Book - Contributions to Embryology Carnegie Institution No.40
| Embryology - 28 Apr 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Meyer AW. Hydatiform degeneration in tubal and uterine pregnancy. (1920) Carnegie Instn. Wash. Publ., Contrib. Embryol., 40: 327- 364.
| Online Editor |
|---|

Links: Hydatidiform_Mole | Carnegie Collection A type of fertilisation abnormality, when only the conceptus trophoblast layers proliferates and not the embryoblast, no embryo develops, this is called a "hydatidiform mole". Due to the continuing presence of the trophoblastic layer, this abnormal conceptus can also implant in the uterus or ectopically. The trophoblast cells will secrete human chorionic gonadotropin (hCG), as in a normal pregnancy, and may appear maternally and by pregnancy test to be "normal". Prenatal diagnosis by ultrasound analysis demonstrates the absence of a embryo.
|
| Historic Disclaimer - information about historic embryology pages |
|---|
|
Hydatiform Degeneration In Tubal And Uterine Pregnancy

Professor of Anatomy in the Lelaiul Stanford Jr. University.
Volume IX (1920) pp 327- 364 With six plates.
- Links: Plate 1 | Plate 2 | Plate 3 | Plate 4 | Plate 5 | Plate 6 | Contribution No.40 | Volume IX | Contributions to Embryology | Hydatidiform Mole | Tubal Pregnancy
Introduction
The following study is an outgrowth of a survey (planned by Mall) of the embryological collection of the Carnegie Institution of Washington. It was my privilege to share in this undertaking and to be permitted to follow any matters of special interest to me. The following report concerns itself especially with the occurrence of hydatiform degeneration in abortuses and specimens in the Mall Collection which were obtained through operation and were classed as pathological. My attention was attracted to the subject while engaged in an examination of the Hofbauer cells, begun at the suggestion of Mall. For the purpose of convenience I shall discuss the tubal and uterine cases separately, including what is common to both with the latter.
Tubal
Strangely enough, the occurrence of chorio-epithelioma arising from tuba pregnancy seems to be better known and also better established than the occurrence of hydatiform mole within the tube. This is especially surprising in view of the stress laid by Marchand (1898) upon epithelial proliferation in cases of hydatiform mole and in view of the fact that trophoblast formation and epithelial proliferation in general have been regarded as being greater in tubal than in cases of uterine implantation. This is illustrated well by such cases as that of Fellner (1903), in which it was impossible to distinguish by histologic examination between the epithelial proliferation present in a case of tubal pregnancy and that from a chorio-epithelioma. From these circumstances alone it seems to me that one might expect hydatiform degeneration to be relatively more common in the tubes. Moreover, when it is recalled that experts still regard it as impossible to decide upon the question of malignancy or benignity in cases of suspected uterine chorio-epithelioma from histologic preparations alone, this surmise gains more in probability. The presence of hyperactivity in the trophoblast in many cases of tubal pregnancy as compared with the uterine was confirmed also by personal observation, and if, as stated by Teacher (1903), chorio-epithelioma arose in hydatiform moles in approximately 40 per cent of 287 cases, and according to Seitz (1904) and Fraenkel (1910) even in 50 per cent, the occurrence of hydatiform degeneration in tubal pregnancy can hardly be doubted because of this fact alone. Nevertheless, of the 7 cases of tubal hydatiform moles cited by him, Werth (1904) regards only the case reported separately by von ReckUnghausen (1889) and by Freund (1889) as well authenticated. Werth reserves judgment, however, on the case of Matwejew and Sykow (1901), a report upon which was accessible to him, and to me, in a short review only. Seitz, however, accepted the short review of this case as convincing, nor did he question the case of Otto (1871), or that of Wenzel (1893), and he incorrectly credited Wenzel with two cases. Werth, on the contrary, regarded these last two cases, and also that of Croom (1895), which is accepted also by Veit (1899), as undoubted instances of "simple hydropic degeneration of the connective tissue of the villi so connnon in aborted chorionic vesicles, both from the tubes and from the uterus." Werth unfortunately does not state just what he means by simple hydropic degeneration, but since he speaks of it as common in aborted ova, one may conclude that he refers to changes in the chorionic vesicle which have followed its isolation within the uterus after complete detachment from its implantation site. For want of a better term, such changes may, I presume, be spoken of as maceration changes, although usually they occur under non-putrefactive conditions. However, I do not thereby imply that these changes are similar under sterile and under putrefactive conditions.
Since Werth speaks of simple hydropic degeneration in aborted ova he does not, I take it, refer to a dropsical condition of the villi possibly due to an obstruction of the venous return, for such a condition necessarily would be rare and not common. Moreover, this condition of necessity would have to arise before and not after the death of the embryo and detachment of the chorionic vesicle. As in one of the cases of Hiess (1914), such a specimen also should contain blood-vessels — for, as emphasized also by Ballantyne (1913), the hydatiform villus is not merely an edematous villus.
That any one at all familiar with hydatiform degeneration, in its earlier as well as its later forms, upon gross and microscopic examination, could confuse it with maceration changes in a fairly well-preserved specimen in any but its very earliest stages does not seem possible to me. Normal villi contain capillaries, not to mention other things characteristic of them. Hydatiform villi, on the contrary, do not contain them, or only very rarely so, and in the early stages. When a villus becomes hydatiform — that is, when hquefaction of the stroma occurs — this liquefaction appears in more or less restricted portions of the villus, thus giving rise to the long fusiform and later spherical vesicles so characteristic of hydatiform mole. But when a villus becomes macerated the change is general, and usually also is noticeable in the embryonic and chorionic membrane itself, or at least within the epithelium. The latter usually is lifted from the stroma here and there, the caliber of the entire villus is increased, and the cai)illaries and the stroma show maceration changes as the villus becomes more translucent. This increase in cahber of the entire villus is not due to local liquefaction of the stroma, but to the pseudo-edema occurring in a villus of normal structure and form. In hydatiform moles, on the contrary, the epithelium not only is firmly attached but usually hyperactive. The changes characteristic of hydatiform degeneration may and often do appear in the villi wliile they still are imjilanted, and not only after the chorionic vesicles are detached. This docs not imply, however, that the villi of a detached hydatiform mole can not also undergo maceration changes. They, of course, frequently do so, and it is in such cases as the.se that differentiation may be difficult or impossible, esjjecially if it is to be made from an examination of ill-preserved fragments only. The same thing is true also of the villi in the early stages of hydatiform degeneration and maceration, especially when the latter masks the former. The difficulty would be still greater in case of whole chorionic vesicles which are almost completely dissolved, leaving only a shadow picture formed by a coagulum without nuclei, which nevertheless may retain almost perfectly the form of the chorionic vesicle and of the individual villi. It may long be impossible to differentiate such cases as these, but they form only a relatively small proportion of the whole. The many cases both of uterine and tubal chorionic vesicles which still were implanted and show exceedingly fine instances of hydatiform degeneration, as well as the many splendid examples of groups of villi which were still implanted in the tube or in the decidua, and which were eciually good examples of hydatiform degeneration, leave no room for doubt as to the frequency of occurrence of this condition, even after due allowance is made for the doubtful cases.
Werth further concluded that not one of the 7 cases of chorio-epithelioma regarded as having arisen from tubal pregnancies recorded before 1904 was sufficiently authenticated. Nevertheless, by 1910 Veit felt justified in saying that a considerable number of cases of chorio-epithelioma arising from tubal pregnancies had been described. He added that Risel (1895) gathered 11 cases from the literature and that the second case had been reported since Risel's paper. Since my interest in the subject is largely incidental, I have not taken the trouble to gather from the literature cases of chorio-epithelioma alleged to have arisen from tubal pregnancies which may have been reported since Veit wrote. Moreover, I could not presume to judge these cases critically. Hence I will accept the fact that chorio-epithelioma arising from tubal pregnancy is regarded as established by a number of investigators. If the conception regarding the relation of chorio-epithelioma to hydatiform mole is justified, then the occurrence of hydatiform degeneration in tubal pregnancy must follow on a priori grounds alone. Moreover, whatever the causes of hydatiform degeneration may be, one possibly is safe in assuming that the condition is not restricted to the uterus, and when I noticed that hydatiform degeneration was so very common in young uterine abortuses the surmise that it might he still more common in cases of tubal pregnancy seemed justified. Since over 100 specimens of tubal pregnancies from the Mall Collection were included in the survey originally planned by him, a study of these specimens formed an excellent opportunity for observations on this subject.
That the case of Otto, with its pathetic history, really was one of hydatiform mole, can not be doubted in view of the careful description of the whole case — its clinical history, necropsy, and the histologic examination. This case is interesting also because the degeneration was in its early stages, the hydatids being only as large as a pinhead and the embryo still being present. Moreover, from Otto's description it is very likely that the specimen contained Hofbauer cells which I have discussed elsewhere (Meyer, 1919).
The history of the case observed by Wenzel in 1855 and reported in 1893 is equally complete and equally pathetic, as could be surmised by all familiar with the history of tubal pregnancy. In this case the mole was as large as a "hen egg," the hydatids varied in size from a dot to a "bird cherry (wild? cherry), and the degeneration was universal, although the menstrual cycle of this specimen was given as only 51 days. It is significant that Wenzel expresses surprise that even excellent handbooks of the day had nothing to say about hydatiform mole in cases of tubal pregnancy, except perhaps to refer to the case of Otto. Nor does the case of Wenzel seem to be the first one observed or that of Otto the first one reported, for Storch (1878), in truly epochal, though largely ignored, observations on hydatiform mole, cites Hennig (187G) as stating that two cases of moles in the tube were reported by Blasius (very likely E. Blasius, 1802-75). Since Storch wrote on hydatiform mole it is implied that Blasius saw one of these and not one of another type of mole, and since hydatiform mole is such a striking condition and has evoked much more interest than the other forms, an observation regarding it in the tubes well might travel down the decades, particularly since until recently the occurrence of hydatiform degeneration in the tubes was regarded as extremely rare. This is indicated also by the fact that Menu (1899) still referred to the case of Otto as a curiosity.
Pazzi (1908') states that two cases of extrauterine moles have been described each by Hennig (1872), Farell (1893), Donald (1902), and one case each by Otto, Freund, Theileher, Maret, Matwjew (Matwejew?) and Sycow (Sykow?), Bland Sutton, and one case of ovarian mole by Wenzel (1893). Wilkinson is said to have described a case of rupture of the tube with reduction of the mole to the size of a cherry, and Lob (1902) also gives a case of molar tubal pregnancy without cessation of menstruation. Since I am quoting Pazzi essentially verbatim, it is evident that he did not read the literature critically or discriminate between ordinary and hydatiform moles, but was misled by the old inclusive and confusing usage of the terms mole and molar, still current at the present day.
Krueger (1909) also reported a case of hydatiform mole with a cyst as large as a "walnut." The pedicle was 4 cm. long and attached to the amnion near the insertion of the cord. Krueger spoke of this as a placental cyst but regarded it as a hydatiform-mole-like structure which, microscopically, was limited to a single villus. If this were the only evidence presented by Krueger one might well question the nature of the cyst, but he added that microscopically the beginnings of hydatiform formations could be recognized on other villi also. Hence it would seem that Krueger's case must be added to the authenticated cases of hydatiform degeneration in the tubes.
So far as I am able to learn, then, the literature contains reports of 9 cases of hydatiform mole occurring in the tube, but two or three of these cases are not well authenticated. These 9 cases are formed by the 2 cases of Blasius or Hennig, that of Otto, of von Recklinghausen and Freund, and of Wenzel, the 2 of Croom, that of Matwejew and Sykow, and that of Krueger. A critical reading of Hennig's book on diseases of the tubes and tubal pregnancy makes it quite clear, however, vhcii, Hennig mainly said that Blasius discovered "tubal moles" and that he observed two, and Behm one case of abortion of tubal moles. From Llie context also it is very clear that Hennig was not discussing hydatiform moles, although it is not possible to say whether he meant that he himself or Blasius observed two cases. I should judge that the latter is the idea it was meant to convey. To these 7 authenticated cases I would add that of Maxwell (1910). In reading Maxwell's doscription one must feel that he himself regarded the case as one of hydatiform mole, but deferred to the opinion of the "Committee." This is suggested also by the title of his article. The illustration which accompanies Maxwell's article is so very suggestive, and his description so characteristic of hydatiform mole, that it seems very probable indeed that the specimen really was such. Maxwell states, for example, that "sections of the viUi embedded in the wall of the tube have the typical structureless, bloated appearance of such pathological villi; and though there is no central cavitation in the villi, their structure, associated with the active proliferation of the Langhans layer, suggests that one is looking at a stage just short of vesicle formation." Moreover, as I am about to show, hydatiform mole is so very common both in tubal pregnancies and in uterine abortions as to increase still further the likelihood that Ma:. well's case actually was one of hydatiform mole. This is merely an opinion, and only a completer description or an examination of the specimen itself could decide the matter.
In connection with what was said before, it is interesting that Maxwell also emphasized that epiblastic activity is increased in all abnormal sites of implantation, and any one interested in the problems of tubal pregnancy and acquainted with Mall's (1915) findings will be struck by Maxwell's statement that microscopical examination of many cases of tubal gestation lends no weight to the view that chronic inflammation of the tubes is at all a common causal factor of tubal pregnancy. Nor can I refrain, in this connection, from quoting the uncontradicted opinion of Doran, expressed in the discussion of Maxwell's case, that tubal gestation "probably represents some general deterioration in the generative power among civilized women."
To the 8 cases contained in the literature I wish to add 48 found among the first 1,187 accessions from the Mall Collection. Nor is it necessary to stop with these, for this collection contains many more not here included. It is merely a matter of recognizing the specimens by a routine examination, and since this paper has been written a number of specimens have been recognized among the daily accessions of tubes received through the unselfish efforts and the scientific interest of practitioners in all parts of the nation.
In addition to over 100 free specimens of uterine hydatiform degeneration, I have also seen more than a dozen fine specimens in large sections of uterine implantation sites, and some entire specimens still embedded in pregnant uteri and tubes. Indeed, how many cases of hydatiform degeneration one can find in conceptuses in tubal or hysterectomy specimens will depend very much upon the care with which the examination is made, for the condition undoubtedly is extremely common, and not I'are, as heretofore supposed.
Although the alleged menstrual age of these conceptuses ranged approximately from 6 to 218 days, most of them were young empty chorionic vesicles or mere remnants of such. Portions of quite a number still were implanted within the tubes, however, and among these were two unusually line ones in a rare specimen of twin pregnancy in the tube donated by Dr. Cecil E. Vest, of Baltimore. Since the question of superfetation has been raised also in connection w4th twin tubal pregnancies, I hasten to add that such a phenomenon, even if it ever occurs (which seems exceedingly doubtful) can be excluded absolutely in this case. Both chorionic vesicles were approximately of the same size and lay in practically the same cross-section of the tube, the surfaces of contact being flattened.
Before proceeding with the statistical findings, I may say that the abortuses in the Mall Collection regarded as pathological are grouped (1) as villi only; (2) as empty or partial chorionic vesicles; (3) as chorionic vesicles containing some or all of the amnion; (4) all specimens containing nodular, or (5) cylindrical embryos, or (6) stunted, and (7) macerated and mummified fetuses. Any one interested in this classification will find it discussed and exemplified in an article by Mall (1917).
There were 40 tubes containing villi only, and in 14 of these hydatiform degeneration probably was present. In 10 specimens its presence was undoubted, but in 4 it was probable only. I realize that this margin of probability is exceedingly largely, but this is easily understood if it is recalled that often only a few degenerate villi embedded in clot were contained in the cross-sections of many of the tubes, and that only a few sections were examined, not, of course, a complete series of each tube. Had the entire tubes been examined, or if more villi had been present, and if those present had been better preserved, the difficulty would have been almost wholly obviated. However, it is idle to set forth these things, because such conditions never will obtain, and the margin of probability becomes greatly reduced if it is remembered that in a large series the specimens necessarily supplement each other. Moreover, the changes in the villi often are so typical that they are unmistakable, even if only a few villi are present. Besides, examination in complete series undoubtedly would increase, not decrease the number found. In some of the doubtful cases the existence of hydatiform degeneration became probable only upon comparison with the many uterine specimens previously examined.


