Musculoskeletal System - Skull Development: Difference between revisions
mNo edit summary |
mNo edit summary |
||
| (10 intermediate revisions by the same user not shown) | |||
| Line 20: | Line 20: | ||
[[:Category:Skull|Category:Skull]] | {{head}} | {{neural crest}} | {{palate}} | {{temporomandibular joint}} | {{joint}} | [[:Category:Skull|Category:Skull]] | {{head}} | {{neural crest}} | {{palate}} | {{temporomandibular joint}} | {{joint}} | ||
{| class="wikitable mw-collapsible mw-collapsed" | {| class="wikitable mw-collapsible mw-collapsed" | ||
! [[ | ! [[Historic Embryology Papers|Historic Embryology]] - Skull | ||
|- | |- | ||
| [[Book_-_Manual_of_Human_Embryology_11E|1910 Textbook Skull]] | [[Book_-_Manual_of_Human_Embryology_-_Figures#Skull|1910 Textbook Skull Images]] | [[Paper - Description of a | | [[Book_-_Manual_of_Human_Embryology_11E|1910 Textbook Skull]] | [[Book_-_Manual_of_Human_Embryology_-_Figures#Skull|1910 Textbook Skull Images]] | [[Paper - Description of a reconstruction of the head of a thirty-millimetre embryo (1910)|1910 30mm Embryo Skull]] | [[Book_-_Contributions_to_Embryology_Carnegie_Institution_No.24|1921 Human Brain Vascular]] | [[Book_-_Contributions_to_Embryology_Carnegie_Institution_No.71|1923 Head Subcutaneous Plexus]] | [[Book_-_Contributions_to_Embryology_Carnegie_Institution_No.39|1919 21mm Embryo Skull]] | [[Book_-_Contributions_to_Embryology_Carnegie_Institution_No.55|1920 Human Embryo Head Size]] | [[Book_-_Contributions_to_Embryology_Carnegie_Institution_No.48|1921 43 mm Fetal Skull]] | [[Paper_-_The_Monotreme_Skull_-_A_Contribution_to_Mammalian_Morphogenesis|1915 The Monotreme Skull]] | [[Embryology_History#Historic_Disclaimer|Historic Disclaimer]] | ||
|} | |} | ||
<br> | |||
{{Musculoskeletal Links}} | |||
== Some Recent Findings == | == Some Recent Findings == | ||
[[File:Vesalius_Skull.jpg|thumb|Historic images of the skull by Vesalius]] | [[File:Vesalius_Skull.jpg|thumb|Historic images of the skull by Vesalius]] | ||
| Line 33: | Line 33: | ||
|-bgcolor="F5FAFF" | |-bgcolor="F5FAFF" | ||
| | | | ||
* '''Candidate positive targets of LHX6 and LHX8 transcription factors in the developing upper jaw'''{{#pmid:34861428|PMID34861428}} "Craniofacial development is controlled by a large number of genes, which interact with one another to form a complex gene regulatory network (GRN). Key components of GRN are signaling molecules and transcription factors. Therefore, identifying targets of core transcription factors is an important part of the overall efforts toward building a comprehensive and accurate model of GRN. LHX6 and LHX8 are transcription factors expressed in the oral mesenchyme of the first pharyngeal arch (PA1), and they are crucial regulators of palate and tooth development. Previously, we performed genome-wide transcriptional profiling and chromatin immunoprecipitation to identify target genes of LHX6 and LHX8 in PA1, and described a set of genes repressed by LHX. However, there has not been any discussion of the genes positively regulated by LHX6 and LHX8. In this paper, we revisited the above datasets to identify candidate positive targets of LHX in PA1. Focusing on those with known connections to craniofacial development, we performed RNA in situ hybridization to confirm the changes in expression in Lhx6;Lhx8 mutant. We also confirmed the binding of LHX6 to several putative enhancers near the candidate target genes. Together, we have uncovered novel connections between Lhx and other important regulators of craniofacial development, including Eya1, Barx1, Rspo2, Rspo3, and Wnt11." | |||
* '''Association between the developing sphenoid and adult morphology: A study using sagittal sections of the skull base from human embryos and fetuses'''{{#pmid:34268732|PMID34268732}} "The developing sphenoid is regarded as a median cartilage mass (basisphenoid [BS]) with three cartilaginous processes (orbitosphenoid [OS], ala temporalis [AT], and alar process [AP]). The relationships of this initial configuration with the adult morphology are difficult to determine because of extensive membranous ossification along the cartilaginous elements. The purpose of this study was therefore to evaluate the anatomical connections between each element of the fetal sphenoid and