BGDA Practical 3 - Week 2 Summary
Introduction
Week 2 is about implantation and the endocrine signaling to block the normal menstrual cycle. We will also consider abnormal events that may occur in development during the second week. This involves abnormalities of implantation and conceptus development.
Note - Normal placentation will be covered in detail in a separate practical class.
Implantation Sites - Normal and Abnormal


Sites of normal and abnormal blastocyst implantation.
Site of most common (normal) implantation is the posterior wall of uterus (shown by X). Abnormal implantation: tubal pregnancies (shown by A-F), ovarian (H), and abdominal (G). Implantation at the internal os generates the clinical condition placenta previa, (resulting in bleeding or placental separation during pregnancy). Note that spontaneous abortion of blastocysts is quite common and studies of blastocysts that do not implant indicate chromosomal abnormalities in many of these embryos.
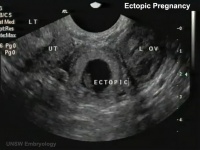
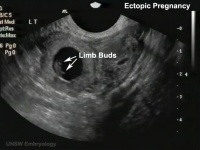
Abnormal implantation sites or Ectopic Pregnancy occurs if implantation is in uterine tube or outside the uterus.
- sites - external surface of uterus, ovary, bowel, gastrointestinal tract, mesentry, peritoneal wall
- If not spontaneous then, embryo has to be removed surgically
Tubal pregnancy - 94% of ectopic pregnancies
- if uterine epithelium is damaged (scarring, pelvic inflammatory disease)
- if zona pellucida is lost too early, allows premature tubal implantation
- embryo may develop through early stages, can erode through the uterine horn and reattach within the peritoneal cavity
| Tubal Ectopic | Bicornuate Uterus Ectopic | ||||||
|---|---|---|---|---|---|---|---|
|
|

|

|
|

|
- Links: ectopic pregnancy | ultrasound
Implantation Images Day 8 and 9

|
Overview of blastocyst implantation in uterine wall during the second week of development.
Identify the embryoblast and trophoblast layers of the conceptus. Carnegie Stage 4 (stages 1-23 describing key steps in embryonic development) represents the beginning of implantation.
The trophoblast layer divides initially into 2 layers; syncytiotrophoblast and cytotrophoblast. |
Placental Abnormalities

Placenta Accreta - Abnormal adherence, with absence of decidua basalis. The incidence of placenta accreta also significantly increases in women with previous cesarean section compared to those without a prior surgical delivery.
Placenta Increta - occurs when the placenta attaches deep into the uterine wall and penetrates into the uterine muscle, but does not penetrate the uterine serosa. Placenta increta accounts for approximately 15-17% of all cases.
Placenta Percreta - placental villi penetrate myometrium and through to uterine serosa.
Placenta Previa
 |
In this placenatal abnormality, the placenta overlies internal os at the cervix of the uterus, essentially covering the birth canal. This condition occurs in approximately 1 in 200 to 250 pregnancies.
In the third trimester and at term, abnormal bleeding can require cesarian delivery and can also lead to abruptio placenta. Ultrasound screening programs during 1st and early 2nd trimester pregnancies now include placental localization. Diagnosis can also be made by transvaginal ultrasound. |
Hydatidiform Mole
 |
A placental tumor with no embryo development.
Several forms of hydatidiform mole: partial mole, complete mole and persistent gestational trophoblastic tumor.
Many of these tumours arise from a haploid sperm fertilizing an egg without a female pronucleus (the alternative form, an embryo without sperm contribution, is called parthenogenesis). The tumour has a "grape-like" placental appearance without enclosed embryo formation. Following a first molar pregnancy, there is approximately a 1% risk of a second molar pregnancy.
|
Week 2 Interactive Component
| Attempt the Quiz - Week 2 | |
|---|---|

Here are a few simple Quiz questions that relate to Week 2 from the lecture and practical. See your Quiz Result - Answer all the questions, then click "submit" to complete. The page will reload and you can then reopen this table to see your result and feedback.
|
| Additional Information - Content shown under this heading is not part of the material covered in this class. It is provided for those students who would like to know about some concepts or current research in topics related to the current class page. |
Monoygotic Twinning
| Week | Week 1 (GA week 3) | Week 2 (GA week 4) | |||||||||||||
| Day | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 |
| Cell Number | 1 | 1 | 2 | 16 | 32 | 128 | bilaminar | ||||||||
| Event | Ovulation | Fertilization | First cell division | Morula | Early blastocyst | Late blastocyst
Hatching |
Implantation starts | X inactivation | |||||||