The evidence offered by the 36 tubal specimens in the second group, which is composed of empty chorionic vesicles or parts thereof, was very conclusive, for the cut portions of most of these tubes contained considerable portions or even sections of whole chorionic vesicles, sometimes quite free from clot. Some of them were implanted almost perfectly in the wall of the tube, and although many of them were folded extremely and collapsed more or less, small areas of several were nevertheless implanted undisturbed within the tube. The villi in some of these implanted specimens were so characteristic and the whole picture so exquisite, that the specimens rightly belong among the very finest instances of hydatiform degeneration found anywhere so far. This is true in particular of the case of twin pregnancy received from Dr. Vest. In this specimen the two chorionic vesicles, the intervillous spaces of which were devoid of blood, lay in almost the same transverse diameter of the tube and hence had distended the latter considerably. Both were implanted quite well over the entire area of contact, which included the whole perimeter of the tube. The chorionic vesicles were; flattened at the region of mutual contact, which divided the tube somewhat unequally as shown in figure 1. Although the embryo and the amnion long had disintegrated completely, and although the chorionic membrane itself is thin, covered by degenerate epithelium and also disintegrating, the epithelium of the villi not only is well preserved but is accompanied by large masses of trophoblast and considerable syncytium. Syncytial buds are found on the chorionic membrane also. The tubal mucosa is larger and the tubal wall partly destroyed by the invading trophoblast. Only a few small vestiges of the walls of the villous vessels remain, and the stroma of all the villi has undergone changes characteristic of hydatiform degeneration represented in figure 2. One villus also contains an epithelial cyst resulting from epithelial invagination with subsequent isolation of the distal extremity, a process to be referred to later in connection with uterine specimens. Since most of the villi of this and similar specimens still are implanted in the tube, there can no longer be any question as to the time in which hydatiform changes in the stroma of the villi may be inaugurated. As illustrated in other instances in which isolated and small groups of villi still were implanted, the advent of degeneration of the stroma occurs, in part at least, before the villus is detached. Hence it is not merely a post-mortem or maceration change.


Another very interesting specimen of tubal implantation is No. 1771, received from Dr. H. M. N. Wynne, of the Johns Hopkins Hospital. The menstrual age of this specimen is 49 days, but its anatomic age, as based upon length according to Dr. Streeter's curve (unpublished), is 37 days, thus showing a discrepancy between the menstrual and anatomic ages of 12 days. The embryonic length is only 12.5 mm., although with a menstrual age of 49 days it should be at least 18 mm. Upon examination, Dr. Streeter found the chorionic vesicle to contain a good deal of magma, some of which still was adherent to the embryo, as figure 3 shows. As has been repeatedly emphasized in the hterature, the presence of this coagulum in itself probably indicates that the embryo died some time previously.


The wall of the tube is quite thin, as figure 4 shows, but the implantation is fairly well preserved around the whole perimeter of the specimen. The mucosa is destroyed throughout the greater extent of the section and the trophoblast is abundant, except in one rather degenerate and hemorrhagic area. The chorionic membrane is thin but contains some vessels distended with blood. The stroma of many of the villi also contains vessels filled with blood, but the vessels in many others are very evidently in degeneration. The syncytium is scanty and many of the villi are very plainly hydatiform, as seen in figures 5 and 6.

