Abnormal Development - Fetal Growth Restriction
| Embryology - 30 Apr 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Introduction

The term "Fetal Growth Restriction" (FGR) or intrauterine growth restriction (IUGR) are used to describe when the fetus does not reach full growth potential. This is usually determined by clinical sonography calculations of fetal weight, fetal size, or symmetry.
The fetal period (weeks 9 to 37) is about four times the length of the embryonic period and the clinical term may not relate directly to just the "fetal period", that is a time of extensive growth in size and mass as well as ongoing differentiation of organ systems established in the embryonic period. Clinically this period is generally described as the Second Trimester and Third Trimester. Many of the critical measurements of growth are now carried out by ultrasound and measured at birth including the Birth-Weight.
| Fetal Links: fetal | Week 10 | Week 12 | second trimester | third trimester | fetal neural | Fetal Blood Sampling | fetal growth restriction | birth | birth weight | preterm birth | Developmental Origins of Health and Disease | macrosomia | BGD Practical | Medicine Lecture | Science Lecture | Lecture Movie | Category:Human Fetus | Category:Fetal | |||
|
- Fetal Graphs: Crown-Rump Length (CRL) | Third trimester CRL | Head Circumference | Head Circumference 2nd Trimester | Liver Weight | Pancreas Weight | Thymus Weight | Small Intestine Length | Large Intestine Length | Length and Weight Changes | Fetal Development
Some Recent Findings

|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Fetal Growth Restriction <pubmed limit=5>Fetal Growth Restriction</pubmed> |
Reading
|
|

Second Trimester

- Second Trimester
- Week 12 - CRL 85 mm, femur length 15 mm, biparietal diameter 25 mm.
Begin by working through the features present in the early 10 week female fetus. Then look in detail at the head development in a 12 week fetus.


|

|

|

|
Then look in detail at the head development in a 12 week fetus showing both forms of ossification in the skull.

|

|

|
Fetal Head Growth
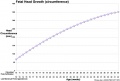
Second and third trimesters
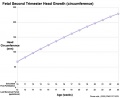
Second trimester


Third Trimester


{kind=link}
{kind=link}
{kind=link}
{kind=link}

- Vibration acoustically of maternal abdominal wall induces startle respone in fetus.
- Month 7 - respiratory bronchioles proliferate and end in alveolar ducts and sacs.
- Week 37 to 38 Birth.
- Links: Third Trimester
References
Journals
Reviews
<pubmed></pubmed> <pubmed></pubmed> <pubmed>22990459</pubmed> <pubmed>22696366</pubmed> <pubmed>22526452</pubmed> <pubmed></pubmed> <pubmed></pubmed>
Articles
<pubmed>23599816</pubmed> <pubmed></pubmed> <pubmed></pubmed>
Search PubMed
Search Pubmed: Fetal Growth Restriction
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, April 30) Embryology Abnormal Development - Fetal Growth Restriction. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Abnormal_Development_-_Fetal_Growth_Restriction
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G