Tongue Development
Introduction

The tongue's embryonic orgin is derived from all pharyngeal arches contributing different components. As the tongue ((Latin, lingua; Greek, glossa) develops "inside" the floor of the oral cavity, it is not readily visible in the external views of the embryonic (Carnegie) stages of development. Tongue muscle cells originate from somites, while muscles of mastication derive from the unsegmented somitomeres. This current page gives a brief overview of early tongue development.
The dorsal tongue is covered by a stratified squamous epithelium, with numerous papillae and taste buds. There are also 8 to 12 circumvallate papillae arranged in an inverted V-shape towards the base of the tongue. These notes cover development of the muscular tongue, not the sense of taste.
| Taste Links: Introduction | Student project | Tongue Development | Category:Taste | ||
|
| Gastrointestinal Tract | Category:Tongue
Some Recent Findings
|
- Bone morphogenetic protein-2 functions as a negative regulator in the differentiation of myoblasts, but not as an inducer for the formations of cartilage and bone in mouse embryonic tongue[2] "In vitro studies using the myogenic cell line C2C12 demonstrate that bone morphogenetic protein-2 (BMP-2) converts the developmental pathway of C2C12 from a myogenic cell lineage to an osteoblastic cell lineage. Further, in vivo studies using null mutation mice demonstrate that BMPs inhibit the specification of the developmental fate of myogenic progenitor cells. ...BMP-2 functions as a negative regulator for the final differentiation of tongue myoblasts, but not as an inducer for the formation of cartilage and bone in cultured tongue, probably because the genes related to myogenesis are in an activation mode, while the genes related to chondrogenesis and osteogenesis are in a silencing mode."
Pharyngeal Arch Contributions
The tongue has contributions from all pharyngeal arches which changes with time. The tongue initially begins as swelling rostral to foramen cecum, the median tongue bud.
| width=348px|height=440px|controller=true|autoplay=false</qt> |
Animation shows the sequence of development of the tongue. The different colours represents the relative contribution from each pharyngeal arch.
|
Week 4


- Links: Carnegie stage 13 | Week 4
Week 8
The four images below are from the Carnegie Stage 22 human embryo during week 8 of development.

|

|

|

|
- Links: Carnegie stage 22 | Week 8
Tongue Muscles
- Tongue muscles originate from the somites.
- Masticatory muscles (MM) originate from the somitomeres. These muscles develop late and are not complete even at birth.
- Tongue muscles develop before masticatory muscles and complete by birth.
Developing muscle fibers within the tongue. Note the multinucleated appearance of each muscle fiber and their overall organization. Muscle goes through the same developmental changes as other skeletal muscle.
See also: Embryonic and postnatal development of masticatory and tongue muscles.[3]


- Links: Skeletal Muscle Histology
Tongue Innervation
The hypoglossal nerve (CN XII) provides the motor innervation of the intrinsic and extrinsic tongue muscles allowing protrusion, retrusion, and changes in the shape of the tongue. Motor units within the hypoglossal motor system can be categorized as predominantly fast fatigue resistant.[4]
The human tongue innervation has been recently analysed histologically and described as extremely dense and complex.[5] The structure of the motor endplate junctions (neuromuscular junctions) was found to be of the multiple en grappe (grapelike cluster) form. The transverse muscle group that comprises the core of the tongue was found to have the most complex innervation. The pattern of innervation of the human tongue also has specializations not found in other mammalian tongues, this allows for fine motor control of tongue shape.
The pathway of the hypoglossal nerve can be imaged using magnetic imaging (MRI) while computer tomography (CT) can show the bony anatomy of the neurovascular foramina of the skull base. Clinically, the nerve pathway can be divided into three regions: intra-axial, cisternal, skull base and extracranial segments.[6]
Lingual Frenulum

Frenulum is a general term for a small fold of integument (skin) or mucous membrane that limits the movements of an organ or part. There are several anatomical frenula associated with the genital system, while the lingual frenulum is associated with the inferior side of the tongue.
The lingual frenulum length (short) and position of insertion (anterior) can lead to speech disorders and may affect postnatal feeding.[7] Interestingly, it is the prevalence of pain in mothers breastfeeding infants with ankyloglossia that presents many problems in breastfeeding.[8]
Children with a frenulum length of more than 2 cm do not show these speech problems. Ankyloglossia (tongue-tie) is the general clinical term for the short frenulum which limits the range of movement of the tongue, there is still no accurate classification for this condition.[9] Frenotomy, frenectomy, and frenuloplasty are the main surgical treatment options to release or remove an ankyloglossia.
Histology

Circumvallate papilla
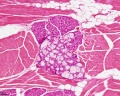
Muscle, salivary gland, white adipose tissue
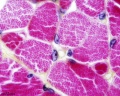
Skeletal muscle

Abnormalities
Macroglossia

Term means an abnormally large tongue. Macroglossia is more common than microglossia and can be associated with a number of genetic abnormalities including: trisomy 21 (Down syndrome), acromegaly, Beckwith-Wiedemann syndrome, mucopolysaccharidoses and primary amyloidosis. There is also an association with congenital hypothyroidism and diabetes.

Macroglossia associated with Beckwith-Wiedemann syndrome.
- Links: Trisomy 21 | Medlineplus - Macroglossia
Microglossia
Term means an abnormally small tongue.
Ankyloglossia
Ankyloglossia (tongue-tie) is the general clinical term for the short lingual frenulum (less than 2 cm), that limits the range of movement of the tongue, prevalence ranges between 4.2% and 10.7%. This is associated with speech development disorders and has been suggested as also associated with feeding disorders. There is still no accurate classification for this condition.[9] Frenotomy, frenectomy, and frenuloplasty are the main surgical treatment options to release or remove an ankyloglossia, though there is still discussion about surgical intervention.
A short lingual frenulum is also associated with a number of genetic syndromes such as: ROR2-Related Robinow Syndrome, Dystrophic Epidermolysis Bullosa, Oral-Facial-Digital Syndrome Type I, Opitz Syndrome (X-Linked Opitz G/BBB Syndrome) and Van der Woude syndrome.
- Links: Medline Plus - Tongue tie | ROR2-Related Robinow Syndrome | Dystrophic Epidermolysis Bullosa | Oral-Facial-Digital Syndrome Type I | X-Linked Opitz G/BBB Syndrome
References
Articles
<pubmed>9060129</pubmed>
Search PubMed
Search PubMed: Tongue Development | Macroglossia | Microglossia
External Links
- Clinical Methods The Tongue
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, June 5) Embryology Tongue Development. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Tongue_Development
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G