A third exceptionally fine specimen of tubal hydatiform mole is No. 2052, donated by Dr. N. M. Davis, of Washington, D. C. Figure 7 shows a portion of the tube containing the hydatiform mole, some hydatiform villi of which protrude through an incision in the wall of the tube. The whole opening is filled with typical hydatiform villi barely detected by the unaided eye but perfectly evident under an enlargement of 4 diameters. They present an extremely fine picture when seen with the binocular under a magnification of 10 to 20 diameters. Examination under a higher magnification shows that the preservation of the specimen is unusually good and that all the villi are markedly hydatiform. Trophoblastic proUferation is so marked that in some places it gives the appearance of decidual formation.
Relatively little syncytium is present, but the trophoblast invades the muscularis in many places and a good deal of coagulum is present, most of it apparently having arisen from degeneration changes in the stroma of the mucosa and from similar changes in the trophoblast and the muscularis. The latter is moderately invaded by round cells. No remnant of the wall of the chorionic vesicle or of the amnion or embryo could be detected in the sections examined, both evidently having been absorbed completely, only some of the villi remaining behind; or, the chorionic vesicle may have been aborted and these villi left implanted within the tube.
Some exceedingly fine hydatiform villous trees wore found among the specimens in this group. Scaffoldings or frameworks formed by proliferating syncytium arising from the epithelium of the chorionic membrane also were seen. Since the syncytial buds were found far out on proliferations of trophoblast which capped the viUi, and also in the center of trophoblastic nodules, the origin of the syncytium from the Langhans layer would seem to be again and exceptionally well confirmed. In some cases a detached hydatiform villus was fastened by opposite extremities to two portions of the tube wall. It is well to remember, however, that one of these attachments probably was gained before the separation of the particular villus from the chorionic vesicle.
Of the 36 cases remaining in this group of chorionic vesicles without amnion, after deducting 8 (7 of which belong in group 1 and 1 in group 2), 50 per cent showed the presence of undoubted hydatiform degeneration and in 1 additional case its existence was doubtful.
Since only a few specimens are contained in each of the last five groups, I shall treat them as one. Among 28 specimens remaining in these groups 12, or 43 per cent, showed the presence of hydatiform degeneration and 4 others were doubtful. From this percentage it is evident that the incidence of hydatiform degeneration among tubal specimens seems to increase with advancing age of the conceptus rather than decrease, as will be emphasized in connection with the uterine specimens to be considered later. This probably can be attributed to the fact that the specimens in the first group are composed of villi only, and that many of the empty chorionic vesicles in group 2 were detached from the wall of the tube by hemorrhage before hydatiform degeneration had developed sufficiently to enable me to recognize it. Moreover, it must be remembered that all tubal specimens, no matter in what group they are classified, are in fact young specimens, and since those falling in the latter grou])s succeeded in maintaining a foothold in spite of repeated hemorrhages, a larger number of them might be expected rightly to show the presence of a hydatiform change.
The incidence of hydatiform degeneration in the 104 tubal pregnancies classed as pathologic is 44, or 42.3 per cent of the whole. This is a somewhat higher incidence than was obtained in the 348 uterine abortuses classed as pathologic. and may be accounted for partly, or wholly even, by the greater incidence of young specimens in the tubal series. That the tubal specimens undoubtedly were younger follows from common knowledge regarding tubal pregnancies alone, but it also is shown by the average menstrual ages, which were 43.4 days in 25 tubal, as compared with 66.6 days in 51 uterine specimens. Moreover, 32 of the 48 tubal specimens of hydatiform defeneration, or 66.6 per cent, fall into the first two groups, thus again showing that the majority' are small, young specimens.
Although the incidence of hydatiform degeneration among the pathologic tubal specimens is but slightly higher than that among the pathologic uterine specimens, the incidence of hydatiform degeneration in all tubal specimens contained among both the normal and pathologic is twice as high as that among the same classes of uterine specimens. This can be explained only partlj' by the fact that a larger proportion of the tubal specimens are young and pathologic. The pathologic tubal specimens form 69.2 per cent of 153 normal and pathologic tubal specimens found among the first 1,187 accessions, but the pathologic uterine specimens form only 33.6 per cent of the normal and pathologic uterine groups among the same accessions. But the real question remains, for the incidence of hydatiform degeneration among the specimens classed as pathologic was essentially the same in tube and uterus. Hence an increased incidence of 100 per cent in hydatiform degeneration in the tubes may be due to the less favorable nidus found there. If so, it throws a very significant light upon the probable cause of hydatiform degeneration, which would seem to he in the conditions surrounding the implantation and early development rather than in the ova or spermatozoa themselves.
The conclusion reached in a study of uterine specimens that hydatiform degeneration is absolutely less, not more frequent near the menopause, is confirmed also by the study of the tubal specimens. The average age of 20 women in the tubal series was 33.9 years, as opposed to an average of 31 years obtained from 36 women in the uterine group. This age difference offers a tempting opportunity for generalization, and did the statistics include thousands of cases one might be willing to say that it points to a progressive change as cause, which begins in the uterus and finally reaches the tubes. But strangely enough, the average number of years of married life of 15 women in the tubal series is exactly the same as that of 29 women in the uterine series, or 7.1 years. This fact at once guards against a venturesome hypothesis, for it allows no longer period for the supposed ascending change to reach the tubes than the uterus.
Eight of 20 women from the tubal series had borne one child, 4 had borne two, and 3 more than two; thus again more than confirming the statistical findings in the uterine series, which show that 9 of 33 women had borne once and 18 but twice. The parallelism between these statistics is striking indeed, especially if the small numbers be considered; 14 of 23 women, or 60.8 per cent, in the tubal series had aborted but once, as compared to 19 out of 44, or 46.3 per cent in the uterine series, a fact which again points to the middle rather than to the end of tlie reproductive life of these women.
I do not know whether or not hydatiform degeneration in the tube also is relatively more common near the menopause, as will be shown to be the case in the uterus, for I have not been able to obtain data on the relative frequency of tubal pregnancy in the different decades in the reproductive life of women. However, since by far the greater number of pregnancies usually occur early in this period, it probably would be safe to assume that most of the tubal pregnancies occur also at this time. Consequently, it might well follow that the ratio of tubal hydatiform degeneration to the number of pregnancies occurring in the later actually might be greater than that in the earlier decades.
The structural changes in hydatiform degeneration will be considered more fully in connection with the uterine cases. Suffice it to say that since I directed my attention especially to hydatiform degeneration I have been able to recognize its presence repeatedly at sight in relatively young vesicles (1 cm. large) not only from uterine but also from tubal pregnancies. This is, of course, especially true in the former, for the chorionic vesicles of these often are {}uite characteristic, and if inspection with the unaided eye or with a reading glass under a magnification of 2 diameters fails to reveal the true nature of the specimen, examination with a binocular under a magnification of 10 or 20 diameters often makes immediate identification possible.
Uterine
To read the titles of articles on '"molar" pregnancies which have appeared during the last few decades, even, is a rather wearisome task. By far the great majority of the articles concern themselves merely with the report of "a case" or (rarely) of "several cases" of hydatiform moles. The recent cancer hterature stands in marked contrast to this, for not even the general practitioner would think of reporting a routine case of cancer of the breast, let us say. The significance of these facts is self-evident, and whatever else they may mean they do imply that hydatiform mole still is regarded as a rare condition. Indeed, many of those reporting "a case" frankly say so, and although the incidence of hydatiform degeneration is estimated variously by different authors and investigators, there seems to be entire agreement that it is a rare, even if not an extremely rare condition. Tliis opinion seems to be shared even by those general practitioners whose long practice runs high up into the hundreds or even into the thousands of obstetrical cases. Indeed, many general practitioners declare that they have not seen a single case of hydatiform mole diunng the practice of a long life.
This prevailing opinion can not be attributed solely to the influence of the schools or to books, but is based upon the actual experience of the individual practitioner and upon his conception of what constitutes hydaliform degeneration. This is illustrated, for example, by Menu, who said that a small hydatiform mole weiglis 300 grams, a large one 8,000, with an average weight in his series of cases of 1,700 grams. But even specialists in charge of hospitals have reported experiences similar to that of the general practitioner. Pazzi (1909), for example, stated that although he had observed more than 6,000 cases of labor in liis private and hospital practice, he never met with a case of hydatiform mole. Moreover, it would seem that only some specialists have come to regard the condition as somewhat less rare than was hcretofon; supposed. This is well expressed by Williams (1917), who wrote: "Hydatiform mole is a rare disease, occurring, according to Madam Hoivin, once in 20,000 cases. On the other hand, the statistics of Williamson would indicate that it may be found but once in 2,400 cases." Williams adds, however, that in his own experience it occurred even more frequently than stated by Williamson; and Essen-Moller (1912), on the basis of 6,000 cases treated between 1899-1908, gives the incidence at the Frauen-Klinik at Lund as 3 per 1,000. My former colleague, De Lee (1915), in commenting on hydatiform degeneration, also stated that he has "frequently found in aborted ova one or more vilU degenerate and forming vesicles"; and similar remarks were made also by others, notablj^ by Miiller (1847), Marchand (1895), Veit (1899), van der Hoeven (1900), Hiess (and according to him also by von Hecker), Langhans, Weber, and Frankel. Findlaj' (1917) also regards "it as fair to conclude with Veit, Freund, and Dunger that abortive types of hydati- form mole are commonly overlooked," and although he gave no evidence for his opinion Weber (1892) insisted that hydatiform mole "occurs much oftener than we are led to believe from books or other literature." Essen-IMoller say's Konig gave an incidence of 1 j^er 728 cases. Pazzi (1908) stated that Dubisa}' and Jennin found in 1903 that hydatiform degeneration occurs once in 2,000 pregnancies, and that Cortiguera in 1906 declared that the frequency' of hydatiform mole has a discouraging variation of from 1 in 3,000 to 1 in 700 labors, but that in his personal experience Cortiguera saw one case in every 300 labors. The latter incidence is only slightly higher than that given by Essen-Moller for the clinic at Lund, and somewhat below that of Kroemer (1907), who found 15 hydatiform moles in 3,856 births, or one in every 257 cases. Mayer (1911) reported 10 instances among 3,105 cases of labor, an incidence of 1 in 310 cases, and it is only necessary to add that Donskoj (1911) stated that the incidence of hydatiform mole in 28,406 cases at the Frauenkhnik at Miinchen, between the years 1884 and 1910, was only 1 for every 4,058 births, to emphasize the discouraging variation of which Cortiguera spoke. Donskoj also stated that Engel gave the incidence as 1 in 800, and Korn as 1 in 1,250 births. Such a surprising fluctuation in the apparent incidence in adjacent communities points to differences in conception of what constitutes a hydatiform mole, and also to differences in character of the material upon which the calculations are based.
The existence of hydatiform degeneration in far greater frequency than commonly supposed is indicated also by the records of the Department of Embryology of the Carnegie Institution of Washington. However, the material covered by these records is not identical with that upon which the above opinions, or those of other obstetricians are based. The opinion of the obstetrician is based upon material belonging very largely in the later months of pregnancy, while that in the Mall Collection, on the other hand, belongs very largely in the earUer months. Hence this material is not truly representative of the entire period of gestation, but the same thing is true of the material upon which the general practitioner, the obstetrician, and the gynecologists have based their opinions, for these are based largely upon material from the last months of pregnancy. Hence mainly the cases of hydatiform degeneration which survive come to their attention.
But unless we can assume that the incidence of hydatiform degeneration is constant during the whole period of gestation, its incidence at any particular time of this period may very incorrectly express that at any other time. This could fail to be true only if the incidence of death of the conceptuses and their susceptibility to hydatiform degeneration were exactly uniform throughout every period of intrauterine life. But we know that neither is true, for it is common knowledge that by far the great majority of the cases of uterine hydatiform degeneration, recorded in the literature, are mature specimens of total or partial degeneration obtained in the later months of pregnancy. Although such specimens may contjiin villi in various stages of degeneration, they nevertheless represent end or near-end results. Like the fetuses which rarely accompany them, they are full-term or near-term products when regarded as hydatiform degenerations, and unless we are to assume that conceptuses once affected by hydatiform degeneration always survive up to this period, statistical deductions based upon the cases that do survive can give us httle idea of the actual freciuency of the condition throughout the entire period of antenatal life.
That the specimens upon which past and also present opinion is based usually were large, is confirmed by the belief in the prevailing clinical criterion of the existence of a disproportionately large uterus in cases of hydatiform mole. The emjihasis laid on this by clinicians is well illustrated by Seitz, who says that cases in which the uterus is too small are the exception. Indeed, it seems that the validity of this cUnical dictum has been questioned only very recently by Briggs (1912). Since most early conceptuses showing hydatiform degeneration have been inhibited in growth before being aborted, it probably is only the specimens which persist that produce a uterine enlargement greater than could normally be expected. However, since — as emphasized by Gierse (1847), Storch, Hicss, and others — most hydatiform moles are expelled early and spontaneously, it is evident that these can not have been adherent — that is, have penetrated very deeply — or they would not have been expelled early and spontaneously. Furthermore, maceration changes so commonly present in aborted hydatiform moles indicate very clearly that a large percentage of them, together with the decidua, had been more or less completely detached from the uterine wall some time before abortion occurred.
As far as one can gather from the literature, iiic present opinion regarding the incidence of hydatiform degeneration would be parallelled quite correctly if, in the case of measles, we assumed that it was as common in octogenarians as in children. Measles, indeed, is an extremely rare disease in advanced age, but it nevertheless is very common in infancy. This is exactly the mistake we have made regarding hydatiform degeneration. It may be and undoubtedly is a rare disease at or near term, as Clierse also stated, but it probably is the commonest of all diseases during the earliest months of gestation. The typical large hydatiform mole is an end result which it has taken long months to develop. No one seems to have followed its evolution, although hydatiform degeneration, whether total or jiartial, is, of course, gradual in its advent.
The records of the Mall Collection contained 8 cases of hxdatiforni mole in the first 2,400 accessions, showing a fretiuency 8 times as great as that given by WilUamson, or an excess of 700 per cent. Since the lirst 2,400 accessions contain 309 ctises of tubal and also 2 of ovarian pregnancy, only 2,089 uterine specimens remain. Hence the recorded incidence in the uterine specimens really is 8 in 2,089, or 1 in every 261 cases. This incidence is only slightly lower than that of Kroemer, and somewhat higher per 1,000 than that given by Essen-Moller for the Frauenkhnik at Lund, or the personal experience of Cortiguera.
The highest incidence of hydatiform degeneration previously reported is that of Storch, who estimated it as 50 per cent, but he unfortunately did not give a record of his cases. However, Storch emphasized that the typical complete hydati- form mole is a relatively rare form of the disease, and that all manner of transition forms between the normal chorionic vesicle and the completely degenerated one can be shown to exist. Storch further emphasized the commonness of hydatiform degeneration, especially in the early months of pregnancy, but as Veit (1899) well said, Storch somehow has not received sufficient credit for his investigations. Gierse was forgotten completely. This seems strange, especially in view of the fact that Storch's work was done in Copenhagen, where Panum (1860) had done and still was doing such fine and very suggestive, indeed epochal, work on the origin of monsters. Although Storch devoted part of his paper to myoma fibrosum, and reported only 5 cases of hydatiform mole, one of which, however, accompanied a living fetus, his opinions on the whole were far ahead of his time. In order to make this clear I shall quote a very significant passage, which indeed needs but slight changes to serve as a conclusion for my own investigations:
- "Nun sind aber bekanntlich Eier mit blasiger Degeneration der Zotten und fehlerhaft oder nicht entwickeltem Fotus ein sehr hiiufiger Befund bei Aborten aus den ersten Schwan- gerschaftsmonaten. Mehrere solche Eier sind schon in den bekannten Arbeiten von Dohrn und Hegar beschrieben worden. Ich habe im Laufe des letzten .Jahres eine grossere .\nzahl von Aborten untersucht und derartige kranke Eier in mehr als der Halfte der Fiille gefunden. Nicht selten ist die Amnionblase vollig leer und enthalt nur eine klare serose Fliissigkeit. In anderen Fallen sitzt an der einen oder anderen Stelle der Innenfljiche des Amnion ein kleiner rundlicher oder unregelmassig geformter, 5-I Mm. grosser Korper, welcher aus Nichts als aus runden, schwach conturirten, zum Theil fettigentarteten Zellen und einer hellen, fast homogenen Zwischensubstanz besteht, und der durch einen feinen, 1-3 Mm. langen Strang von ahnlicher Natur mit dem Amnion verbunden ist. In noch anderen Eiern ist der Embryo zwar etwas weiter entwickelt, aber von den verschiedensten Formen von Alissbildungen befallen. Seltener ist der Embryo einigermaassen wohl gebildet und von bis zu 2 Cm. Lange, wie dies auch Hohl nur einmal gefunden hat. Sehr gewohnlich ist fettige oder lipoide Entartung des Embryo vorhanden; derselbe ist dann eine kiirzere oder langere Zeit vor der Geburt abgestorben. Als die aussersten Glieder dieser Reihe von kranken Eiern stehen endlich die sehr seltenen Falle, in welchen der Embryo seine Entwickelung ziemlich ungestort fortgesetzt zu haben scheint, und von denen die Fiille von Martin und der oben beschriebene dreimonatliche abort Beispiele sind.
- "Die blasige Entartung der Chorionzotten kann demnach neben den verschiedensten Zustanden des Embryo fegunden werden. Sehr hiiufig ist letzterer der Sitz von mehr oder weniger eingreifenden Krankheitsprozessen gewesen, die in demselben verschiedene Aliss- bildungen hervorgerufen und ihn in seiner Entwickelung gehemmt haben. Es sind diese Krankheistprozesse wahrscheinlich immer sehr friih im Ei entstanden, und miissen mit Panum zuniichst als entziindliche A'organge aufgefasst werden, welche nach ihrer Intensitat und vielleicht nach dem Zeitpunkte, zu welchem sie im Keime auftreten, bald eine theilweiso N'crocliinp der KeinuinlaKPn dcr mcisten wiclitiKorcii Or^ano mit N'crkruppcUing des ganzcn embryonalon K()ri)ers, bald niehr locale I\lissl)il(hingeii oiiizi'lncr Korjier- thcile horvorrufcn koiinen. Das Erstere ist in den hicr hosprochenen Aburteii sehr hiiufig der Fall: der Embrj'o ist zu eineni unfDriiilichen Kluniiien umgewandelt, dein die nieisten Organe deren Keiine dvirch Entziiiuhing zerstc'irt worden sind, giinzlich fehlen. ^'oIl diescn verkriippelteii Aniorphi linden sieh in anderen Eiern alle Uebcrgiingsfornien zu niehr oder weniger entwiekelten Missbildungen was auch Paniini an einigen Beispielen nachgewiescn hat. Es Scheinen in der That die nicht zerstorten Keinizellen der verschiedenen Organe, nach dem ablaiife des Krankheitsprozcsscs, ihren ursi)runglichen Entwickelungs- j)lan mit einer oft merkwiirdigen Hartniickigkeit, so gut sie es kcinnen, festzuhalten. Von dieseni \'erhaltnisse liefern die bekannten herzlosen Amorphi, die durch einen Zwillingsbruder einhiirt werden und dadurch zu einer oft bedeutenden Cirosse heranwachsen konnen, ein schlagendes Beispiel. In unseren Aborten sind zwar diese Amorphi, die keinen Zwillings- bruder zur Erhaltung ihres Krcislaufes geliabt haben, fruhzeitig zu (Jrunde gegangen, und ihre Clewebsteile sind einer fettigen (lipoiden) Entartung anheimgefallen ; sie haben jedoch ihre Entwickehmg eine Zeit lang fortgesetzt.
- "Est is von den verschiedenen Verfassern vielfach von einer Auflosung der Embryonen in der Amnionfliissigkeit und von einer nachherigen Resorption derselben gesprochen worden. Ich glaube indessen, dass die.sen Vorgiingen eine sehr geringe RoUe beizulegen ist. Man findet in der Tlmt gewohnlich Nichts, was auf eine solche Resorption deuten konne. Es scheinen vielniehr die abgestorbenen Embryonen auch lange nach ihrem Tode eine v;rosse Wiederstandfiihigkeit gegen die Einwirkung, von .\mnionflussigkcit beizubehalten. Ich halie mehrmals ganz kleine, verkriippelte Embryonen zwar fetig entartet, in ihrer Form aber v(")llig wt)hl erhalten, in Eiern gefunden, die bis zu 10 Monaten im Uterus zuriickge- hiilten worden sind. Zudem ist die Amnionfliissigkeit in diesen Eiern meist ganz klar, oder sie enthalt nur losgestossene, hinfiillige Amnionejiithelzellen suspendii't. Wenn daher die Eier ganz leer gefunden werden, so riihrt dies gewiss am Hiiufigsten tlaher, dass der Primitivestreifen seiner Zeit vollig destruirt worden und somit gar kein Embryo zur Ent- wickehmg gewommcn ist. * * * Im AUgemeinenerreichensiekienebedeutende (iriisse und werden zudem oft fruhzeitig aus dem Uterus ausgestossen, in dem sie, wie oben bcsprochen, ein sehr betriichtliches Contingent zu den Aborten iiberliaupt liefern. * * *
- " Die Traubenmole und die verschiedenen Ucbergengsformen derselben, die an Aborten sehr haufig vorgefunden werden, ist als Hyperplasie und secundiire cystoide Entartung des (von AUantois nicht herstanuumenden) C'horionI)indegewebs vorzugsweise charactertisirt. Die Krank^'eit wird von pathologischen Zustiuiden der i'lbrigen Eitheilc, Amnion und Embryo (Missbildungen, ^'erkriipl)elungen und friihzeitigem .\bsterben des letzteren) sehr haufig begleitet. Seltener ist der Embryo regelamasmig entwickelt, stirbt al)er meist auch dann wegen mangelhafter Vascularisation der (Chorion) Placenta fruhzeitig ab. Sehr selten scheint der P^mbryo ungestort bis zur Geburt sich fort entwickelt zu haben."
But the unregarded observations and illustrations of (Jierse arc still more startling than these opinions and observations by Storch, who knew of CJierse's observations published posthumously by Meckel. The latter quite correctly stated that such careful observations as those made by Clierse always introduce new i)oints of view. If it be remembered that in these days, almost a century later, specimens of hydatiform degeneration which are 4 cm. in diameter still are reported separately as examples of early hydatiform degeneration, the great merit of Gierse's observa- tions in this regard alone will be clearly evident, upon recalling that Giersc pictured a hydatiform villus from a chorionic vesicle tlie size of a hazelnut (about 12 mm.), the largest hydatiils on which were only one-tliird of a line large. Moreover, Gierse added :
- "Derlcichen geiinge krankhafte Veranderungen finden sich an au.serordentlichen vielcn Abortus, und sie scheinen die hiiufigste Ursache des Abortus in den ersten Monaten zu sein."
How such an epoch-making conclusion not only could be forgotten, but absolutely overlooked or disregarded, by all but a few of the scores upon scores who have written on hydatiform degeneration, it is difficult indeed to understand. Gierse, who took steps to ascertain what normal villi look like, stated that villi with marked irregularities as described by Desormaux, Breschet, Raspail, and Seller undoubtedly were abnormal; surmised that vilh in abortuses seldom are normal, and added that between the slight pathologic changes in the caliber of the vilh and the most evident hydatiform moles the plainest transition can be found. Among other important things Gierse also recognized the early fenestration of the stroma and pictured such a villus under a magnification of 250 diameters, and although reported very briefly, his findings, wholly confirmed here, still wait for general recognition.
Just as the great majority of specimens described in the literature are large, so 4 of the 8 specimens originally classed as such in the Mall Collection also are large, and none of the 8 are very young, as the following protocols show:


- No. 70 (Dr. Charles H. Ellis) is a small, fimi, degenerate-looking, almost solid mass 40X30X28 mm., composed of small cysts, degenerate decidua, exudate and degeneration products. As figure 8 shows, it is very similar to a very much larger specimen. No. 323 (Dr. V. Van Williams). The latter is a large, firm, felt-fike mass 120X90X65 mm., represented in figure 9. The individual cysts, which vary from 1 to 20 mm., are packed together rather firmly, though a few large ones are free. The exterior of the specimen is formed by a thick layer of degenerate decidua and gives only a slight indication of its true nature upon closer inspection or upon examination of the cut surface. No fetal remnants were noticed, and microscopic examination shows tliat the specimen is composed merely of a large hydatiform mass which was retained for a long tune and then aborted in toto with the surrounding decidua and exudate.

