related to both feeding and nutrition before a surgical repair can be carried out.[12][13]
|

Cleft palate feeder |
Hearing
| Note also the neonatal association with conductive hearing loss from serous effusion with cleft lip and palate.[14] Tympanostomy tubes can help with some but not all these neonates.
|

Newborn hearing test |
Preterm
- Links: Birth - Preterm
Animal Models

Mouse Palate
- E11 - protrude from bilateral maxillary processes
- E12.5 - secondary palatal development begins
- E12.5-E14 - grow vertically along the developing tongue
- E14.5 - they elevate, meet, and fuse at the midline, to form an intact palate shelf, reflex opening and closing movements of the mouth
- E15.5 - palatal fusion is complete, mesenchymal condensation followed by osteogenic differentiation occurs.
- Links: Mouse Development | Bone Morphogenetic Protein | Wnt | Pax
International Classification of Diseases
Cleft lip and cleft palate (Q35-Q37)
Use additional code (Q30.2), if desired, to identify associated malformations of the nose. Excludes Robin's syndrome ( Q87.0 )
| Q37 | Cleft palate with cleft lip |
| Q37.0 | Cleft hard palate with bilateral cleft lip |
| Q37.1 | Cleft hard palate with unilateral cleft lip |
| Cleft hard palate with cleft lip NOS | |
| Q37.2 | Cleft soft palate with bilateral cleft lip |
| Q37.3 | Cleft soft palate with unilateral cleft lip |
| Cleft soft palate with cleft lip NOS | |
| Q37.4 | Cleft hard and soft palate with bilateral cleft lip |
| Q37.5 | Cleft hard and soft palate with unilateral cleft lip |
| Cleft hard and soft palate with cleft lip NOS | |
| Q37.8 | Unspecified cleft palate with bilateral cleft lip |
| Q37.9 | Unspecified cleft palate with unilateral cleft lip |
| Cleft palate with cleft lip NOS |
Cleft Lip
| Cleft Lip Genes[17] | ||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Midline Cleft Lip Genes
| ||||||||||||||||||||||||||||||||||||||
|
Cleft Lip (+/− cleft palate) Genes
|
Cleft Risk Variants
Two genes were identified from a recent genome-wide study.[6]
- MAFB is expressed in the mouse palatal shelf.
- ABCA4 is a member of a superfamily of transmembrane proteins, and mutations in ABCA4 play a major role in the etiology of Stargardt disease and related retinopathies. Gene produces an ATP-binding cassette (ABC) superfamily trans-membrane protein
- Links: OMIM - MAFB | OMIM - ABCA4
Folate
A recent study of periconceptional folate supplementation using the Cochrane Pregnancy and Childbirth Group's Trials Register (July 2010) identified no statistically significant evidence of any effects on prevention of cleft palate and cleft lip at birth.[18]
Molecular
SATB2 - Special At-Rich Sequence-Binding Protein has a role in craniofacial development and patterning.PubmedParser error: The PubmedParser extension received invalid XML data. ()
P63 - cleft palate is a form of ectodermal dysplasia and functioning p63 prevents dysplasia.
TBX22 - has been identified as expressed in the palatal shelves during the elevation process.
TGFBR3 - Transforming Growth Factor-Beta Receptor Type III loss of signaling by receptor loss was found to be associated with cleft palate formation due to aberrant cell cycle progression and altered gene expression.
References
- ↑ Marini NJ, Asrani K, Yang W, Rine J & Shaw GM. (2019). Accumulation of rare coding variants in genes implicated in risk of human cleft lip with or without cleft palate. Am. J. Med. Genet. A , , . PMID: 31063268 DOI.
- ↑ Hlongwa P, Levin J & Rispel LC. (2019). Epidemiology and clinical profile of individuals with cleft lip and palate utilising specialised academic treatment centres in South Africa. PLoS ONE , 14, e0215931. PMID: 31071123 DOI.
- ↑ Chiquet BT, Yuan Q, Swindell EC, Maili L, Plant R, Dyke J, Boyer R, Teichgraeber JF, Greives MR, Mulliken JB, Letra A, Blanton SH & Hecht JT. (2018). Knockdown of Crispld2 in zebrafish identifies a novel network for nonsyndromic cleft lip with or without cleft palate candidate genes. Eur. J. Hum. Genet. , , . PMID: 29899370 DOI.
- ↑ Allori AC, Mulliken JB, Meara JG, Shusterman S & Marcus JR. (2017). Classification of Cleft Lip/Palate: Then and Now. Cleft Palate Craniofac. J. , 54, 175-188. PMID: 26339868 DOI.
- ↑ Letra A, Zhao M, Silva RM, Vieira AR & Hecht JT. (2014). Functional Significance of MMP3 and TIMP2 Polymorphisms in Cleft Lip/Palate. J. Dent. Res. , 93, 651-6. PMID: 24799419 DOI.