adult morphology. Sagittal sections from 25 embryos and fetuses of gestational age 6-34 weeks and crown-rump length 12-295 mm were therefore examined and compared with horizontal and frontal sections from the other 25 late-term fetuses (217-340 mm). The OS was identified as a set of three mutually attached cartilage bars in early fetuses. At all stages, the OS-post was continuous with the anterolateral part of the BS. The BS included the notochord and Rathke's pouch remnant in embryos and early fetuses. The dorsum sellae was absent from embryos, but it protruded from the BS in early fetuses before a fossa for the hypophysis became evident. Although not higher than the hypophysis at midterm, the dorsum sellae elongated superiorly after gestational age 25 weeks. In early fetuses, the AP was located on the side immediately anterior to the otic capsule. The AT developed on the side immediately posterior to the extraocular rectus muscles. At late term, the greater wing was formed by membranous bones from the AT and AP. The AT and AP formed a complex bridge between the BS and the greater wing. A small cartilage, future medial pterygoid process (PTmed) was located inferior to the AT in early fetuses. At midterm, one endochondral bone and multiple membranous bones formed the PTmed. The lateral pterygoid process (PTlat) was formed by a single membranous bone plate. Therefore, we connected fetal elements and the adult morphology as follows. (1) Derivative of the OS makes not only the lesser wing but also the anterior margin of the body of the sphenoid. (2) Derivatives of the BS are the body of the sphenoid including the sella turcica and the dorsum sellae. (3) Most of the greater wing including the foramen rotundum and the foramen oval originate from the AT and AP and multiple membranous bones. (4) The PTmed originate from endochondral bones and multiple membranous bones, while the PTlat derive from a single membranous bone." | |||
* '''Review - A comprehensive review of the anterior fontanelle: embryology, anatomy, and clinical considerations.'''{{#pmid:28396968|PMID28396968}} "Fontanelles are a regular feature of infant development in which two segments of bone remain separated, leaving an area of fibrous membrane or a "soft spot" that acts to accommodate growth of the brain without compression by the skull. Of the six fontanelles in the human skull, the anterior fontanelle, located between the frontal and parietal bones, serves as an important anatomical diagnostic tool in the assessment of impairments of the skull and brain and allows access to the brain and ventricles in the infant. The diagnostic value of the anterior fontanelle, through observation of its shape, size, and palpability, makes the area of significant clinical value." | * '''Review - A comprehensive review of the anterior fontanelle: embryology, anatomy, and clinical considerations.'''{{#pmid:28396968|PMID28396968}} "Fontanelles are a regular feature of infant development in which two segments of bone remain separated, leaving an area of fibrous membrane or a "soft spot" that acts to accommodate growth of the brain without compression by the skull. Of the six fontanelles in the human skull, the anterior fontanelle, located between the frontal and parietal bones, serves as an important anatomical diagnostic tool in the assessment of impairments of the skull and brain and allows access to the brain and ventricles in the infant. The diagnostic value of the anterior fontanelle, through observation of its shape, size, and palpability, makes the area of significant clinical value." | ||
|} | |} | ||
{| class="wikitable mw-collapsible mw-collapsed" | {| class="wikitable mw-collapsible mw-collapsed" | ||
! More recent papers | ! More recent papers | ||
| Line 99: | Line 103: | ||
Meckel's cartilage, located within the first pharyngeal arch mandibular prominence, forms a cartilage "template" besides which the {{mandible}} bone develops by the process of intramembranous ossification. It is important to note that this cartilage template does not ossify (endochondral ossification) but provides a transient structure where the mandible will form, and later degenerates. | Meckel's cartilage, located within the first pharyngeal arch mandibular prominence, forms a cartilage "template" besides which the {{mandible}} bone develops by the process of intramembranous ossification. It is important to note that this cartilage template does not ossify (endochondral ossification) but provides a transient structure where the mandible will form, and later degenerates. | ||