- No. 749 (Dr. G. G. McCormick), on the contrary, is a fresh, loose, typical hydatiform mass composed of loase hydatids of various sizes, as shown in figure 10. As the specimen floats loosely in fluid, it fills a half-liter jar about two-thirds. A considerable portion of the hydatid cysts are glued into a solid mass by blood, exudate, and decidua, which form a layer on the exterior.

- No. 1323 (Dr. J. W. SchUeder) also is a large mass very like the preceding, which completely fills a liter jar. It is accompanied by much clot and composed mainly of a large, thick-walled, hemorrhagic, necrotic mass 80X50X45 mm, containing a large, thin-walled cavity 65X30X25 mm, which is broken at one end. This cavity which is apparently that of the chorionic vesicle, is empty, smooth, and thin-walled, except where it is composed of a characteristic hydatiform mass shown in figure 11.

- No. 1325 (Dr. Fred R. Ford), shown in figure 12, is a small, irregular mass 40X33 X 20 mm. , the exterior of most of which is formed by a thin layer of decidua. Within this is a small group of quite tj-pical hydatid cysts, the largest of which measures about 10X5 mm. The appearance of the specimen suggests that it is merely a fragment, though the amount of decidua present indicates that the entire specimen probably was not much larger. The history of this specimen is especially interesting because of the diagnosis of tubal pregnancy, caused by the presence of a cornual myoma and the occurrence of repeated bleeding.
By far the most interesting specimen, in some respects, of hydatiform degeneration among those diagnosed as such upon gross examination in the Mall Collection is No. 1640.
- No. 1640 This abortus, received through the courtesy of Dr. J. W. Williams, measured 40X20 X15 mm. Upon examination Dr. G. L. Streeter found it to be composed of a flattened decidual and chorionic mass which, upon section, showed "pearl-like vesicuhir enlargements which suggest hydatiform degeneration." The exterior of this specimen is composed of a thin, hemorrhagic decidua which completely surrounds the villi. The hydxitid luiture of this clearly is recognizable upon close scrutiny with the imaided eye, and easily becomes evident upon magnification of 12 diameters with the binocular microscope. Examination of the histologic preparations reveals it to be a very fine specimen of relatively early hydatiform degeneration.

- No. 1914 (Dr. G. C. McGorniick) is a fine, very characteristic mass, part of which is shown in figure 13. It is like Nos. 749 and 132.3, but very much larger, for in fluid it completely fills a 2-liter jar. This specimen was said to have accompanied a living, 7-months fetus, having been expelled between the fetus and the placenta. Only a sniidl amount of clot, and what seems to be a small portion of placenta and membranes, accompanied it. Since the placenta was not saved it is impossible to say whether the mass resulted from partial degeneration of the placenta belonging to the living child, or whether it represented a degenerate twin placenta, which is rather unlikely but not imj)ossible, in view of the well- authenticated cases found in the literature. This specimen is of interest not only for the numerous large, clear cysts, one of which measures 30X25 mm., which it contains, but because it accompanied the birth of a living child and because of the relative rareness of such a coincidence. In regard to the latter. Dr. McCormick added that in his experience of over 1 ,000 labors he had never before met this coincidence. The rareness of the specimen is emphasized still further by the statement of Professor Williams that such an instance has not been observed in a series of over 17,930 obstetrical cases treated by the department of obstetrics of the Johns Hopkins Medical School, as well as by the small series of such cases recorded in the literature.


- No. 1926, a companion specimen to No. 1640, is composed of material from curettage received through the courtesy of Dr. Karl Wilson, of the department of obstetrics of the Johns Hopkins Medical School. It was removed from the same patient about a year later than specimen No. 1640. Upon gross examination the hydropic nature of some of the villi is plainly evident, as shown in figure 14, and upon microscopic examination the diagnosis of hydatiform degeneration could be confirmed, although the villi were extremely degenerate. The menstrual history of this case fortunately is known and is thoroughly reliable. The last menstruation occurred January 24 and curettage was done August 4. Bleeding occurred every two or three weeks during March and April and was repeated throughout May. Since the uterus, which had reached the symphysis, had not enlarged any for months, in view of the long duration of pregnancy the operation was performed. The major portion of the specimen is very small. The chorio-decidual portion was felt-like in consistency and extremely fibrous, due largely no doubt to the long retention. Most of the accompanying material looks like mucosa rather than decidua, although some of the larger pieces very evidently contained villi. Some of these were relatively thick and fibrous, and others were vesicular. All of the material was extremely fibrous, making it difficult to get a satisfactory teased preparation. Accompanying this material was a small body 5X7.5X .30 mm., shown in figure 15. Both nodule and stalk contained some remnants of the embryo. Although the appearance of the stalk suggests the umbilical cord, it contains fragments of the body of the embryo, some of which evidently are composed of nerve tissue.
Microscopic examination of the jiedunculated mass further shows it to be composed of degenerate remnants of organs, tissues, and cells. It is partly denuded and partly covered by a layer of fibrous connective tissue which contains local thickenings. In other areas this fibrous layer gives place to a single or more celled layer, or to polygonal epithelioid cells. The interior of this specimen is composed of a degenerate jumble including fragments of the central nervous system, of the heart, liver, and cartilages. The entire body is chaotic in its structure, and small fragments of the nervous system are scattered throughout its entire extent. This would seem to indicate that the disruption of the tissues was mechanical. The material in which these remnants are contained is composed of coagulum, some mesenchyme, cellular detritus, blood and polymorphonuclear leucocytes, degenerated cells, which appear to have been phagocytic, but which are more likely fusion products or "symplasma" (as Bonnet called them). A few remnants of vessels are found only in the fragments of cartilage.
This short review of the gross appearance of the cases of hydatiform degeneration recognized by the unaided eye with the customary criteria, originally classed as such in the Mall Collection, shows that they vary decidedly in their gross, naked-eye characteristics, both as to size and appearance. Xo. 1640 scarcely is distinguishable as a case of hydatiform degeneration from gross appearances alone, unless one's attention is directed especially to the matter, but all the rest of the specimens, both small and large, not only are easily recognizable, but are so characteristic that they could not possibly be overlooked. As was indicated above, the incidence of these specimens of hydatiform degeneration among the first 2,400 accessions in the Mall Collection was 1 in every 261 abortuses, or more than 8 times the incidence given by Williamson, and 1.3 times that given by Essen-Moller. Although this incidence is so much higher, it does not necessarily contradict the statements of Williamson, for it represents the incidence of hydatiform degeneration in abortuses belonging very largely below 7 months. Nor does it tell the whole story for these months, for since the incidence of hydatiform degeneration given in the records of the Mall Collection is based upon determinations made essentially in the usual way — that is, by unaided inspection of the gross specimen alone — we must regard it also merely as an apparent, not as the actual incidence. For, as will appear later, the actual incidence can be revealed only by a careful gross and microscopic study of all specimens, both normal and pathologic. Such a study has not as yet been completed, but 348 uterine specimens classed as pathologic, and 105 pathologic tubal specimens, contained in the first 1,187 accessions, were carefully examined.
The actual number of cases of hydatiform degeneration found among the 348 uterine abortuses classed as pathologic was 112, or 32.4 per cent of the whole. The incidence of hydatiform degeneration in the pathologic tubal pregnancies was somewhat higher even — 44 specimens of undoubted hydatiform degeneration in 105, or 41.9 per cent. Since nearly all the tubal specimens are young, while the uterine series contains many more relatively older ones, the effect of this fact upon the determined relative incidence of hydatiform degeneration among the pathologic tubal and uterine specimens must be borne in mind. For a reliable conclusion regarding the relative incidence in the uterine and tubal pregnancies it would be necessary to select a series from each, composed of specimens of approximately corresponding ages. "What the incidence of hydatiform degeneration is among the uterine and tubal specimens classed as normal I do not know, but it undoubtedly is far below that in those classed as pathologic. It is well to remember, however, that many, if not most of the instances of beginning degeneration very likely will be found among the specimens classed as normal. This is well illustrated by a hysterectomy specimen, No. 83G.
If we assume that the incidence of hydatiform degeneration among the pathologic specimens in the rest of the Mall Collection is the same as that among those in the first 1,1S7 accessions, then we get over 314 estimated instances of hydatiform degeneration in pathologic tubal and uterine cases alone. Since I have found a number of chorionic vesicles accompanying embryos classed as normal which also show hydatiform degeneration, this number would be increased still further; but unfortunately too few of the specimens classed as normal were examined to justify an estimate. Yet these normal specimens form GO. 4 per cent of the first 1,000 and 40.7 per cent of the first 2,500 accessions. This supposed increase, due to inclusion of specimens contained among the normal, would be offset somewhat, however, by the fact that the first 1,000 accessions contain a somewhat larger proportion of young conceptuses, each succeeding 1,000 probably becoming somewhat more representative of actual life conditions. The difference between the composition of the first 1,000 accessions and that of the 1,000 between 1,500 and 2,500 is not very great, however, for the former contains only an excess of 17.6 per cent of cases falling in the first five groups of the Mall classification, which groups are composed largely of specimens below an embryonic length of 20 mm. Then, the relative proportions of tubal and uterine specimens in the different thousands also must be taken into consideration. But in any case the estimated incidence of hydatiform degeneration in the Mall Collection, calculated without regard to those contained among specimens classed as normal, is 7.5 per cent, and the actual incidence hence probably is more than 1 in every 10 accessions. The incitlency among the uterine specimens alone would be 10.9 per cent, and among the tubal alone 20.8 per cent. This difference of 100 per cent between the tubal and uterine specimens may have a probable significance in connection with the cause of hydatiform degeneration.
If, as alleged by various investigators, the great majority of abortions occur in the first 3 months, it is highly probable that many of these early conceptuses are lost and never come to the attention of any one, and that therefore the proportion of early specimens in this or any other collection is no doubt too small. Moreover, in quite a number of specimens of the first 1,000 accessions the chorionic vesicles were too degenerate for examination, and in others they were absent, but we have reason to believe that this is not true to the same extent in the material beyond the first 1 ,000 accessions. Then, too, since only a few relatively large sections from a single portion of the chorionic vesicles were examined, it is evident that some cases in which the degeneration may have been purely local probably were overlooked. Hence the actual incidence of hydatiform degeneration in this collection is probably not merely 8 times but 240 times as great as that givcMi by Williamson (1900), and 33.3 times as great as that given by Essen-Moller.
Most persons will, I presume, be willing to regard an increase of 700 per cent above that of Williamson as possible, but one of 24,000 percent above Williamson, or even 3,333 per cent above that of Essen-Moller as wholly out of the question.
Yet, strange as it may seem at first sight, this is not a random guess but an estimate based upon (hi; actual incidence of hydatiform degeneration as determined by a careful gross and microscopic examination of mounted and unmounted material from over 400 abortuses. However, I lay no special emphasis on these percentages, and am using them merely to emphasize the great frequency of hydatiform degeneration. It matters little whether we shall ultimately determine an incidence of 10 or 5 per cent, but it does matter considerably whether we regard the frequency as 5 or 0.05 per cent, for this is a diference of 10, 000 per cent.
In view of the prevailing opinion, I realize that these findings may seem incomprehensible and perhaps incredible, unless it is distinctly borne in mind that it is not stated that this incidence refers to the later months of pregnancy or to term. What the incidence in the later months of pregnancy may be I do not know, but I have called attention to an apparently well-founded belief that it is a relatively rare condition, the estimates ranging from 1 in 2,000 to 1 in 728 or 300 cases.
In regard to the incidence of hydatiform degeneration in uterine specimens, it should also be remembered that the life, in contrast to the laboratory incidence for the entire period of gestation is higher, not only because the chorionic vesicles were not included in many of the accessions and because others were too degenerate, but because I have not as yet been able to recognize the very earliest stages with entire certainty. Furthermore, many instances of hydatiform degeneration from the early months of pregnancy, especially the first and second, are inevitably lost. The increase due to these things would be offset somewhat, however, by the lower incidence of hydatiform degeneration in specimens from the last months of pregnancy, relatively few abortuses from these months being contained in the Mall Collection.

To what extent the material in this Collection is truly representative of actual life conditions is difficult, if not impossible, to determine. This question could be answered only if all the abortuses and material from abortions actually reached physicians, and if the latter sent all of them to the laboratory. My own impression so far is that the material representative of a sufficiently large community probably would have a somewhat lower incidence, notwithstanding the fact that many specimens not only of hydatiform degeneration, but of abortuses in general, especially from the first month of pregnancy, are lost. However, since the presence of hydatiform degeneration is especially common among early specimens, the inclusion of these might raise the incidence for the whole period of gestation more than the inclusion of all specimens (not excepting those of the last three months) would lower it. But the result obtained would represent the incidence of hydatiform degeneration in abortuses alone, and not that in all pregnancies. The latter could be obtained only by including all gestations which end normally. If we accept Pearson's (1897) estimate that approximately 40 per cent of all pregnancies end prematurely, then the incidence of hydatiform degeneration among abortuses would represent very nearly twice that in all pregnancies. Mall's estimate of 20 per cent prenatal mortality, on the other hand, would give us an incidence only one-fifth as great as that among abortuses. Hence, the actual life incidence of hydatiform degeneration in all gestations would then be 1 in 10, as based upon Pearson's, and 1 in 25. as based upon Mall's estimated prenatal mortality. But even if, as estimated upon this basis, 4 or 10 per cent of all conceptions end in hydatiform degeneration, this does not necessarily contradict the current opinion regarding its rareness at or near term.
A careful examination witli the binocular microscope of all specimens has shown that hydatiform degeneration as a rule is sufficiently general even in young vesicles, so that sections of a single portion about 10 mm. square, would enable one to make a fairly reliable diagnosis. Now and then, however, the process seems to be rather irregularly developed, especially in the larger specimens.
In order to determine accurately the question of distribution of hydatiform degeneration over various portions of the chorionic vesicle, it will be necessary to examine a series of sections of portions of the chorionic vesicle for each small specimen. This has not yet been done, but since the portions used for microscopic examination had been taken at random without previous knowledge of the existence of hydatiform degeneration in any but the 8 specimens above described, and since a series of 453 vesicles was examined, I can not believe that it can often be limited to any particular area on relatively young vesicles. In these it usually is universal even if not complete. It is of special interest in this connection that Muggia (1915), after reviewing the small list of cases of alleged hydatiform degeneration of the chorion laeve in connection with a study of a case of his own, came to the conclusion that these cases are not really degenerations of the chorion laeve, but merely partial degenerations of the placenta. Although I have given no thorough attention to the normal changes in the chorion laeve, I am (quite certain that they are not the cause of confusion in the series of hydatiform degenerations from the Mall Collection. Cases in which whole chorionic vesicles exclusively hydatiform in character were contained in the tubes, and a number of others which still were implanted within the uteri showed equally exquisite hydatiform changes around the whole perimeter. Such cases as these ultimately confirm the oi)inion that in young vesicles as a rule the condition is general except at its very inception. This is true particularly by the time the degeneration has reached a stage which can be considered at all typical in its gross development, as determined by careful examination of numerous specimens with the binocular.