- ↑ 6.0 6.1 Beaty TH, Murray JC, Marazita ML, Munger RG, Ruczinski I, Hetmanski JB, Liang KY, Wu T, Murray T, Fallin MD, Redett RA, Raymond G, Schwender H, Jin SC, Cooper ME, Dunnwald M, Mansilla MA, Leslie E, Bullard S, Lidral AC, Moreno LM, Menezes R, Vieira AR, Petrin A, Wilcox AJ, Lie RT, Jabs EW, Wu-Chou YH, Chen PK, Wang H, Ye X, Huang S, Yeow V, Chong SS, Jee SH, Shi B, Christensen K, Melbye M, Doheny KF, Pugh EW, Ling H, Castilla EE, Czeizel AE, Ma L, Field LL, Brody L, Pangilinan F, Mills JL, Molloy AM, Kirke PN, Scott JM, Scott JM, Arcos-Burgos M & Scott AF. (2010). A genome-wide association study of cleft lip with and without cleft palate identifies risk variants near MAFB and ABCA4. Nat. Genet. , 42, 525-9. PMID: 20436469 DOI.
- ↑ 7.0 7.1 Freitas JA, das Neves LT, de Almeida AL, Garib DG, Trindade-Suedam IK, Yaedú RY, Lauris Rde C, Soares S, Oliveira TM & Pinto JH. (2012). Rehabilitative treatment of cleft lip and palate: experience of the Hospital for Rehabilitation of Craniofacial Anomalies/USP (HRAC/USP)--Part 1: overall aspects. J Appl Oral Sci , 20, 9-15. PMID: 22437671
- ↑ P. Lancaster and E. Pedisich, Congenital Malformations Australia 1981-1992, ISSN 1321-835.
- ↑ Abeywardana S & Sullivan EA 2008. Congenital Anomalies in Australia 2002-2003. Birth anomalies series no. 3 Cat. no. PER 41. Sydney: AIHW National Perinatal Statistics Unit.
- ↑ Michalski AM, Richardson SD, Browne ML, Carmichael SL, Canfield MA, VanZutphen AR, Anderka MT, Marshall EG & Druschel CM. (2015). Sex ratios among infants with birth defects, National Birth Defects Prevention Study, 1997-2009. Am. J. Med. Genet. A , 167A, 1071-81. PMID: 25711982 DOI.
- ↑ Diewert VM & Lozanoff S. (1993). A morphometric analysis of human embryonic craniofacial growth in the median plane during primary palate formation. J. Craniofac. Genet. Dev. Biol. , 13, 147-61. PMID: 8227288
- ↑ Paradise JL & McWilliams BJ. (1974). Simplified feeder for infants with cleft palate. Pediatrics , 53, 566-8. PMID: 4823331
- ↑ Campbell AN & Tremouth MJ. (1987). New feeder for infants with cleft palate. Arch. Dis. Child. , 62, 1292. PMID: 3435170
- ↑ Chen JL, Messner AH & Curtin G. (2008). Newborn hearing screening in infants with cleft palates. Otol. Neurotol. , 29, 812-5. PMID: 18617869 DOI.
- ↑ Eifinger F, Lang-Roth R, Braumann B, Saffar M, Huenseler C & Kribs A. (2008). Primary respiratory support in preterm infants with cleft lip and palate. J Laryngol Otol , 122, 307-9. PMID: 17666126 DOI.
- ↑ McMahon RM, Bagchi I, Worsey S & Kumararatne B. (2006). Use of mask continuous positive airway pressure in a preterm infant presenting with bilateral cleft lip and palate. J Laryngol Otol , 120, 228-9. PMID: 16460577 DOI.
- ↑ Dixon MJ, Marazita ML, Beaty TH & Murray JC. (2011). Cleft lip and palate: understanding genetic and environmental influences. Nat. Rev. Genet. , 12, 167-78. PMID: 21331089 DOI.
- ↑ De-Regil LM, Fernández-Gaxiola AC, Dowswell T & Peña-Rosas JP. (2010). Effects and safety of periconceptional folate supplementation for preventing birth defects. Cochrane Database Syst Rev , , CD007950. PMID: 20927767 DOI.
Journals
- The Cleft Palate-Craniofacial Journal Homepage | Available issues
Reviews
Indian J Plast Surg. 2009 October; 42(Suppl):Cleft Lip and Palate Issue Bush JO & Jiang R. (2012). Palatogenesis: morphogenetic and molecular mechanisms of secondary palate development. Development , 139, 231-43. PMID: 22186724 DOI.
Meng L, Bian Z, Torensma R & Von den Hoff JW. (2009). Biological mechanisms in palatogenesis and cleft palate. J. Dent. Res. , 88, 22-33. PMID: 19131313 DOI.
Dudas M, Li WY, Kim J, Yang A & Kaartinen V. (2007). Palatal fusion - where do the midline cells go? A review on cleft palate, a major human birth defect. Acta Histochem. , 109, 1-14. PMID: 16962647 DOI.
Ferguson MW. (1988). Palate development. Development , 103 Suppl, 41-60. PMID: 3074914
Hay ED. (1995). An overview of epithelio-mesenchymal transformation. Acta Anat (Basel) , 154, 8-20. PMID: 8714286
Articles
Steding G & Jian Y. (2010). The origin and early development of the nasal septum in human embryos. Ann. Anat. , 192, 82-5. PMID: 20149609 DOI.
Xiong W, He F, Morikawa Y, Yu X, Zhang Z, Lan Y, Jiang R, Cserjesi P & Chen Y. (2009). Hand2 is required in the epithelium for palatogenesis in mice. Dev. Biol. , 330, 131-41. PMID: 19341725 DOI.
Search PubMed
Search Pubmed: cleft lip and palate development |
Additional Images