See also the 1957 historic paper on temporomandibular joint development.<ref name=Moffatt1957>{{Ref-Moffatt1957}}</ref> | See also the 1957 historic paper on {{temporomandibular joint}} development.<ref name=Moffatt1957>{{Ref-Moffatt1957}}</ref> | ||
===Embryonic and Fetal Mandible=== | ===Embryonic and Fetal Mandible=== | ||
| Line 251: | Line 255: | ||
=== Craniosynostosis === | === Craniosynostosis === | ||
Attenuation of signaling pathways stimulated by pathologically activated FGF-receptor 2 mutants prevents craniosynostosis.{{#pmid:17132737|PMID17132737}} "Craniosynostosis, the fusion of one or more of the sutures of the skull vault before the brain completes its growth, is a common (1 in 2,500 births) craniofacial abnormality, approximately 20% of which occurrences are caused by gain-of-function mutations in FGF receptors (FGFRs). ...These experiments show that attenuation of FGFR signaling by pharmacological intervention could be applied for the treatment of craniosynostosis or other severe bone disorders caused by mutations in FGFRs that currently have no treatment." | Attenuation of signaling pathways stimulated by pathologically activated FGF-receptor 2 mutants prevents craniosynostosis.{{#pmid:17132737|PMID17132737}} "Craniosynostosis, the fusion of one or more of the sutures of the skull vault before the brain completes its growth, is a common (1 in 2,500 births) craniofacial abnormality, approximately 20% of which occurrences are caused by gain-of-function mutations in FGF receptors (FGFRs). ...These experiments show that attenuation of FGFR signaling by pharmacological intervention could be applied for the treatment of craniosynostosis or other severe bone disorders caused by mutations in FGFRs that currently have no treatment." | ||
See also {{Crouzon syndrome}}. | |||
====Dolichocephaly and scaphocephaly==== | ====Dolichocephaly and scaphocephaly==== | ||
| Line 310: | Line 316: | ||
:'''Links:''' [https://www.omim.org/entry/176943 OMIM - FGFR2] | |||
== Skull Histology == | == Skull Histology == | ||
A histological image of a skull bone formation by Intramembranous ossification. | A histological image of a skull bone formation by Intramembranous ossification. | ||
| Line 324: | Line 331: | ||
===Reviews=== | ===Reviews=== | ||
{{#pmid:35220463}} | |||
{{#pmid:1522265}} | {{#pmid:1522265}} | ||
| Line 352: | Line 361: | ||
</gallery> | </gallery> | ||
===Historic | ===Historic=== | ||
[[Embryology_History|Historic Embryology]] | [[Embryology_History|Historic Embryology]] | ||
{| class="wikitable mw-collapsible mw-collapsed" | {| class="wikitable mw-collapsible mw-collapsed" | ||
! [[Book_-_Manual_of_Human_Embryology_11E|1910 Development of the Skeleton]] | ! Johns Hopkins Fetal Skull Collection (1918–1951) | ||
|- | |||
|{{Johns Hopkins Fetal Skull Collection simplified table}} | |||
|} | |||
{| class="wikitable mw-collapsible mw-collapsed" | |||
! [[Book_-_Manual_of_Human_Embryology_11E|1910 Development of the Skeleton]] | |||
|- | |- | ||
| | | | ||
| Line 380: | Line 395: | ||
|} | |} | ||
{| class="wikitable mw-collapsible mw-collapsed" | {| class="wikitable mw-collapsible mw-collapsed" | ||
! [[Paper - The skull of a human fetus of 40 mm 1|1914 Human Fetus 40 mm Skull]] | ! [[Paper - The skull of a human fetus of 40 mm 1|1914 Human Fetus 40 mm Skull]] | ||
|- | |- | ||
| | | | ||
| Line 400: | Line 415: | ||
|} | |} | ||
{| class="wikitable mw-collapsible mw-collapsed" | {| class="wikitable mw-collapsible mw-collapsed" | ||
! [[Book_-_Contributions_to_Embryology_Carnegie_Institution_No.48|1921 43 mm Fetal Skull]] | ! [[Book_-_Contributions_to_Embryology_Carnegie_Institution_No.48|1921 43 mm Fetal Skull]] | ||
|- | |- | ||
| | | | ||
| Line 423: | Line 438: | ||
|} | |} | ||
{| class="wikitable mw-collapsible mw-collapsed" | {| class="wikitable mw-collapsible mw-collapsed" | ||
! [[Anatomy_of_the_Human_Body_by_Henry_Gray#1_Development|1918 Gray's Anatomy]] | ! [[Anatomy_of_the_Human_Body_by_Henry_Gray#1_Development|1918 Gray's Anatomy]] | ||