It is especially interesting that, just as soon as syncitial hydatitl elliptical villi, or portions of the same begin to appear, the condition can be recognized with some certainty under a magnification of 12 to 20 diameters with the binocular microscope. It often was surprising how relatively early stages could thus be detected and the diagnosis confirmed later by histologic examination. Indeed, Colloidin blocks of tissue from which sections had been cut gave splendid testimony when examined in Huid with the binocular. One of the not very early stages contained in utero and represented in figure 10 could be recognized with the unaided eye; and when examined with the binocular, under a magnification of about 12 diameters, the picture was unusually fine and wholly unmistakable, as shown in figure 17.
That hydatiform degeneration is incomparably more common in the earlier than in the later months of pregnancy, thus justifying the comparison made with measles, is substantiated by statistics covering the material examined. From these it is evident that, excepting cases of large hydatiform masses originally classed as hydatiform degeneration from inspection of the gross specimens alone, practically all the specimens are relatively young. This is true especially of those from tubal pregnancies, and we may hence regard it as established that hydatiform degeneration is a change which is exceedingly common in the earlier months of pregnancy, just as measles is common in childhood, and that it becomes progres.sively less common as the end of pregnancy is approached, just as does measles as senility is approached. The obstetrician does not see most of the cases of hydatiform degeneration, for they merely are reported as miscarriages and the specimens often are destroyed or retained unrecognized by the general practitioner or the midwife. They often are aborted spontaneously and completely with the decidua and rarely are still contained in a closed decidual cast when they reach the laboratory.
The spontaneity of the abortion, especially in early cases, was emphasized also by Storch in the above quotation. Cortiguera (1906) is reported by Pazzi (1908) also to have declared that many moles disappear wholly without leaving a remnant, even if occurring repeatedly in the same woman, and Donskoj also stated that many of those aborted do not come to the attention of physicians because of their harmlessness. This, however, does not imply that those which persist and develop into large masses are equally harmless, and it must be remembered that it is upon these that the current opinion regarding the tendencies to malignancy of the hydatiform mole is based.
The conclusion regarding the greater incidence of hydatiform degeneration in the early months of pregnancy is conclusively confirmed by the occurrence of 32 of the 48 tubal specimens within the first two classes of the pathologic division of Mall, and 104 of the 112 uterine specimens in the first six classes of this division. Most of the specimens in these classes are composed of villi, of empty chorionic vesicles, or of vesicles with embryos most of which have a length of less than 20 to 30 mm. That hydatiform degeneration is more common in the early months of pregnancy is indicated also by the well-known reports of Kehrer (1894) on 50 cases, and of Borland and Gerson (1896), who found that 63 per cent of 100 cases had aborted in the fourth and fifth months of pregnancy. According to Seitz, Hirtzman (1874) also found that 62.8 per cent of 35 cases had aborted between the third and sixth month. Only 4 per cent of Kehrer's 50 cases and only 3 per cent of the cases of Borland and Gerson aborted at the tenth month. Bonskoj stated that 7 of the 10 cases reported by him aborted in the fourth month and none after the sixth month. He stated further that 56 per cent of Bloch's 50 cases aborted before the sixth month, 44 per cent later than this, one being retained until the fourteenth month. The latter case is especially interesting because retention not only beyond term but after the death of the mole seems to be regarded as relatively rare. This, however, does not imply that retention beyond the period of growth of the hydatid mole does not occur, although Sternberg (1910), who also emphasized the great rarity of this condition, erroneously stated that the (Jerman literature reveals only a single instance of missed abortion in case of hydatiform mole, viz., that of Poten (1901). In this case a hydatiform mole of the size of a duck egg; was said to have been aborted approximately one month beyond term. Hence growth must have ceased long before and the mole have remained in ulcro as a "harmless body." To this case of Poten, Sternberg adds a case in which a hydatiform mole of 14X9.6 X4.3 mm. was aborted in the twelfth month after the cessation of menstruation. Although Sternberg included 4 cases from other countries among these missed- abortion moles, inz., those of Shell (undated), Ferguson (also undated), Colorni (190S), and Gaifani (1908), one can hardly doubt that more cases could be added. Since the case of Shell was one of twin pregnancy in which one conceptus became hydatiform, it is not at all unlikely that some other cases among this rather small series of twin pregnancies accompanied by hydatiform degeneration may belong in this category.
Mayer also emphasized the fact that, although instances of retention of fetuses are very common, instances of retention of hydatiform mole are very rare, only a few cases having been recorded. Mayer refers to 2 cases by Kehrer, 3 of Borland and Gerson, and to 1 case of Lange, and reports 4 of his own. These 4 were found among 10 cases of hydatiform mole, an incidence of retention of 40 per cent. They are interesting, especially in connection with the observation of Briggs that, contrary to current belief, uterine enlargement often is not beyond the normal. Mayer says that this enlargement was too great in but 1 of the 4 cases, and that retention lasted as long as 4 to 5 months.
At least 3 of the cases of hydatiform mole originally recorded as such in the Mall Collection belong among retained specimens, as the illustrations alone suggest. But a fair percentage of detached chorionic vesicles included in the list of cases here reported undoubtedly also was retained after the cessation of growth, and it is for this reason that I further emphasize the fact that the uterine volume in a considerable percentage of these cases also, instead of having been too great for the duration of the pregnancy unquestionably was too small. This is well illustrated by the histories of specimens Nos. 70, 323, 1G40 and 1926, and by the specimens themselves.
The average menstrual age of 51 of 112 uterine specimens of this series of hydatiform degeneration — in which the data were available — was 66.6 days, or 2\ months. As will be seen, this is a far lower average age than heretofore reported, a difference which explains itself from what has been said already. It is interesting that the average menstrual age of 5 of the 8 specimens in the Mall Collection originally classed as hydatiform degenerations is 168.2 days, or 2.^, times as great, thus being in substantial agreement with the usual results. Three of these 5 are large specimens, the fourth measures 40X20X15 mm., and the other is composed of small fragments contained in material from curettage. From this alone it follows that the menstrual age is a very uncertain guide, especially as to the size of a hydatiform mole.



It seems superfluous to add any tiling to the good description of the gross appearance of the typical h3'datiform mole currently reported in the literature. Such cases are so characteristic that even a novice can recognize them at sight. Yet if the findings reported here are reliable, or even approximately so, it nevertheless must be evident that, in the past, the great majority of specimens of true hydatiform mole have remained unrecognized merely because they did not happen to present the customary, well-known picture to ike unaided eye. Small chorionic vesicles, such as No. 2077 shown in natural size in figure 18, which attract no attention upon cursory inspection may, and often do, present the most exquisite picture of hydatiform degeneration when seen under a magnification of 3 to 20 diameters, as illustrated in figure 19. This is true especially if the examination is made with the binocular microscope. Since I have adopted this method of examination it has been possible to recognize instances of decidedly general and typical hydatiform degeneration in chorionic vesicles less than 2 cm. in size, with later confirmation of the diagnosis by a histologic examination. However, I have not been able to recognize very early stages merely by examination of the gross specimens, for gross recognition is possible only when portions of at least some of the villi have become sufficiently elliptical or globular to attract attention. Histologic recognition is possible far earlier than this, as shown in figure 20.

The general appearance of the whole chorionic vesicle sometimes is an aid in gross identification, for the villi not infrequently are smooth, slightly branched, and unusually long, so that the vesicle looks shaggy, as illustrated in figure 21. The typical gross, hydatid or watery, translucent nature of the vilU can not be relied upon in early stages, for normally shaped villi, which have undergone considerable lysis, may be almost transparent and also somewhat more than normally bulbous. However, save in the case of some specimens of tubal pregnancy, the swelling of the villi, due to maceration or to luetic changes, is quite different in character from that characteristic of hydatiform degeneration, and usually quite easily distinguishable from it. Judging from several specimens of villi which were macerated in distilled water during a period of weeks, post partum maceration never could cause confusion and the same thing undoubtedly is true of intra-uterine maceration.
Since numerous trophoblastic nodules are present also in other conditions, notably in retained placentae as found by Aschoff and others. I have not been able to regard their presence in unusual numbers, in some cases of hydatiform degeneration, as of crucial value, but the absence of placental differentiation at a time when it should be present, with a uniform and unusual development of the villi over the whole exterior of relatively large chorionic vesicles, is decidedly significant and has often been found to imply the presence of hydatiform degeneration. The same thing is true of a very irregular distribution of the villi, or of uniformly distributed fusiform enlargements on the villi and of the loss of the dull appearance of their cut surfaces, as seen under the binocular. As soon as the stroma becomes hydatiform, and even before liquefaction is present, the cut surfaces of hydatiform villi look somewhat shiny and waxy or, perhaps better still, parafiine-like, as in the specimen in situ shown in figure 21. A bluish tinge always is present, and this appearance is very characteristic. However, how easily a specimen of hydatiform mole can be recognized by examination with the binocular alone necessarily will depend also upon the condition of the specimen. If the villi are matted, glued, or macerated, not only the early hydatiform changes but even fairly advanced ones often are masked so completely that recognition is difficult or impossibie without histologic examination.
In many early specimens the diagnosis could be made at sight from a histologic preparation under low magnification, even when it was impossible to make a diagnosis by examination with the binocular microscope alone. What makes this possible is not, as has been generally assumed since Marchand's epochal work on chorio-epithlioma, the ajipearance of the syncytium or that of the Langhans layer or of the trophoblast, but the changes in the stroma which precede those in the epithelium. The evidence in regard to this matter is overwhelming, and in the early stages when the stroma already has been altered, it often is impossible to tell whether the epithehal development is normally or abnormally active. Moreover, in spite of Marchant's statement to the contrary, extremely large cysts often have but a single smooth layer of epithelium. This has been asserted repeatedly by other investigators also. The two layers of epithelium are not by any means always present and, while there is no agreement in the matter, the opinion seems to be that the grade of epithelial proliferation can not be used as a criterion for the deter- mination of the presence of hydatiform degeneration. Menu said that the presence of marked epithelial proliferation was emphasized early by Miiller (1847), Ercolani (1876), Franque (1896), and Owry (1897); and according to Pazzi (1908), Ercolani and Polano altogether denied the existence of connective tissue in the hydatiform mole. The same thing was asserted by Sfameni (1903), who claimed to have found further evidence of the exclusively epithelial nature of the hydatiform mole in 1905. According to Sfameni the hydatiform mole does not result from a modification of existing chorionic villi, but from an entirely new growth which is wholly epithehal in character! But this opinion, which was accepted also by Niosi (1906), seems to exist among Italian writers only.
Although Durante (1898) represented extremely long syncytial buds, he nevertheless found (1909) epithelial proliferation present only where certain vascular changes were present. Winter (1907) stated that the condition of the epithelium varies greatly, and Falgowski (1911) emphasized that he could not demonstrate the presence of an increased epithelial proliferation or of vacuolation of the syncytium. Aman (1916) also found that epithelial proliferation may be wholly absent. Ballantyne (1913), on the contrary, found epithelial proliferation "so well developed that it suggested that it is an essential process in the formation of the mole." liallantyne further likened hydatiform degeneration to edematous growths and emphasized that both really are epithelial new growths. This opinion is accepted also by de Hnoo (1914), who regarded the hydatiform mole as a neoplasm of the trophoblast with secondary changes in the stroma.
There is no agreement at present as to whether the epithelial changes are primary or secondary. As is well known, Marchand (1895) — und Miiller, l*]rco!aiii, and Langhans long before that — regarded the epithelial changes as primary, but most investigators seem to have come to the opposite conclusion. Some share the opinion of Schrocder that hydatiform degeneration points to a stimuhis resulting in hypoplasia of the entire chorionic villus. Nor is there agreement as to what the initial changes are. Durante (1909) regarded the presence of vessels with an imperfect endothelial lining and with thick infiltrated walls as the initial lesion in hydatiform degeneration. These changes were noted by him, especially in trunk villi, and epithelial proliferation was most evident where the vascular lesions were most pronounced. Durante further stated that the chain form of the hydatids is due to the fact that the vascular lesions occur at intervals along the villus. Unfortunately, the structure of long hydatiform villi does not confirm such an explanation nor Durante's conclusion that the hydatid cavities within the viUi result from dilatation of the capillaries. Many investigators report the early disappearance of the blood-vessels, a phenomenon which some regard as secondary and others as primary to the death of the embryo.
In the course of this investigation a villus with a normal stroma and normal vascularization never was found to have undergone true hydatiform degeneration, but one with a normally active epithelium — both Langhans layer and syncytium — often was truly hydatiform. That is, it not only was watery in appearance, but also fusiform or globular even in external form. In fact, Marchand (1895) himself found that "Das Epithel welches die Zotten und ihre Anschwellungen bekleidet zeigt ein sehr verschiedenes Verhalten." Yet even to-day, the feeling on the part of many seems to be that unless a marked hyperplasia of the Langhans layer and of the syncytium is present the condition is not one of hydatiform mole. This position seems to me to be untenable for, as Marchand himself said, the change in epithelium usually is least in the young viUi, and he should have added it is unrecognizable in the early stages and in young conceptuses. A perusal of the literature descriptive of the actual cases leaves little doubt upon this point, and a careful study of the advent of the earliest recognizable changes in hydatiform mole is absolutely convincing. The earliest recognizable, even if not the incipient, changes occur in the stroma and in the vessels — and not in the epithelium. In passing, it may be noted that although Marchand stated that the change in the epithelium is primary, he nevertheless somewhat contradictorily added that the most important fact is the degenerative change in the stroma of the villi.
Although not applicable to what I have come to regard as the incipient changes in hydatiform degeneration, it nevertheless is true that the stroma often, if not always, quite early becomes hydatiform — that is, glassy or clear, though not necessarily watery. Moreover, the villous vessels often degenerate or disappear completely at a very early stage. It is exceedingly difficult to make any definite statement as to what is typical regarding the epiithelium. This has been said by others also. Indeed, this necessarily foUows from the fact agreed to by every one, that histologically there is no true line of demarcation between the ordinary benign hydatiform mole, the so-called destructive benign (?) hydatiform mole — whatever its status may be — and the malignant hydatiform mole, or chorio-epitheUoma. Such a conclusion alone presupposes the existence of the widest differences in the condition of the t'pitlu'lium in the these cases, and that such differences actually exist is beyond question.
Marchand's revolutionary investigation on chorio-epithelioma notwithstanding, the epithelium is not always two-layered, nor is it always thickened, in hydatiform mole. That the epithelium can not always be active beyond the normal follows also from the fact that the proliferative changes in it are subsequent to, even if not necessarily conseciuent upon, changes in the stroma. Furthermore, like the latter they are gradual in their evolution and may stop or be stopped at any stage of their development. Then, too, the condition of the epithelium depends very largely upon the preservation of the abortus, and this, as is well known, varies greatly. The most striking thing about the epithelium usually is not its thickness, the presence of large masses of trophoblast, or of numerous syncytial buds, but its splendid state of preservation, especially as contrasted with that of the stroma. This is true of all except macerated or degenerate specimens, for the life of the epithelium seems assured as long as there are periodic accessions of fresh blood, which, as the clinical histories illustrate, usually is the case. The stroma, on the other hand, probably not being wholly independent of the contained capillaries, is deprived very largely of its sustenance during, even if not in consequence of, their degeneration. According to some, hydatiform degeneration of the stroma is the result of an accumulation of nutritive products in consequence of the absence of the vessels. Degeneration of stroma and vessels, however, may result from malnutrition due to poor implantation.