Unilateral cleft lip and palate

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Terms
| Palate Development (expand to see terms) |
|---|
|
| Other Terms Lists |
|---|
| Terms Lists: ART | Birth | Bone | Cardiovascular | Cell Division | Endocrine | Gastrointestinal | Genital | Genetic | Head | Hearing | Heart | Immune | Integumentary | Neonatal | Neural | Oocyte | Palate | Placenta | Radiation | Renal | Respiratory | Spermatozoa | Statistics | Tooth | Ultrasound | Vision | Historic | Drugs | Glossary |
External Links
External Links Notice - The dynamic nature of the internet may mean that some of these listed links may no longer function. If the link no longer works search the web with the link text or name. Links to any external commercial sites are provided for information purposes only and should never be considered an endorsement. UNSW Embryology is provided as an educational resource with no clinical information or commercial affiliation.
- Medline Plus - Cleft Lip and Palate
- Better Health Channel - Cleft palate and cleft lip
- March of Dimes Birth Defects Foundation - Cleft Palate
- Victoria Neonatal ehandbook - Cleft Lip and Palate | Royal Children's Hospital Melbourne
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2026, July 26) Embryology Abnormal Development - Cleft Lip and Palate. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Abnormal_Development_-_Cleft_Lip_and_Palate
- © Dr Mark Hill 2026, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G