SH Lecture - Respiratory System Development: Difference between revisions
mNo edit summary |
mNo edit summary |
||
| Line 13: | Line 13: | ||
:''Current research suggests that both genetic and the developmental environment (fetal and postnatal) can influence the growth, differentiation and function of the respiratory system.'' | :''Current research suggests that both genetic and the developmental environment (fetal and postnatal) can influence the growth, differentiation and function of the respiratory system.'' | ||
[[Media:SH Lecture 2018 - Respiratory System Development.pdf|'''2018 Respiratory Development Lecture PDF''']] | |||
Revision as of 12:33, 2 March 2018
| Embryology - 16 Jun 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Introduction




|
The lecture will introduce the development of the respiratory system and associated structures. The lecture will not cover adult anatomy, physiology of gas exchange, red blood cell function, cardiovascular development and will leave detailed histology to your associated practical class. | 
|
- Current research suggests that both genetic and the developmental environment (fetal and postnatal) can influence the growth, differentiation and function of the respiratory system.
2018 Respiratory Development Lecture PDF
- Lecture: 2017 | 2017 PDF | 2016 | 2016 PDF | 2015 | 2015 PDF | 2014 | Lecture 2014 PDF | 2013 PDF | 2013 | 2012 | 2012 PDF (10 pages) | eMed Link to Learning Activity - Respiratory System Development
- SH Links: Lymphatic Lecture | Lymphatics Practical Support | Respiratory Lecture | Respiratory Practical Support | Medicine
The respiratory system does not carry out its physiological function (of gas exchange) until after birth, though the respiratory tract, diaphragm and lungs do begin to form early in embryonic development and continue through fetal development, only functionally maturing just before birth. The lungs continue to grow postnatally through childhood and some research finding suggest that there remains potential for growth in the adult.
The respiratory tract is divided anatomically into 2 main parts:
- upper respiratory tract - consisting of the nose, nasal cavity and the pharynx.
- lower respiratory tract - consisting of the larynx, trachea, bronchi and the lungs.
The respiratory "system" usually includes descriptions of not only the functional development of the lungs, but also related musculoskeletal (diaphragm) and vascular (pulmonary) development.
AimTo understand the prenatal and postnatal developmental anatomy of human respiratory organs.
|
Key Concepts
| ||||||||||||



Respiratory Functional Unit
Alveolus
Alveolus (Latin alveolus = "little cavity", plural is alveoli)

|

|
| Alveolus histology | Alveolus structure |

|

|
Primary Lobule
|
Secondary Lobule
|
Developmental Overview

Germ Layers
- Endoderm and splanchnic mesoderm form majority of conducting and alveoli.
- Ectoderm will contribute the neural innervation.
- Mesoderm also contributes the supporting musculoskeletal components.
Week 4 - laryngotracheal groove forms on floor foregut.
Week 5 - left and right lung buds push into the pericardioperitoneal canals (primordia of pleural cavity)
Week 6 - descent of heart and lungs into thorax. Pleuroperitoneal foramen closes.
Week 7 - enlargement of liver stops descent of heart and lungs.
Month 3-6 - lungs appear glandular, end month 6 alveolar cells type 2 appear and begin to secrete surfactant.
Month 7 - respiratory bronchioles proliferate and end in alveolar ducts and sacs.
Development Stages
Note - the sequence is important rather than the actual timing, which is variable in the existing literature.
| Lung Stage | Human | Features | Vascular | |
|---|---|---|---|---|
| Embryonic | week 4 to 5 | lung buds originate as an outgrowth from the ventral wall of the foregut where lobar division occurs | extra pulmonary artery then lobular artery | |
| Pseudoglandular | week 5 to 17 | conducting epithelial tubes surrounded by thick mesenchyme are formed, extensive airway branching | Pre-acinar arteries | |
| Canalicular | week 16 to 25 | bronchioles are produced, increasing number of capillaries in close contact with cuboidal epithelium and the beginning of alveolar epithelium development | Intra-acinar arteries | |
| Saccular | week 24 to 40 | alveolar ducts and air sacs are developed | alveolar duct arteries | |
| Alveolar | late fetal to 8 years | secondary septation occurs, marked increase of the number and size of capillaries and alveoli | alveolar capillaries | |
| embryonic stage - pseudoglandular stage - canalicular stage - saccular stage - alveolar stage Links: Species Stage Comparison | respiratory | ||||
Embryonic
Week 4 to 5 - lung buds originate as an outgrowth from the ventral wall of the foregut where lobar division occurs.
|
||

|

| |
| Stomodeum (Week 4, stage 11) | Buccopharyngeal membrane (Week 4, stage 11) | |