The epithelium of the villi often was found single-layered without any syncytium whatever, or with at most a few syncytial buds. Nevertheless, both the syncytium and trophoblast very often show evidences of a marked activity which is not confined to implanted vilh or to the epithelium of the villi as a whole, but which may extend to that of the chorionic membrane as well. Surprisingly long, complex syncytial buds, whorls and festoons, as shown in figures 22, 23, and 24, and as said to have been observed by Frankel, often are present, especially on the villi, although in a few instances fine buds and frameworks of syncytium also were seen arising from the epithelium of the chorionic membrane. This feature (shown in figure 23) has, I believe, not been specially emphasized heretofore, though observed by Clivio (1908).

Mounds formed by the Langhans layer were common, especially on the tips of the villi where they frequently formed irregular masses of small nodules — the "appendici durate" of Crosti (1895). These gave the villous tree the appearance of a leafless orange loaded with fruit, only that the trophoblastic nodules are mainly apical, as shown in figure 25. In several instances syncytial buds were found far out on these; trophoblastic masses, a fact which is of special, if not of crucial significance in connection with the old question of the origin of the syncytium, for these buds undoubtedly had not been transported tluMc. But however one may regard these things, such appearances as represented in figure 24 are unmistakable, for they show thickenings composed of Langhans cells aiul garlands of considerable length, portions of which are composed of absolutely distinct cells of the Langhans type, as well iis other portions composed of syncytium with every gradation between the two. Nor do I believe that the assumption that syncytium can resolve itself into indiviiduaI cells can be used to deny the implication of these facts.
Although hydatiform villi covered by a single layer of rather small cells of the nature of Langhans cells, sometimes without visible cell boundaries, frequently were seen, villi covered by typical syncytium only never were seen. The single layer present, although syncytial in places, suggested Langhans cells rather than the real syncytium. Moreover, since the cells of the Langhans layer usually were smaller rather than larger than normal, it follows from this alone that their proliferation must have been marked, in order to completely cover the enlarged villus, in spite of the fact that the layer remained single-celled. Were this not the case, the extraordinary increase in size which accompanies the formation of large hydatid cysts could not possibly occur without rupture of the covering layer.