|- | |- | ||
| | | | ||
| Line 443: | Line 458: | ||
* '''intramembranous ossification''' - bone formation from a membrane where no pre-existing cartilage is found, such as the calvarial vault component. | * '''intramembranous ossification''' - bone formation from a membrane where no pre-existing cartilage is found, such as the calvarial vault component. | ||
* '''neurocranium''' - the portion of the skull that surrounds the brain. Ossification of bones in cranial base (endochondral) and vault (intramembranous). | * '''neurocranium''' - the portion of the skull that surrounds the brain. Ossification of bones in cranial base (endochondral) and vault (intramembranous). | ||
* '''opisthion''' - anatomical region located on the occipital bone, located at the midpoint of the posterior margin of the foramen magnum. | * '''opisthion''' - anatomical region located on the occipital bone, located at the midpoint of the posterior margin of the foramen magnum. | ||
* '''posterior fontanel''' - developing skull region that closes by about 3 months postnatally. | * '''posterior fontanel''' - developing skull region that closes by about 3 months postnatally. | ||
* '''primary craniosynostosis''' - an intrinsic defect in a suture. | * '''primary craniosynostosis''' - an intrinsic defect in a suture. | ||
* '''secondary craniosynostosis''' - premature closure of normal sutures due to systemic and metabolic (hyperthyroidism, hypercalcemia, hypophosphatasia, vitamin D deficiency, renal osteodystrophy, Hurler's Syndrome, sickle cell disease and thalassemia) and those that can affect brain growth. | * '''secondary craniosynostosis''' - premature closure of normal sutures due to systemic and metabolic (hyperthyroidism, hypercalcemia, hypophosphatasia, vitamin D deficiency, renal osteodystrophy, Hurler's Syndrome, sickle cell disease and thalassemia) and those that can affect brain growth. | ||
* '''simple craniosynostosis''' - premature fusion involving only one suture. | * '''simple craniosynostosis''' - premature fusion involving only one suture. | ||
* '''synostosis''' - premature fusion. | * '''synostosis''' - premature fusion. | ||
* '''viscerocranium''' - facial skeleton and some anterior neck structures. | * '''viscerocranium''' - facial skeleton and some anterior neck structures. | ||
Latest revision as of 04:14, 5 July 2022
| Embryology - 21 May 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Introduction
The skull is a unique skeletal structure in several ways: embryonic cellular origin (neural crest and mesoderm), form of ossification (intramembranous and ) and flexibility (fibrous sutures). The cranial vault (which encloses the brain) bones are formed by intramembranous ossification. While the bones that form the base of the skull are formed by endochondral ossification.
Ossification
- endochondral ossification - ethmoid, basi sphenoid, basi occipital, petrous temporal
- intramembranous ossification - facial skeleton (nasals, maxillae, premaxillae, zygomatic, mandible) and cranial vault (frontal, parietal, and squamous temporal)
The bones enclosing the brain have large flexible fibrous joints (sutures) which allow firstly the head to pass through the birth canal and secondly postnatal brain growth. (See also notes on Head Development) In humans, ossification within the skull continues postnatally, through puberty until mid 20's and in old age the sutures separating the vault plates are often completely ossified.
In the entire skeleton, early ossification occurs in the jaw and at the ends of long bones (More? see movie developing mouse). Osteoblasts manufacture bone and are derived from ectomesenchymal in origin. (More? see lineage below). Flexible fibrous sutures allow growth of the brain to be accomodated by calvarial plate growth. Recent studies have show that noggin (a BMP antagonist) is involved in closure of these sutures.
Developmentally and clinically there are several abnormalities associated with skull growth and palate development. These abnormalities can furthermore impact on other systems such as neural, sensory, respiratory and nutritional functions.
Category:Skull | head | neural crest | palate | temporomandibular joint | joint
Some Recent Findings