(Week 5, stage 14)
- week 4 - 5
- Endoderm - tubular ventral growth from foregut pharynx.
- Mesoderm - mesenchyme of lung buds.
- Intraembryonic coelom - pleural cavities elongated spaces connecting pericardial and peritoneal spaces.
Stage 13 - Trachea and Lung buds

|

|

|

|
| Week 4 | Week 4-5 (Stage 12 to 13) | Week 5 (Stage 15 to 16) | Week 6 (Stage 16 to 17) |
Pseudoglandular stage
Week 8 |

Fetal lung histology |

(This is what a gland looks like.)
Canalicular stage
|

|
Saccular stage
- week 24 to near term.
- most peripheral airways form widened "airspaces", termed saccules.
- saccules widen and lengthen the airspace (by the addition of new generations).
- future gas exchange region expands significantly.
- Fibroblastic cells also undergo differentiation, they produce extracellular matrix, collagen, and elastin.
- May have a role in epithelial differentiation and control of surfactant secretion.
- Alveolar Cells Type II (Type II pneumocytes)
- begin to secrete surfactant, levels of secretion gradually increase to term.
- allows alveoli to remain inflated
- Vascular tree - also grows in length and diameter during this time.
Alveolar stage

|

|
Upper Respiratory Tract


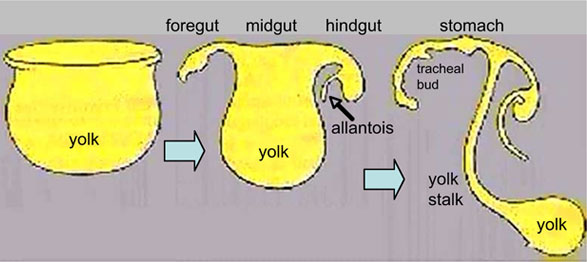
Foregut Development - from the oral cavity the next portion of the foregut is initially a single gastrointestinal (oesophagus) and respiratory (trachea) common tube, the pharynx which lies behind the heart. Note that the respiratory tract will form from a ventral bud arising at this level.

|
Note - Specialised olfactory epithelium for smell, a small region located in roof of nasal cavity. |

|
Respiratory epithelium
Respiratory epithelium development |


Nasal cavities

Larynx

Adult upper respiratory tract conducting system



| Additional Information - Histology | ||
|---|---|---|
This will be covered in detail in your associated SH Practical class.
|



Lower Respiratory Tract
week 4 early respiratory endodermal bud

week 4 later ventral endoderm growth
lower respiratory tract

conducting system bronchi to lungs


|

|
| Stage 13 (Week 4-5) | Stage 22 (Week 8) |
- lung buds ( endoderm epithelial tubes) grow/push into mesenchyme covered with pleural cells (lung border)
- generates a tree-like network by repeated:
- elongation
- terminal bifurcation
- lateral budding
Growth initially of branched "conducting" system of bronchial tree, followed by later development of the "functional units" of the alveoli.
| Additional Information - Histology | ||
|---|---|---|
| This will be covered in detail in your associated SH Practical class.
Respiratory Trachea Mucosa - formed by epithelium and underlying lamina propria.
Submucosa - connective tissue and submucosal glands
Cartilage
Hyaline Cartilage Development
Bronchi Branching main bronchi -> lobar bronchi -> segmental bronchi (supply lung bronchopulmonary segments) -> bronchi -> bronchioles (smaller than 1 mm) -> respiratory bronchioles.
Bronchioles
Respiratory Bronchioles
|









Fetal Lung Volume
Each human lung volume as determined by ultrasound and matched to gestational age[6]
|

|
Pleural Cavity


- anatomical body cavity in which the lungs develop and lie.
- pleural cavity forms in the lateral plate mesoderm as part of the early single intraembryonic coelom.
- This cavity is initially continuous with pericardial and peritoneal cavities and form initially as two narrow canals.
- later becomes separated by folding (pleuropericardial fold, pleuroperitoneal membrane) and the later formation of the diaphragm.
- pleuropericardial fold - (pleuropericardial membrane) An early embryonic fold which restricts the communication between pleural cavity and pericardiac cavity, contains both the cardinal vein and phrenic nerve.
- pleuroperitoneal membrane - An early embryonic membrane that forms inferiorly at the septum transversum to separate peritoneal cavity from pleural cavity.
Pleura
- serous membrane covers the surface of the lung and the spaces between the lobes.
- arranged as a closed invaginated sac.
- two layers (pulmonary, parietal) continuous with each other, the potential space between them is the pleural cavity.
Diaphragm
Adult Diaphragm.