|

|

|

|
||||||||||||
| Monoygotic
Twin Type |
Diamniotic
Dichorionic |
Diamniotic
Monochorionic |
Monoamniotic
Monochorionic |
Conjoined | |||||||||||
Table based upon recent a recent twinning review.[1] Links: twinning
Pelvic Inflammatory Disease and Ectopic Pregnancy
Rates of pelvic inflammatory disease and ectopic pregnancy in Australia, 2009-2014[2]
- Calculated yearly PID and EP diagnosis rates in three states (Victoria, New South Wales, Queensland) for women aged 15-44 years using hospital admissions and emergency department (ED) attendance data, with population and live birth denominators. * Ectopic Pregnancy - in 2014 the rate of all admissions was 17.4 (95% CI 16.9 to 17.9) per 1000 live births and of all ED presentations was 15.6 (95% CI 15.1 to 16.1).
- Comparing 2014 with 2009, the rates of all EP admissions (aIRR 1.06, 95% CI 1.04 to 1.08) and rates in EDs (aIRR 1.24, 95% CI 1.18 to 1.31) were higher.
- Pelvic Inflammatory Disease and EP remain important causes of hospital admissions for female STI-associated complications. Hospital EDs care for more PID cases than inpatient departments, particularly for young women." Australian statistics | bacterial infection
Decidualization
Okada H, Tsuzuki T & Murata H. (2018). Decidualization of the human endometrium. Reprod. Med. Biol. , 17, 220-227. PMID: 30013421 DOI.
- ↑ Hall JG. (2003). Twinning. Lancet , 362, 735-43. PMID: 12957099 DOI.
- ↑ Goller JL, De Livera AM, Guy RJ, Low N, Donovan B, Law M, Kaldor JM, Fairley CK & Hocking JS. (2018). Rates of pelvic inflammatory disease and ectopic pregnancy in Australia, 2009-2014: ecological analysis of hospital data. Sex Transm Infect , , . PMID: 29720385 DOI.
Terms
- cytotrophoblast - The "cellular" trophoblast layer surrounding (forming a "shell") the early implanting conceptus. Beginning at uterine adplantation, proliferation and fusion of these cells is thought to form a second outer trophoblast layer, the syncytiotrophoblast. The cytotrophoblast layer contributes to formation of the placental villi, the functional component of the fetal placenta. (More? Placenta Development | Week 2)
- decidua basalis - The term given to the uterine endometrium at the site of implantation where signaling transforms the uterine stromal cells (fibroblast-like) into decidual cells. This forms the maternal component of the placenta, the decidualization process gradually spreads through the remainder of the uterus, forming the decidua parietalis. (More? Placenta Development | Week 2)
- ectopic implantation - (ectopic pregnancy, Greek, ektopos = out of place) Term referring to blastocyst implantation at (abnormal) sites other than within the body of the uterus (uterine body), this can result in an ectopic pregnancy. (More? Week 2)
- epiblast - (Greek, epi = above, upon) the layer (of the bilaminar embryo) that generates endoderm and mesoderm by migration of cells through the primitive streak. The remaing cells form ectoderm.(More? Week 2 | Week 3)
- hypoblast - The transient epithelium that forms during week 2 of human development that lines the blastoceol, and forms part of the bilaminar embryo (epiblast/hypoblast) from the inner cell mass. During trilaminar embryo development, the process of gastrulation replaces the hyoblast layer within the embryo with endoderm germ layer.(More? Week 2)
- myometrium - Uterus anatomy term describing the uterus wall (uterine wall) middle smooth muscle layer. This layer lies between the lining endometrium and the covering serosa (perimetrium). During pregnancy this layer increases in thickness, mainly by smooth muscle hypertrophy, and its contraction is required for childbirth and expulsion of the placenta. (More? Uterus Development | Birth
- syncytiotrophoblast - A multinucleated cell currently thought to form by the fusion of another trophoblast cell the cytotrophoblasts, within the trophoblast layer (shell) of the implanting conceptus. In early development, these cells mediate implantation of the conceptus into the uterine wall and secrete the hormone (human Chorionic Gonadotrophin, hCG) responsible for feedback maintainance of the corpus luteum (in maternal ovary) and therefore maintaining early pregnancy. (More? Trophoblast | Week 2 | Placenta Development | human Chorionic Gonadotrophin)
References
BGDA: Lecture 1 | Lecture 2 | Practical 3 | Practical 6 | Practical 12 | Lecture Neural | Practical 14 | Histology Support - Female | Male | Tutorial
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2026, July 4) Embryology BGDA Practical 3 - Week 2 Summary. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/BGDA_Practical_3_-_Week_2_Summary
- © Dr Mark Hill 2026, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G