|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Skull Embryology | Skull Development | Mandible Development |
| Older papers |
|---|
| These papers originally appeared in the Some Recent Findings table, but as that list grew in length have now been shuffled down to this collapsible table.
See also the Discussion Page for other references listed by year and References on this current page.
|
Fetal Skull
The Images below show the combined endochondral and intramembranous ossification that is occurring in early fetal development (week 12).
In the first 2 images the bone cartilage is shown in blue and the new bone in red.
Note the difference in appearance between the upper and lower jaw (maxilla and mandible), the currently cartilage base of the skull (chondrocranium) and the cranial vault (neurocranium).

Fetal head lateral view |

Fetal head medial view |

Fetal head section |
This mid-line section through the fetal head shows features of the developing skull and the brain, face and mouth.
|
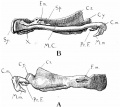
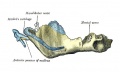
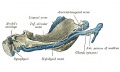
Mandible Development

Meckel's cartilage, located within the first pharyngeal arch mandibular prominence, forms a cartilage "template" besides which the mandible bone develops by the process of intramembranous ossification. It is important to note that this cartilage template does not ossify (endochondral ossification) but provides a transient structure where the mandible will form, and later degenerates.
See also the 1957 historic paper on temporomandibular joint development.[9]
Embryonic and Fetal Mandible

embryo 18 mm

embryo 24 mm

Embryo 24 mm (outer aspect, about Carnegie stage 22)

Embryo 24 mm (inner aspect, about Carnegie stage 22)

embryo 28 mm
fetus 43 mm

fetus 65 mm

fetus 55 mm

fetus 95 mm
fetus 95 mm (outer aspect, about Fetal week 12, GA week 14)
fetus 95 mm (inner aspectt, about Fetal week 12, GA week 14)

human 18-24-95 mm











Birth to Adult Mandible

Birth

Childhood

Adult

Old Age




|

Animated GIF |
- Mandible Development: Week 8 outer view | Week 8 inner view | Week 12 outer view | Week 12 inner view | Week 12 Head outer view | Week 12 Head inner view | Birth | Childhood | Adult | Old Age | Small Animation | Large Animation | Muscle Attachments | Mandible Ossification | 1909 Mandible | embryo 18 mm | embryo 24 mm | embryo 28 mm | fetus 43 mm | fetus 65 mm | fetus 55 mm | fetus 95 mm | human 18-24-95 mm | Skull Development | Head Development
Neurocranium
Frontal bone
- neural crest origin
- requires Msx1 and Dlx5[10]
Parietal bone
- paraxial mesoderm origin
Skull Views

|

|

|

|
| anterior view | superior view | lateral view | lateral view |
| showing anterior fontenelle, sutures, mandible | showing anterior fontenelle, sutures | showing suture, mandible | newborn skull |
Skull Fontanels and Sutures

The bones enclosing the brain have large flexible fibrous joints (sutures) which allow firstly the head to compress and pass through the birth canal and secondly to postnatally expand for brain growth. (More? Molecular Skull Sutures) These sutures gradually fuse at different times postnatally, firstly the metopic suture in infancy and the others much later. Abnormal fusion (synostosis) of any of the sutures will lead to a number of different skull defects, leading to disruption of brain development. (More? Abnormal Synostosis) In old age all these sutures are generally completely fused and ossified.
Skull Fontanels
The newborn skull has 6 fontanels (fontanelles) the most obvious are the anterior and posterior fontanels that close at different times postnatally.
|

Newborn Skull Fontanels (CT, vertex view) |
At the molecular level, accelerated suture intramembranous ossification can be mediated through a dual role of β-catenin in both the expansion of osteoprogenitors and the maturation of osteoblasts.[11] These researchers also show that disruption of Axin2/β-catenin signaling alters the regulation of the downstream transcription target, cyclin D1, in the canonical Wnt pathway.[12]
Computed Tomography Views