- Not respiratory tract but musculoskeletal development, there are 5 embryonic elements that contribute to the diaphragm.
- Innervation of the human diaphragm is by the phrenic nerves

|
|

- Phrenic Nerves - arising from the same segmental levels as the diaphragm skeletal muscles, segmental levels C3 to C5.
- The paired phrenic nerves are mixed nerves
- motor neurons for the diaphragm
- sensory nerves for other abdominal structures (mediastinum, pleura, liver, gall bladder).
Bochdalek hernia - most common on the posterior left side (85%). Failure of the pleuroperitoneal foramen (foramen of Bochdalek) to close allows viscera into thorax. Intestine, stomach or spleen can enter the pleural cavity, compressing the lung.
Pulmonary Circulation

- the pulmonary system not "functional" until after birth
- pulmonary arteries - 6th aortic arch arteries
- pulmonary veins - are incorporated into the left atrium wall
- bronchial arteries - branches from dorsal aorta
Fetal
Fetal Respiratory Movements
- Fetal respiratory movements (FRM) or Fetal breathing movements (FBM) are regular muscular contrations occurring in the third trimester.
- preparing the respiratory muscular system for neonatal function.
- may also have a role in late lung development.
The First Breath
- The respiratory system does not carry out its physiological function (gas exchange) prenatally and remain entirely fluid-filled until birth.
- At birth, fluid in the upper respiratory tract is expired and fluid in the lung aveoli is rapidly absorbed this event has also been called "dewatering of the lung".
- The lung epithelia has to now rapidly change from its prenatal secretory function to that of fluid absorbtion.
The exchange of lung fluid for air leads to:
- fall in pulmonary vascular resistance
- increase in pulmonary blood flow
- thinning of pulmonary arteries (stretching as lungs increase in size)
- blood fills the alveolar capillaries
In the heart - pressure in the right side of the heart decreases and pressure in the left side of the heart increases (more blood returning from pulmonary).
Postnatal

Alveoli
- At birth about 15% of adult alveoli number have formed
- 20 - 50 million to in the adult about 300 million.
- remaining subdivisions develop in the first few postnatal years
Respiratory Rate
- neonatal rate is higher (30-60 breaths/minute) than adult (12-20 breaths/minute).
- tachypnea - (Greek, rapid breathing) an increased respiratory rate of greater than 60 breaths/minute in a quiet resting baby
| Age | Rate (breaths/minute) |
| Infant (birth - 1 year) | 30 - 60 |
| Toddler (1 - 3 years) | 24 - 40 |
| Preschool (3 - 6 years) | 22 - 34 |
| School age (6 - 12 years) | 18 - 30 |
| Adolescent (12 - 18 years) | 12 - 16 |
Rib Orientation
- Infant rib - is virtually horizontal, allowing diaphragmatic breathing only.
- Adult rib - is oblique (both anterior and lateral views), allows for pump-handle and bucket handle types of inspiration.
Respiratory Tract Abnormalities



Respiratory System - Abnormalities
- Meconium Aspiration Syndrome - (MAS) Meconium is the gastrointestinal contents that accumulate in the intestines during the fetal period. Fetal stress in the third trimester, prior to/at/ or during parturition can lead to premature meconium discharge into the amniotic fluid and sunsequent ingestion by the fetus and damage to respiratory function. Damage to placental vessels meconium myonecrosis may also occur.
- Newborn Respiratory Distress Syndrome - (Hyaline Membrane Disease) membrane-like substance from damaged pulmonary cells, absence of surfactant, if prolonged can be irreversible, intrauterine asphyxia, prematurity and maternal diabetes medline plus | eMedicine
- Tracheoesophageal Fistula - Tracheo-Oesophageal Fistula, Oesophageal Atresia - Oesophageal Atresia with or without tracheo-oesophageal fistula Fistula - an abnormal communication between 2 structures (organs, vessels, cavities) that do not normally connect.
- Lobar Emphysema (Overinflated Lung) - There is an overinflated left upper lobe There is a collapsed lower lobe The left lung is herniating across the mediastinum
- Congenital Diaphragmatic Hernia - (1 in 3,000 live births) Failure of the pleuroperitoneal foramen (foramen of Bochdalek) to close (left side), allows viscera into thorax -iIntestine, stomach or spleen can enter the pleural cavity, compressing the lung. rare (Morgagni hernia) -an opening in the front of the diaphragm. Congenital Diaphragmatic Hernia | GeneReviews
- Azygos Lobe - Common condition (0.5% of population). The right lung upper lobe expands either side of the posterior cardinal. There is also some course variability of the phrenic nerve in the presence of an azygos lobe.
- Congenital Laryngeal Webs - Laryngeal abnormality due to embryonic (week 10) incomplete recanalization of the laryngotracheal tube during the fetal period. Rare abnormality occuring mainly at the level of the vocal folds (glottis).
- Hyaline Membrane Disease - (Newborn Respiratory Distress Syndrome) a membrane-like substance from damaged pulmonary cells.
- Bronchopulmonary Dysplasia - A chronic lung disease which can occur following premature birth and related lung injury. Most infants who develop BPD are born more than 10 weeks before their due dates, weigh less than 1,000 grams (about 2 pounds) at birth, and have breathing problems.
- Asthma - Flow limitation during tidal expiration in early life significantly associated with the development of physician-diagnosed asthma by the age of 2 years. Infants with abnormal lung function soon after birth may have a genetic predisposition to asthma or other airway abnormalities that predict the risk of subsequent lower respiratory tract illness. PMID 8176553
- Cystic Fibrosis - Inherited disease of the mucus and sweat glands, causes mucus to be thick and sticky. Clogging the lungs, causing breathing problems and encouraging bacterial grow. (Covered elsewhere in the course)
Environmental Factors
The lung is most sensitive to environmental effects given the long timecourse of development, including postnatal, multi-system origins, immune interactions, and our growing understanding of the effects of the prenatal environment on adult health (DOHAD). Below are some recent reviews of related topics.(not part of today's lecture presentation)
- Maternal alcohol[4]
- Maternal obesity[7]
- Maternal diabetes[8]
- Maternal smoking[9]
- Chronic hypoxaemia[10]
- Environmental chemicals[11]
Additional Information