Not infrequently proliferation of the epithelium without increase in thickness may manifest itself in another way. The caliber of the villi in the earlier stages of hydatiform degeneration sometimes does not increase much, no thickening of the proliferating epithelium is noticeable, and yet the latter shows marked proliferation. Under these circumstances, the borders of the villi and of the chorionic epithelium may appear extraordinarily sinuous as illustrated in figure 26, and epithelial invaginations from opposite sides rarely meet in the center, as indicated in figure 27, and by fusion completely isolate a portion of the stroma. It usually is in these cases of very sinuous epithelium that the epithelial invaginations sometimes become constricted, leaving a closed epithelial vesicle or a nodule of epithelium attached to a stalk or wholly isolated within the stroma, as shown in figures 28 and 29. All stages in this process of vesicle formation were found, and rarely also extensions of epithelial sprouts as described by Neumann (1897) and others were seen, portions of which had become isolated in the stroma to appear later as typical syncytial giant cells. These facts, too, would seem to throw a sidelight upon the origin of the syncytium for those to whom this question is still an open one.
All these tilings abundantly testify to the activity on the part of the epithelium in many hydatiform moles, even when thickening of it is absent, but they are of diagnostic value only if present, and I wish to emphasize again that they may be wholly absent or at least unrecognizable in the early stages. Moreover, the degree of epithelial proliferation varies greatly, as illustrated in figures 30, 31, and 32.
Until I am able to learn more about the structure of normal villi in various stages of development, I am not willing to commit myself regarding the incipient changes in hydatiform degeneration. These may be unrecognizable with present methods. However, it is possible to say that in young conceptuses the disappearance of the capillaries, which was regarded as a possible cause for the development of hydatiform mole by Hewitt (1860 and 1861), and also emphasized later by Hahn (1865), Maslowsky (1882), and by others, undoubtedly is a very early and possibly the very earliest noticeable change in some cases. Of course, I do not imply that death of the embryo is the cause of this disappearance, as Hewitt held, and I am not ready to say that the vascular change is the very earliest one in all cases. This would imply that hydatiform degeneration under no circumstances can begin before the capillaries have ai)i)carocl in the villi. There is some evidence which suggests that it possibly may appear before this time. If so, it would be incorrect to speak of a disappearance of the vessels in such chorionic vesicles, for if the advent of hydatiform degeneration can precede the appearance of the villous capillaries, vascularization of the villi ma.v never occur. In older conceptuses, however, in which vascularization of the villi has sujiervened, the first recognizable change is the disappearance of these capillaries. Many specimens in which the latter were in various stages of degeneration were examined carefully, and the opinion of Hewitt (1860), that hydatiform degeneration can not arise in villi which have been vascularized, can be regarded as of historical interest only. Different stages in the process of vascular degeneration are represented in figures 33 to 35 inclusive.
Coincident with the disappearance of the vessels, changes in the stroma also are noticeable. Usually it tends to become glassy, the individual nuclei becoming separated farther. The stroma, though apparently solid, is uniformly slightly bluish and vitreous, with well-defined, rather small, pycnotic, pointed nuclei, but with not a vestige of a vessel, though the epithelium is splendidly preserved. The latter may be one-layered or two-layered, and may be accompanied by syncytial buds and trophoblastic masses and nodules. In such specimens the entire picture really is exquisite, and a mere glance through the compound microscope reveals the lack of vessels in the vitreous stroma and the marked differences in size of the sections of the villi.
After these early changes, licjuefaction of the stroma usually follows. As is well known, liquefaction generally begins in the interior and first appears in the form of vacuolation; but this vacuolation (which I can not regard merely as an edema) is not intra-cellular but intercellular, and as it becomes more pronounced it really takes on the nature of fenestration. Sections of the whole cross-section of the villi, even though large, may be composed of a series of fenestrse (see fig. 36) separated by exceedingly fine strands of the remaining stroma which may contain remnants of the nuclei. But finally, even the fine trabecular separating the fenestras disappear, and the stage of the watery, old, hydatid condition has been reached. More generally, however, the vacuoles or small fenestra lying in the middle become confluent at the center of the cross-section of the villus, which then is liquefied completely. As is well known, this liquefaction gradually extends to the periphery as the zone of the surrounding stroma is narrowed in the process. Not infrequently, however, liquefaction of the stroma occurs quite generally throughout the cross- section of the villus and is accompanied by the formation of numerous large cells, the wandering or migrating cells of earlier writers. A few of these cells almost always can be found, and rarely the whole section of the villus is studded with (fig. 37) or even formed by these large, erratic cells which usually lie in fenestra? in the stroma. In other instances a large portion of the sections of the villi may be occupied by them, as shown in figure 38. The presence of these cells in viUi regarded as normal has long been known. Their presence in hydatiform moles was noted by Otto, Marchand (1895), Essen-Miiller, and by many others. Their occurrence in normal and pathological chorionic vesicles, and their significance are considered more fully by Meyer (1919). No matter what the condition of the epithelium, or more specifically that of the Langhans lajer, the syncytium and trophoblast may be, the above-noted changes in the stroma always are quite typical. They are not the only changes noted, however, and their advent may differ somewhat.
Not infrequently, changes quite comparable to those in the villi occur also in the stroma of the chorionic membrane itself, a fact which has not heretofore been emphasized. Also, it is frequently decidedly glassy; liquefaction may occur here and there and may become complete in the course of time. Hofbauer cells not uncommonly also are present. Among the changes noted in this membrane the disappearance of the vessels is most common and constant, although epithelial proliferation is not rare, as already stated. Moreover, when (as in one of Storch's cases) a hydatiform villus is 15 cm. long, one scarcely can doubt that the stroma also must have proliferated — not merely degenerated. Some of the strings of hydatid cysts in a specimen in the Mall Collection have a length of over 10 to 12 cm., and in these cases also one can hardly assume that this increased length in the villi was unaccompanied by prohferation of the stroma. From these things alone it follows that the stroma can not remain passive always, although Gromadzki (1913) concluded that the stroma never proliferates. Vecchi (1906), however, reported an increase in the stroma of the vilU, and it will be recalled that Marchand also implied the presence of proliferative changes in the connective tissue when he wrote that they depend on those in the epithelium.
I have never been able to find mitotic figures, a fact which may be accounted for, however, by the presence of degenerative changes due to intrauterine separation and retention of most specimens. Indeed, the failure to find mitoses speaks against proliferation in the stroma no more than in case of the epithelium, in which the presence of karyokinetic figures has been reported by a few investigators only. Yet pronounced proliferation of the epithelium often is present. The failure to find mitotic figures is very likely due to the condition of the material.
Careful scrutiny of a large series of specimens has revealed the fact that the disappearance of the vessels in the villi, in the chorionic membrane, and also in the umbiUcal cord is centripetal as a rule. However, in many specimens the vessels not only may be present in the chorionic membrane although absent in the villi, but may be very numerous and even engorged with blood. It is difficult to say to what extent the engorged condition of these vessels and of those in the body of the abnormal embryos sometimes contained in these hydatiform moles is due to the propulsion of the embryonic blood before the advancing vascular constriction and degeneration, but I am inclined to beUeve that the centripetal movement of the process is not a negligible factor.
Although only a few instances of the birth of a living fetus or of a fetus which had reached the later months of pregnancy are recorded in the literature, it now is quite generaUy recognized that the fetus, though dead and too small for its menstrual age, usually is present. This stands in contradiction to the earlier belief iUustrated by the statement of Gierse (1847), that the fetus usually was reported as absent, and that when present (as in the cases of Meckel, Gregorini, Otto, Cruveilhier, and his own) it usually was less tihan 1 inch long, even when retained for a period of from 3 to 10 months.
This apparent contradiction regarding the presence of the fetus in hydatiform moles is explained easily by the fact that the cases in the earlier literature are old, far advanced in degeneration, while the more recent literature contains many more in the earlier stages of degeneration. Yet in spite of this fact the earlier opinion survives to the present day, for Graves (1909-10) spoke of "the very unusual presence of a normal fetus inside a mole," and Vineberg (1911) still more strangely held that the presence of a fetus excludes the specimen from the class of true hydatiform moles!
Among the specimens concerned in this report many contained a fetus. Tliis was true of 24.5 per cent of 49 tubal and 64.4 per cent of 121 uterine specimens, including some (9) doubtful cases. In some early specimens the fetus is in a state of excellent preservation. This is what one might expect, for the onset of hydatiform degeneration is gradual and often partial. The condition of the fetus in many of them alone also suggests that its death was secondary to the degeneration.
The fetal length ranges from 1 to 90 mm. in the uterine and from 1 to 80 mm. in the tubal series. Although the average length of the embryo in the tubal series is 12.3 mm., and that of the uterine only 10.1 mm., 58 per cent of the tuljal speci- mens nevertheless were below 7 mm. in length as contrasted with 52.5 per cent of the uterine.
The presence of a fetus with a frequency almost three times as great in the uterine series again indicates that the abnormal conditions within the tubes lead to early death, digestion, and absorption, or at least to dissolution, of the embryo. This fact again points directly to a faulty nidus as causative agent, for if the absence of a fetus is to be laid to primary ovular defects, then one must admit that relatively far more of such diseased ova become implanted within the tube than within the uterus.
Of the many explanations which have been offered for the advent of hydatiform degeneration, none seems to be better established than that of endometritis. Tliis was first emphasized by Virchow (1863), and Lwow (1892) also reported 4 cases in patients under his care in whom lues could be excluded but in whom he held endometritis responsible. Emanuel (1895) was the first, it seems, to demonstrate the presence of cocci in inflammatory foci of round cells in the decidua accompanying a case of hydatiform mole. Veit (1899) also believed that disease of the decidua is the cause of hydatiform degeneration. Veit further stated that Waldeyer, Jarotzky, and Storch also believed that an irritative condition of the decidua is responsible. Stoffel (1905) also found cocci other than gonococci present and says he can not avoid holding endometritis responsible in his case. The association of hydatiform degeneration and endometritis was noted also l)y INIarchand (1895), Oster (1904), and Sternberg; also by Essen-Mollor, who reported the phenomenal case of a woman with endometritis, who had aborted a hydatiform mole 18 times in 9 years. Falgf)wski, on the contrary, concluded that the ova themselves were diseased and argued that hydatiform degeneration should be much more common if it were due to endometritis. Taussig (1911) also stated that leucocytic infiltration of the decidua is frequently present in hydatiform moles, but iasistcd that "leucocytic infiltration in the placenta then should not be interpreted as infection.
- Inflammation and infection should be kept apart." I presume Taussig really meant infiltration and infection should be kept apart, and the question then turns upon the structure of the normal decidua and the significance of infiltration for the development of the ovum.
It may be recalled that Marchand (1904) reported the presence of isolated groups of small cells in the normal decidua which looked hke mononuclears under low magnification, and which he believed often have been confused with them. But even granting this, and the further facts that the exact histologic changes in the decidua are not fully known, and that it is rather difficult to ascertain just what decidual changes are regarded as evidence of the existence of an endometritis, any one examining a large series of cases of hydatiform degeneration aborted with the decidua can not doubt the presence of marked decidual changes in a very large percentage of them. These changes are not limited to infiltration with scattered round cells or erythrocytes, or to focal accumulation of the same, but often extend to almost complete fibrosis, as shown in figure 39, so that experienced investigators have mistaken the thin, fibrous decidua for a part of the chorionic membrane.
It is true that the existence of these changes in the deciduae themselves does not necessarily imply that they were antecedent to the implantation of the ovum, but fortunately' the clinical histories and material from curettage often supply crucial evidence. From such cases and from the cumulative weight of evidence from the large series of cases here reported, the great majority of which showed decidual infiltration or other changes suggestive of endometritis, the frequent association of abnormal deciduae with hydatiform degenerations is evident. The fact that the incidence of hydatiform degeneration in the tubal was somewhat higher than that in the uterine series might be regarded as contradicting this relationship, but such is not the case. The mucosa of the tubes at best is an unfavorable nidus for implantation because of the absence of decidual formation alone. Hence, even if salpingitis were somewhat less frequent than endometritis, proper nidification in the tube could easily more than account for the existing differences. Hence the higher incidence of hydatiform degeneration in the tubal series in fact becomes confirmatory of the conclusion that abnormal nidification really may be responsible for the advent of hydatiform degeneration.
The only fact which might be interpreted as indicating that germinal defects primarily are responsible for the development of hydatiform degeneration is the relatively higher incidence of the condition in older women. Against this, however, stands the other fact that such women also show the cumulative effects upon the endometrium of age, endometritis and pregnancy. Furthermore, since hydatiform degeneration so often follows one or two normal births or abortions, it would be impossible to find an adequate explanation for the release of the defective ova so often after and not before these events.
I am reminded also in this connection of a case the detailed history of which is fully known. It is that of a robust young woman who successively gave birth to two moles and then to a normal full-term child and secundincs. In this case curettage was done in connection with each mole. Apparently the new endometrium, which had formed after the second abortion and curettage, permitted normal implantation and normal development to progress to term. To ignore the condition of the endometrium in this case and attribute the development of hydatiform degeneration to the successive release of abnormal ova would seem to disregard important facts — especially so since no one has established the occurrence of abnormal ova within the Graafian foUicle, a possibility which I do not wish to deny, although Donskoj 's report of a case of hereditary mole must surely be taken cum grano sails (with a grain of salt).
That an abnormal nidus may be responsible for the advent of hydatiform degeneration would seem to be indicated also by the fact that the process usually was better developed and more general in the tubal than in the uterine cases. That both endometrium and decidua show astonishing differences in structure under pathological conditions is well known. The entire tubal mucosa, on the other hand, even when normal, forms an abnormal nidus which would affect all portions of early chorionic vesicles somewhat alike, and since, as found by Mall, inflammatory conditions in the tubes predispose to tubal imjilantation, the higher incidence of hydatiform degeneration in the tubes is easily explained. Nor does the existence of partial hydatiform degeneration argue against such an explanation.
Although Kehrer reported not a single fatality in 50 cases of hydatiform mole, Hirtzman (according to von Winckel) gave the fataUty as 13 per cent, Borland and Gerson as 18, and Williamson as 20 to 30 per cent. Von Winckel (1904) regarded these i)ercentages as entirely too high, however, although Oster reported 2 cases of malignancy out of 15 among cases in which the late results were ascertainable — an incidence of 13.3 per cent. Kroemer (1907) found that chorio-epithelioma developed in 5 out of 15 cases of hydatiform moles, or in 33.3 per cent, but only twice in 3,841 "normal implantations." Daels (1908) says La Torre claimed a malignancy of 64 per cent; de 8enarcleus one of 28.7 per cent, or 14 out of 49 cases. Frjienkel (1910) emphasized that the estimates of the number of cases in which hydatiform degeneration is followed by malignant disease vary greatly, while Robertson (1915) quoted Findley as finding that IG per cent of 250 hydatiform moles collected from the literature were followed by malignant disease. Briggs, who reported 21 cases of hydatiform degeneration with 2 of chorio-epithelioma or an incidence of malignancy of 9.5 per cent, called attention to the "diminishing ratio in the; tendency to malignancy shown by his series."
Findley stated that chorio-epithehoma develoiH'd in 131 out of 500 cases gathered by him from the literature, which is an incidence of 26.2 per cent; but, as already stated, most of these cases from the hterature are old, advanced degenerations, many of which have been retained for a long time. The tendency to malignancy in these probably can in no way be compared to that in smaller and younger specimens, many of which are aborted entire with the surrounding decidua. Consequently, it need not surprise us that out of 19 cases of this series, in which later reports were obtainable, none were reported as having developed chorio- epithelioma.
Perhaps I may here add a word of caution, however, in regard to a possible change in attitude toward the question of malignancy with a consequent relaxation of vigilance. It is true that out of the 21 cases of Briggs only 2 developed chorio- epithelioma, but it must not be forgotten that Briggs in part was, and I to a far larger extent, am dealing with a different class of hydatiform moles than those upon a study of which the prevailing conception of malignancy is based. Hydatiform moles which continue to grow and which survive for months after the death of the embryo evidently are more vigorous, and hence no doubt also more dangerous than those which are aborted early and spontaneously. Since the latter formed the great majority of all moles here considered, opinions regarding malignancy formed on this basis probably would lead to disaster if applied in practice. Such conceptions would be based upon a totally different incidence than the current one of 1 hydatiform mole in every 2,000 cases. Instead of relaxing our vigilance it would seem wise to increase it, particularly in the cases of so-called spontaneous abortions — the cases in which no ascertainable cause for the termination of pregnancy can be found, especially if the chorionic vesicle is empty or if the embr^^o belongs in one of the early groups of Mall's classification.
The average age of 36 women aborting hydatiform moles was 31 years. Although I do not regard the alleged ages as necessarily the actual ones, this average age agrees very well with that of 6 cases reported by Poten, 10 by Donskoj, 23 by Briggs, 6 by Gromadski, and 8 by Robertson. The average age of Poten's cases was 32 years, of Donskoj 's 25 years, of Briggs's 28 years, of Gromadski's 29.6 years, and of Robertson's 28.4 years. Pazzi (1908) , on the other hand, stated that Briquel placed the greatest frequency of hydatiform degeneration between 20 and 30 years. These averages are so far on the near side of the menopause that one can make liberal allowances for the proverbial disinclination of women to state their exact age, even to physicians, and nevertheless regard the prevailing opinion undoubtedly as ill-founded. If, as Lewis (1906) stated, it is necessary to add only half a year to the average age of a large group of women in order to ascertain the actual average age when considering general social statistics, then everyone will admit that still less allowance than this need be made in the case of women who are speaking to their physicians, knowing that whatever they may say will be regarded as strictly confidential. That it is unncessary to make large allowances for under-statement of their age on the part of these women is indicated also by the average duration of their married life before aborting moles. This in the case of 29 women was 7.1 j'-ears. Hence, if one bears in mind that the average age of first marriages according to Webb (1911) is 25.1 years, one can easily see that the average age of the women aborting hydatiform moles, which was given as 29.6 years, is probably not too low at all, thus confirming the findings of Williamson, who denied that hydatiform mole was especially common near the menopause.
The conclusion that the average age of 29.6 years undoubtedly is near the actual is confirmed also by the fact that a hydatiform mole was the first abortion in 19 out of 41 women, or almost half the number; 12, or almost one-third, had aborted twice, and only 10 had aborted more than twice. But what is still more confirmatory is the existence of a surprising parallelism between the data on abortion and those on births; 9 of 33 women had given birth to but 1 child, and an eriual number had given birth to but 2. Hence over 50 per cent of the 33 women had borne children twice, or less than twice, and only 15, or less than half, had borne oftener than this.
This undoubted evidence of the youth of these women is confirmed still further by the statement of Lewis who, from an analysis of 16,325 first births, found that nearly one-half of them occur between the ages of 20 and 24, almost three-fourths between 20 and 29 years, and that first births are more frequent between 30 and 40 than between 15 and 19 years. I realize, to be sure, that social statistics can not be translated from one country to another without modification, but in such a mixed population as ours this modification probably need be less (rather than greater) than in case of some countries.
The conclusion that the occurrence of but a single birth before the advent of hydatiform degeneration probably implies that such women are relatively young is emphasized still further by the statement of Lewis that in one-third of the marriages in Scotland "the bride had a child when unmarried or was pregnant at the time of marriage," and that 50 per cent of the first births in Scotland occur within 9 to 24 months after marriage. Lewis also gives the average interval between marriage and the first birth in 16,176 first births as 13.54 months, but little more than one year. Since Lewis stated that the interval between the birth of the first and that of the second child is but little longer than that between marriage and the birth of the first child, being only 3.07 years, it is evident that not even those women who had borne two children before the advent of hydatiform degeneration could have been near the menopause. This conclusion is emphasized still further by the fact that in 96.12 per cent of 16,176 fruitful marriages fertility was demonstrated within three years after marriage.
Nevertheless, in spite of the clear implication of all these facts, I wish to emphasize again that since what have been heretofore regarded as hydatiform degenerations were large specimens mainly, it well may be, and according to certain authors it is true, that such cases occur later in the reproductive life of women. Yet it certainly is significant that Findley in tabulating 500 of such cases from the literature found that 275, or 55 per cent, occurred before the thirty-fifth year, and of 36 specimens from the Mall Collection 23, or 63.6 per cent, came from women below this age. It may also be recalled that 78 per cent of Kehrer's 50 cases and 90 per cent of Bloch's occurred before the fourth decade.
Fourteen out of 23 cases, or 61.3 per cent of the uterine series, in which the age was given, occurred at or before the thirtieth year, and 18 out of 23, or approximately 80 per cent, at or before the thirty-fifth year. These things abundantly emphasize the conclusion reached by some investigators that hydatiform mole is not absolutely more common at or near the menopause. But it nevertheless may be relatively more common. That is, the number of hydatiform moles aborted after 40 com.pared with the total number of pregnancies or births after 40, actually may be greater than this ratio before 40 years.
From calculations based on data given by Lewis the average number of births occurring after 40 years in Sweden, Norway, Denmark, Brunswick, Berlin, Buda Pesth, France, and Scotland is 9.9 per cent. This agrees remarkably well with Bloch's estimate of 10 per cent. But if 77.2 per cent of the cases of hydatiform mole occur below 40, and 22.8 per cent after that year, then it is evident that hydatiform mole nevertheless is relatively more common after than before 40 years, for approximately one-fourth of the cases of hydatiform degeneration would be associated with one-tenth of the births. This would be an increased frequency of 300 per cent above that before 40 years. A similar result would be obtained by comparing Findley's or Williamson's series. Hence, hydatiform degeneration though absolutely loss is relatively more frequent in later life. This fact, however, does not necessarily imply that age in itself is responsible for the increased incidence after 40. A comparison of the incidences of hydatiform degeneration in young and old primiparse, of good health, might elucidate this question.
These statistics are not in agreement with the prevailing opinion that hydatiform moles are more common in multipara; than in primiparfe. Indeed, as I under- stand, they suggest rather that after the first conception, which was normal in a large percentage of these young women, something happened which interfered with the normal development of succeeding conceptions. That, it seems to me, is extremely significant and very suggestive. Here is a group of relatively young women, over 50 per cent of whom had borne but twice and some only once, and then gave birth to a hydatiform mole. While I realize the necessity for circumspection, especially in these matters, these facts seem to me to suggest that something hap- pened to a normal endometrium. Other facts also point in the same direction.
Even if it is not wholly correct, as Findley states, that more cases of hydatiform mole were reported in the last decade than in the previous 14 centuries, it is not unlikely that approximately as many specimens of this condition are contained in the Mall Collection as have been reported heretofore. Moreover, upon the basis of the present rate of accession, a large number of formerly unrecognized cases of hydatiform moles — both tubal and uterine — are donated to this collection annually. This fact, together with others to which attention has been called, ought to stimulate our interest in this problem.
Bibliography
Aman, J. A., 1916. VhcT (lestruirende Blasenmolc. Monatschr. f. Geb. u. Gyn., Bd. 34.
Ballantyn'e, J. W., and James Young, 1913. Fatal case of hydatiform mole. Obst. Trans. Edin., 38.
Bloch, 1S69. Die Blasenmole. Inaug. Dis.s., Freiburg.
Brioos, H., 1912. On the relative ahe of the uterus in cases of hydatid mole with illustrative cases and specimens. Jour. Obst. and Gyn., British Emp., London, 21.
Clivio, I., 1908. A proposito di un cjiso di mola vescicolare iniziale. Folia Ginaecologia, i, Fasc. Primo.
Croom, J. IIalliday, 1895. Two cases of extra-uterine gestation operated ujion at the fourth month. Edin. Med. Jour., 40, part 2.
Crosti, G., 1895. Contribuzione alio studio dell' aborto di origine ovulaire. Atti dall assoziazione medica Lombardo, No. 3. Rev. in Centralbl. f. Gyn., Bd. 20, 1896.
Daels, F., 1908. Au sujet de I'^tiologic do la mole hydatique. Ann. Soe. de med. de Gand.
De Lee, J. B., 1915. The principles and practice of obstetrics. Philadelphia.
DoN-SKOJ, DiMiTRY, 1911. Beitrage zur Kenntniss der Blasenmole. I. D., Miinchen.
DoRLAND and Gerson, 1896. Cystic disease of the chorion, with a tabulation of one hundred cases. Unvi. Med. Mag., vol. 8.
Durante, G., 1898. Varietes, histologic et nature de la mole hydatid. Arch, de med. exper. , 1909. Lesions des vaisseaux fa>taux dans le mole hydatiforme (nature et pathologic de la mole). Gynec, Par. I, 13.
Emanuel, R., 1895. Demonstration zur Lehre von der Endometritis in der Schwangerschaft. Zeitschr. f. Geb, u. Gyn., Bd. 31.
EssEN-MoLLER, Elis, 1912. Studien iiber die Bla.senmole. Wiesbaden.
Falgow.ski, W., 1911. Kritische Wiirdigung eines
Falles von Blasenmole bei ZvvilUngsschwangerschaft mit einem ausgetragenen Kind. Monatschr. f. Geb. u. Gyn., Bd., 34.
Fellner, O. O., 1903. Ueber periphere Langhanszellen, zugleioh eine Erwiederung auf den Aufsatz von R. Meyer: "Zur Kenntniss der benignen Chorio-epithelialen Zellinvasion." Zeitschr. f. Geb. u. Gyn., Bd. 21.
FiNDLEY, P., 1917. Hydatiform mole; an analysis of 500 cases. Amer. Jour. Obst., 75.
Fraenkel, L., 1910. Ruckbildung von Ovarialtumoren nach Blasenmole. Monatschr. f. Geb. u. Gyn., Bd. 32.
Freund, W. a., 1889. (No title.) See "Berichte uber die Verhandlungen der gynakologischen Sektion der 62 Versammlung deutscher Naturforschcr und Arzte zu Heidelberg," 1889. (A reference to the case only.) Centralbl. f. Gyn., Jahr. 13, p. 690.
Gierse, Aucju.st, 1847. Ueber die Krankheiten des Eies und der Placenta. Verhandlung der Gcsell-Bch. f. Gebh., Berlin, Bd. 2.
Chaves, E. W. IL, 1909-10. A specimen of tubal mole. Proc. Roy. Soc. Med., London, 3, Obst. and Gyn. sec. 1.
V. Gromadzki, IIrinhich, 1913. Ein Beitrag zur Lehn' von der Blasenmole mit besonderer Beriicksichtigung deren Pathogenese. Inaug. Diss., Halle.
Hahn, C. F. O., 1865. Ueber ein cystcnnrtiges Gebilde im NabelstrangeinerTraubcnmole Monatschr. f. Gebk. u. Frauenkrankh., Bd. 26. Hennig, Carl, 1876. Die Krankheiten der Eileiter und die Tubenschwangerschaft. Stuttgart.
Hewitt, Graily, 1860. On the hydatiform or vesicular mole; its nature and mode of origin. Obst. Trans., 1, London. , 1861. Hydatiform degeneration of the ovum. Obst. Trans. London, 2.
HiEss, Viktor, 1914. Ein Beitrag zur Pathologie und Klinik der Blasenmole. Gynak. Rundschau, Berlin u. Wien, Jalu-. 8.
Hirtzman, 1874. Mentioned by Seitz, 1904. Thfese, Paris.
Kehrer, F. a., 1894. Ueber Traubenmole. Arch. f. Gyn., Bd. 45.
Kroemer, p., 1907. Klinische Beobachtungen iiber Etiologie und Therapie des ChorionepitheUom insbesondere uber die Behandlung der Blasenmole. Deutsche med. Wochenschr., Jahr. 33, 2.
Krueger, M., 1909. Eine seltene Form der Placentarcy.ste; ein Beitrag zur Lehre von der Blasen-mole. Zeitschr. f. Geb. u. Gyn., Bd. 64, H. 2.
Lewis, C. J. and J. N., 1906. NataUty and fecundity. London. Lwow, J. M., 1892. Mola vesiculosa. Centralbl. f. Gyn., Jahr. 16.
Mall, F. P., 1915. On the fate of the human embryo in tubal pregnancy. Contributions to Embryology, I, Carnegie Institution of Washington.
— , 1917. On the frequency of localized anom.alies in human embryos and infants at birth. Amer. Jour. Anat., 22.
Marchand, Franz, 1895. Ueber den Bau der Bhisenmolen. Monatschr. for Geb. u. Gyn., Bd. 32. , 1898. Ueber diis maligne Chorio-epithelium. Zeitschr. for Geb. u. Gyn., Bd. 39. , 1904. Beitrag zur Kenntniss der normalen und pathologischen Histologic der Decidua. Arch. f. Gyn., Bd. 72.
Maslowski, 1882. Zur pathologischen Anatomie der Traubenmole. Centralbl. f. Gyn., No. 10.
Matwejew, G. F., and W. M. Sykow, 1901. Blasen-mole in <ler Tuba Fallopii und cystische Degeneration des Ovariums. .Sitzngsb. der Mosk. gj'n. GeselLsch. \\'iatseh., No. 24. (Rev. in Zentralbl. f. Gyn., Bd. 26, 1901.)
Maxwell, R. D., 1910. Tubal mole with edema of the connective tissue of the villi. Proc. Roj-al Soc. Med., London, 3, Sect. Obst. and Gyn.
Mayer, Karl, 1911. Retention von Blasenmolen. Med. klin. lierlin Jahr. 7, Th. 2. Menu, Adolphe, 1S99. La mole vfisiculairc. Tumeur maligne. Thfee, Paris.
Meyer, A. W., 1919. On the nature, occurrence and identity of the plasma cells of Hofbauer. Jr. Morph., vol. 32.
MucGiA, ViRoiNio, 1915. Contributo alio studio della parziale degenerazione vesicolare partiale della placenta Folia gynec, Pavia, T. 2.
MfTLLER, H., 1847. Bau der Molen. Wurzburg. Neumann, Julius, 1897. Ueber Blasenmole und maligne Deciduom. Monatschr. f. Geb. u. Gyn., Bd. 6.
Niosi, Francesco, 1905. Corioncpitelioma maligno, primitivo, bilaterale dell' ovaia, non embrio- matoso, indipendente da gravidanza e con incipiente formazione di vescicole raolari. Atti della Societa Italiana di Ostetricia e Ginecologia, 11. Roma, 1900.
OsTEB, Karl R., 1904. Uber das spiitere Befinden der Frauen nach Gebiirt einer Blasenmole. H. Fiencke, Kiel.
Otto, Heinrich, 1871. Ueber Tubcnschwangerschaft mit Beriicksichtigung eines Falles von Graviditas tubaria molaris hydatidosa. Inaug. Dissert, Greifswald.
Panttm, p. L., 18G0. Untersuchungen uber die Entstehung der Missbildungen zunachst in den Eiern der Vogel. Berlin.
Pazzi, M., 1908'. Vescicole molari iniziali. Folia Ginecologia, 1, Fasc. Terzo. , 1908'. Vescicole molari iniziali e nouva orientazione della teoria patogenetica della mole vescicolare e del corionepitelioma. Folia Gynaecologia, 1, Fasc. 3. • , 1908^. La Nostre cognizioni intorno alia mola vescicolare ed alia nidificazione del-l'uovo. Rassegna D'Ostetricia e Ginecologia, 17. , 1909. Note di patologia sperimentale e di istologica patologiea intorno alia mola vescicolare e considerazioni relative. La Ginecologia Moderna, 2, Fasc. 2.
Pearson, K., 1897. The chances of death and other studies in evolution. London.
PoTEN, W., 1901. Beitrag zur Diagnose der Blasenmolen Schwangerschaft. Monatschr. f. Geb. u. Gyn., Bd. 14. V. Recklinghausen, 1889. Perforierende Blasenmole bei fiinfwochentUcher Tubenschwangerschaft. Deutsch med. Wochenschr. (Merely a society minute.)
RiSEL, W., 1895. Demonstration von frischen Praparaten nebst Bemerkungen. Gesellsch. f. Geb. zu Leipzig, June 17. (As reported in Zentralbl. f. Gyn. 1896.)
Robertson, J. F., 1915. Hydatiform mole; a report of eight cases. N. Y. Med. Jour., 102.
Seitz, L. 1904. Erkrankungen der Placenta. Kap. iii, Handb. der Geb. F. von Winckel, Bd. 2, Wiesbaden.
Sfameni, p., 1905. Sulla natura esclusivamente epitheliale delle vescicole nella mola idatigena. Ann. di ostet., Milano, T. 27.
Sternberg, Martin, 1910. Ueber sogennante Fleisch- Blasen-Molen mit lingerer Verhaltung im Uterus. 1. D., BerUn.
DE Snoo, K., 1914. Bijdrage tot de anatomic en de aetiologie der blaasmola. Nederlandsch Tijdschrift voor Verloskunde en Gynaecologie, 23, p. 56.
Stoffel, A., 1905. Untersuchungsergebnisse eincs Friistadium von Blasenmole; zugleieh ein Beitrag 7ur Aetiologie derselben. Monatschr. f. Gyn. u. Gebh., Bd. 21.
Storch, E. D., 1878. Beitrag zur pathologic des Eies. Falle von sogenannter partiellem Myom der Placenta. Arch. f. path. Anat., Bd. 72.
Taussig, F. J., 1911. Hydatiform mole of unusual type. Weekly Bull. St. Louis Med. Soc, 5.
Teacher, J. IL, 190.3. On chorioepithelioma (the so-called deciduoma malignum), and the occurrence of chorioepithelioma and hydatiform-mole-like structures in tumors of the testes. London Obst. Trans., 45.
Van der Hoeven, 1900. Ueber die Etiologie der Mole hydatidosa. Arch. f. Gyn., Bd. 62.
Vecchi, Mario, 1906. Di una particolare alterazione di sviluppo die viUi coriaU. Note anatomiche per lo studio della mola vescicolare. Raccolta di scritti ostelrico-ginecologici pel Giubileo Didattico del Prof. Senatore Luigi Mangialh. Pavia.
Veit, J., 1899. Das Deciduom malignum. Blasemnole und ihr Verhiiltnis zum Deciduom. Handb. der Gynak., Bd. Ill', Wiesbaden.
, 1908. Das maligne chorioepitheliom. Handb. der Gyn., Bd. 3, Zweite Hiilfte, Wiesbaden.
Vineberg, Hiram V., 1911. Hj'datid mole. Amer. Jour. Obst., 64.
Virchow, R., 1863. Die krankhaften Geschiilste, Berlin.
Webb, A. D., 1911. New dictionary of statistics, London.
Weber, Samuel L. 1892. Remarks on the differential diagnosis and treatment of cystic degeneration of the chorion. Amer. Jour. Obst.
Wenzel, Carl, 1893. Alte Erfahrungen im Lichte der neuen Zeit und ihre Anschauungen iiber die Entstehung von Krankheiten. 1 Blasenmole Eileiter, Wiesbaden.
Werth, R., 1904. Die Extrauterineschwangerschaft. Kap. I, Handb. der Geb. F. von Winckel, Bd. II, Wiesbaden.
Williams, J. W., 1917. Obstetrics. New York and London.
Williamson, 1900. The pathology and symptoms of hydatiform degeneration of the chorion. Trans. London Obst. Soc, 41.
voN Winckel, 1904. Handbuch der Geburtshilfe, Wiesbaden.
Winter, George, 1907. Lehrbuch der gynakologischen Diagnostik. Leipzig Dritte Auflage.
List of Illustrations
Links: Plate 1 | Plate 2 | Plate 3 | Plate 4 | Plate 5 | Plate 6 | Contribution No.40 | Volume IX | Contributions to Embryology
Plate 1