Skull CT Vertex, later and basal views.[13] |
Sutures and Fontanels
|
coronal suture

lambdoid suture

metopic suture begins at nose and runs superiorly to meet sagittal suture and fuses during infancy (fusion beginning at 3 months and completes by 6 to 8 months of age) before all other cranial sutures.
sagittal suture
Cranial Base Synchondroses
In the base of the skull there can also be found a number of synchondrosis, "cartilage sutures", that are the last to close and have a role in the ongoing growth of the postnatal skull. Synchondrosis is a type of cartilaginous joint in which the cartilage is usually converted into bone before adult life. It has been compared in appearance to a long bone growth plate, but is bipolar rather than unipolar in structure.
These sutures also lost at different times in postnatal development:
- Inter-sphenoidal – around birth
- Spheno-ethmoidal – 6-7 yrs
- Spheno-occipital – 12-15 yrs
Fetal Head Growth


Abnormalities
There are several skull deformities caused by premature fusion (synostosis) of different developing skull sutures. Suture abnormalities are classified as either "simple" (only one suture involved) or "compound" (two or more sutures involved). Failure of neural (brain) development may also result in acrocephaly of the skull.
 |
* craniosynostosis premature cranial suture fusion, results in an abnormal skull shape, blindness and mental retardation.
|
Craniosynostosis
Attenuation of signaling pathways stimulated by pathologically activated FGF-receptor 2 mutants prevents craniosynostosis.[8] "Craniosynostosis, the fusion of one or more of the sutures of the skull vault before the brain completes its growth, is a common (1 in 2,500 births) craniofacial abnormality, approximately 20% of which occurrences are caused by gain-of-function mutations in FGF receptors (FGFRs). ...These experiments show that attenuation of FGFR signaling by pharmacological intervention could be applied for the treatment of craniosynostosis or other severe bone disorders caused by mutations in FGFRs that currently have no treatment."
See also Crouzon syndrome.
Dolichocephaly and scaphocephaly

|
| Dolichocephaly and scaphocephaly
(premature fusion of the sagittal suture) |
Brachycephaly and anterior plagiocephaly
(Greek, brakhu = short) (Greek plagios = oblique)
- brachycephaly - premature bicoronal fusion
- anterior plagiocephaly - unicoronal fusion
Leads to a restriction of anterior-posterior calvarial growth and relatively unaffected biparietal growth.


Skull Turricephaly

Skull Trigonocephaly

(Greek, trigonos = three angles) This abnormality results from the premature fusion of the metopic suture occurring before 6 months (3-9 months) of age.
Skull Oxycephaly

Images show oxycephaly from severe sagittal and coronal synostoses (arrowheads).
Craniofrontonasal Syndrome
Craniofrontonasal syndrome (CFNS) is a human X-linked developmental disorder caused by a mutation in ephrin-B1 affecting mainly females. Characterised by abnormal development of cranial and nasal bones, craniosynostosis (premature coronal suture fusion), and other extracranial anomalies (limb polydactyly and syndactyly).

|
(a) Facial view showing marked hypertelorism, divergent squint, and central nasal groove (subject age, 1 year).
|
| Craniofrontonasal syndrome[14] | Links: OMIM - Craniofrontonasal Syndrome |
Crouzon syndrome
Crouzon syndrome (craniofacial dysostosis) rare genetic disorder also characterized by premature closure of cranial sutures. Cranial and facial malformations vary, ranging from mild to potentially severe, including among members of the same family (autosomal dominant). The syndrome is caused by mutations in one of the FGFR genes, most commonly FGFR2.
- Links: OMIM - FGFR2
Skull Histology
A histological image of a skull bone formation by Intramembranous ossification.