| Grays - Respiratory Images |
|---|
|




























| Respiratory Histology |
|---|
|
Histology will be covered in more detail in your associated practical class. Fetal Histology
Adult Histology
|


{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
- ↑ Ardini-Poleske ME, Clark RF, Ansong C, Carson JP, Corley RA, Deutsch GH, Hagood JS, Kaminski N, Mariani TJ, Potter SS, Pryhuber GS, Warburton D, Whitsett JA, Palmer SM & Ambalavanan N. (2017). LungMAP: The Molecular Atlas of Lung Development Program. Am. J. Physiol. Lung Cell Mol. Physiol. , 313, L733-L740. PMID: 28798251 DOI.
- ↑ Schittny JC. (2017). Development of the lung. Cell Tissue Res. , 367, 427-444. PMID: 28144783 DOI.
- ↑ Stabler CT & Morrisey EE. (2017). Developmental pathways in lung regeneration. Cell Tissue Res. , 367, 677-685. PMID: 27957616 DOI.
- ↑ 4.0 4.1 Gauthier TW & Brown LA. (2017). In utero alcohol effects on foetal, neonatal and childhood lung disease. Paediatr Respir Rev , 21, 34-37. PMID: 27613232 DOI.
- ↑ Herriges M & Morrisey EE. (2014). Lung development: orchestrating the generation and regeneration of a complex organ. Development , 141, 502-13. PMID: 24449833 DOI.
- ↑ Peralta CF, Cavoretto P, Csapo B, Falcon O & Nicolaides KH. (2006). Lung and heart volumes by three-dimensional ultrasound in normal fetuses at 12-32 weeks' gestation. Ultrasound Obstet Gynecol , 27, 128-33. PMID: 16388511 DOI.
- ↑ McGillick EV, Lock MC, Orgeig S & Morrison JL. (2017). Maternal obesity mediated predisposition to respiratory complications at birth and in later life: understanding the implications of the obesogenic intrauterine environment. Paediatr Respir Rev , 21, 11-18. PMID: 27818069 DOI.
- ↑ Azad MB, Moyce BL, Guillemette L, Pascoe CD, Wicklow B, McGavock JM, Halayko AJ & Dolinsky VW. (2017). Diabetes in pregnancy and lung health in offspring: developmental origins of respiratory disease. Paediatr Respir Rev , 21, 19-26. PMID: 27665512 DOI.
- ↑ McEvoy CT & Spindel ER. (2017). Pulmonary Effects of Maternal Smoking on the Fetus and Child: Effects on Lung Development, Respiratory Morbidities, and Life Long Lung Health. Paediatr Respir Rev , 21, 27-33. PMID: 27639458 DOI.
- ↑ McGillick EV, Orgeig S, Giussani DA & Morrison JL. (2017). Chronic hypoxaemia as a molecular regulator of fetal lung development: implications for risk of respiratory complications at birth. Paediatr Respir Rev , 21, 3-10. PMID: 27692868 DOI.
- ↑ Miller MD & Marty MA. (2010). Impact of environmental chemicals on lung development. Environ. Health Perspect. , 118, 1155-64. PMID: 20444669 DOI.
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, June 16) Embryology SH Lecture - Respiratory System Development. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/SH_Lecture_-_Respiratory_System_Development
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G