Adult Skull
| Adult Skull MRI | Links: | Skull Development | - MRI | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
References
- ↑ Cesario J, Ha S, Kim J, Kataria N & Jeong J. (2021). Candidate positive targets of LHX6 and LHX8 transcription factors in the developing upper jaw. Gene Expr Patterns , 43, 119227. PMID: 34861428 DOI.
- ↑ Yamamoto M, Jin ZW, Hayashi S, Rodríguez-Vázquez JF, Murakami G & Abe S. (2021). Association between the developing sphenoid and adult morphology: A study using sagittal sections of the skull base from human embryos and fetuses. J Anat , 239, 1300-1317. PMID: 34268732 DOI.
- ↑ D'Antoni AV, Donaldson OI, Schmidt C, Macchi V, De Caro R, Oskouian RJ, Loukas M & Shane Tubbs R. (2017). A comprehensive review of the anterior fontanelle: embryology, anatomy, and clinical considerations. Childs Nerv Syst , 33, 909-914. PMID: 28396968 DOI.
- ↑ Homayounfar N, Park SS, Afsharinejad Z, Bammler TK, MacDonald JW, Farin FM, Mecham BH & Cunningham ML. (2015). Transcriptional analysis of human cranial compartments with different embryonic origins. Arch. Oral Biol. , 60, 1450-60. PMID: 26188427 DOI.
- ↑ Clendenning DE & Mortlock DP. (2012). The BMP ligand Gdf6 prevents differentiation of coronal suture mesenchyme in early cranial development. PLoS ONE , 7, e36789. PMID: 22693558 DOI.
- ↑ Haberland M, Mokalled MH, Montgomery RL & Olson EN. (2009). Epigenetic control of skull morphogenesis by histone deacetylase 8. Genes Dev. , 23, 1625-30. PMID: 19605684 DOI.
- ↑ Sisson BE & Topczewski J. (2009). Expression of five frizzleds during zebrafish craniofacial development. Gene Expr. Patterns , 9, 520-7. PMID: 19595791 DOI.
- ↑ 8.0 8.1 Eswarakumar VP, Ozcan F, Lew ED, Bae JH, Tomé F, Booth CJ, Adams DJ, Lax I & Schlessinger J. (2006). Attenuation of signaling pathways stimulated by pathologically activated FGF-receptor 2 mutants prevents craniosynostosis. Proc. Natl. Acad. Sci. U.S.A. , 103, 18603-8. PMID: 17132737 DOI.
- ↑ Moffatt BC. The prenatal development of the human temporomandibular joint. (1957) Carnegie Instn. Wash. Publ. 611, Contrib. Embryol., 36: .
- ↑ Chung IH, Han J, Iwata J & Chai Y. (2010). Msx1 and Dlx5 function synergistically to regulate frontal bone development. Genesis , 48, 645-55. PMID: 20824629 DOI.
- ↑ Liu B, Yu HM & Hsu W. (2007). Craniosynostosis caused by Axin2 deficiency is mediated through distinct functions of beta-catenin in proliferation and differentiation. Dev. Biol. , 301, 298-308. PMID: 17113065 DOI.
- ↑ Mirando AJ, Maruyama T, Fu J, Yu HM & Hsu W. (2010). β-catenin/cyclin D1 mediated development of suture mesenchyme in calvarial morphogenesis. BMC Dev. Biol. , 10, 116. PMID: 21108844 DOI.
- ↑ 13.0 13.1 Khanna PC, Thapa MM, Iyer RS & Prasad SS. (2011). Pictorial essay: The many faces of craniosynostosis. Indian J Radiol Imaging , 21, 49-56. PMID: 21431034 DOI.
- ↑ Twigg SR, Kan R, Babbs C, Bochukova EG, Robertson SP, Wall SA, Morriss-Kay GM & Wilkie AO. (2004). Mutations of ephrin-B1 (EFNB1), a marker of tissue boundary formation, cause craniofrontonasal syndrome. Proc. Natl. Acad. Sci. U.S.A. , 101, 8652-7. PMID: 15166289 DOI.
Reviews
Liao J, Huang Y, Wang Q, Chen S, Zhang C, Wang D, Lv Z, Zhang X, Wu M & Chen G. (2022). Gene regulatory network from cranial neural crest cells to osteoblast differentiation and calvarial bone development. Cell Mol Life Sci , 79, 158. PMID: 35220463 DOI.
Shah M, Ross JS, VanDyke C, Rudick RA, Goodkin DE, Obuchowski N & Modic MT. (1992). Volume T1-weighted gradient echo MRI in multiple sclerosis patients. J Comput Assist Tomogr , 16, 731-6. PMID: 1522265
Stelnicki EJ, Mooney MP, Losken HW, Zoldos J, Burrows AM, Kapucu R & Siegel MI. (1997). Ultrasonic prenatal diagnosis of coronal suture synostosis. J Craniofac Surg , 8, 252-8; discussion 259-61. PMID: 9482048
Ocampo RV & Persing JA. (1994). Sagittal synostosis. Clin Plast Surg , 21, 563-74. PMID: 7813156
Vander Kolk CA & Carson BS. (1994). Lambdoid synostosis. Clin Plast Surg , 21, 575-84. PMID: 7813157
Cohen MM. (1993). Sutural biology and the correlates of craniosynostosis. Am. J. Med. Genet. , 47, 581-616. PMID: 8266985 DOI.
Articles
Weinzweig J, Kirschner RE, Farley A, Reiss P, Hunter J, Whitaker LA & Bartlett SP. (2003). Metopic synostosis: Defining the temporal sequence of normal suture fusion and differentiating it from synostosis on the basis of computed tomography images. Plast. Reconstr. Surg. , 112, 1211-8. PMID: 14504503 DOI.
Search PubMed
Search July 2010 "Skull Development" All (15473) Review (1231) Free Full Text (1634)
Search Pubmed: Skull Development
Additional Images

Adult axial skeletonon

Endochondral bone

Skull - osteoblast lineage model

Skull vault defect and midface hypoplasia




Historic
| Johns Hopkins Fetal Skull Collection (1918–1951) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1910 Development of the Skeleton |
|---|
|
















| 1914 Human Fetus 40 mm Skull |
|---|
Macklin CC. The skull of a human fetus of 40 mm 1. (1914) Amer. J Anat. 16(3): 317-386. Macklin CC. The skull of a human fetus of 40 mm 2. (1914) Amer. J Anat. 16(3): 387-426. |











| 1921 43 mm Fetal Skull |
|---|
|
















| 1918 Gray's Anatomy |
|---|
|




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Terms
- anterior fontanel - developing skull region that closes by about 20 months postnatally.
- basion - anatomical region on the basiocciput located at the midpoint between the anterior margin and posterior margin (opisthion) of the foramen magnum.
- compound craniosynostosis premature suture fusion involving two or more sutures.
- craniosynostosis - (craniostenosis) the premature fusion of cranial sutures.
- dermatocranium - (membranous) skull calvarial vault develops from intramembranous ossification.
- harlequin eye - a term used to describe the prominent bilateral elliptical orbits of the skull seen in brachycephaly.
- endochondral ossification - bone formation from a pre-existing cartilage template, such as the chondrocranium.
- intramembranous ossification - bone formation from a membrane where no pre-existing cartilage is found, such as the calvarial vault component.
- neurocranium - the portion of the skull that surrounds the brain. Ossification of bones in cranial base (endochondral) and vault (intramembranous).
- opisthion - anatomical region located on the occipital bone, located at the midpoint of the posterior margin of the foramen magnum.
- posterior fontanel - developing skull region that closes by about 3 months postnatally.
- primary craniosynostosis - an intrinsic defect in a suture.
- secondary craniosynostosis - premature closure of normal sutures due to systemic and metabolic (hyperthyroidism, hypercalcemia, hypophosphatasia, vitamin D deficiency, renal osteodystrophy, Hurler's Syndrome, sickle cell disease and thalassemia) and those that can affect brain growth.
- simple craniosynostosis - premature fusion involving only one suture.
- synostosis - premature fusion.
- viscerocranium - facial skeleton and some anterior neck structures.
External Links
External Links Notice - The dynamic nature of the internet may mean that some of these listed links may no longer function. If the link no longer works search the web with the link text or name. Links to any external commercial sites are provided for information purposes only and should never be considered an endorsement. UNSW Embryology is provided as an educational resource with no clinical information or commercial affiliation.
- PubMed Health Craniosynostosis
- Johns Hopkins Fetal Skull Collection (1918–1951) - collection was begun by Adolph Hans Schultz (1891–1976) - fetal, stillbirths, newborns, and infants up to approximately one year of age. Collection of 112 specimens was transferred to the Cleveland Museum of Natural History on a permanent loan in 1973.
| Johns Hopkins Fetal Skull Collection (1918–1951) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, May 21) Embryology Musculoskeletal System - Skull Development. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Musculoskeletal_System_-_Skull_Development
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G