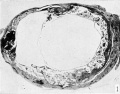
Fig. 1. Cross-section of twin hydatiform chorionic vesicles within the tube. (Specimen No. 825.) X3.

Fig. 2. Hydatiform villi from same specimen in section. X 45.

Fig. 3. Embryo No. 1771, covered with magma. X 4.

Fig. 4. Cross-section of tube No. 1771. X 2.

Fig. 5. Cross-section of tube from same case. X 4.

Fig. 6. Hydatiform villi from same case. X 45.

Fig. 7. Hydatiform chorionic vesicle in loco with the tube incised. No. 2052. X 2.
Plate 2


Fig. 8. Gross appearance of specimen No. 70.

Fig. 9. Gross appearance of specimen No. 323.

Fig. 10. Gross appearance of specimen No. 749. X 1.1.

Fig. 11. Gross appearance of specimen No. 1323. X 1.2.

Fig. 12. Gross appearance of specimen No. 1325. X 12.

Fig. 13. Grass appearance of specimen No. 1914. X i
Plate 3


Fig. 14

Fig. 15

Fig. 16
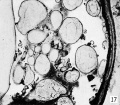
Fig. 17

Fig. 18

Fig. 19
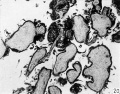
Fig. 20
Plate 4

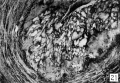
Fig. 21
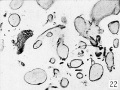
Fig. 22

Fig. 23

Fig. 24
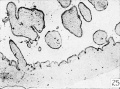
Fig. 25

Fig. 26

Fig. 27

Plate 5

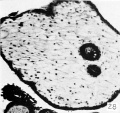
Fig. 28

Fig. 29
- Meyer1920 fig30.jpg
Fig. 30
- Meyer1920 fig31.jpg
Fig. 31
- Meyer1920 fig32.jpg
Fig. 32
- Meyer1920 fig33.jpg
Fig. 33


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Plate 6

Fig. 1. Cross-section of twin hydatiform chorionic vesicles within the tube. (Specimen No. 825.) X3.
Fig. 2. Hydatiform villi from same specimen in section. X 45.
Fig. 3. Embryo No. 1771, covered with magma. X 4.
Fig. 4. Cross-section of tube No. 1771. X 2.
Fig. 5. Cross-section of tube from same case. X 4.
Fig. 6. Hydatiform villi from same case. X 45.
Fig. 7. Hydatiform chorionic vesicle in loco with the tube incised. No. 2052. X 2.
Fig. 8. Gross appearance of specimen No. 70. X1.6.
Fig. 9. Gross appearance of specimen No. 323. X 1.75.
Fig. 10. Gross appearance of specimen No. 749. X 1.1.
Fig. 11. Gross appearance of specimen No. 1323. X 1.2.
Fig. 12. Gross appearance of specimen No. 1325. X 12.
Fig. 13. Grass appearance of specimen No. 1914. X i
Fig. 14. External appearance of the larger part of the small mass of specimen No. 1926. X 4.
Fig. 15. Embryonic (cyemic) mass accompanying No. 1926. X 4.
Fig. 16. A small portion of specimen No. 1189 still in Inco. X 6.
Fig. 17. Another portion of the same specimen. X 30.
Fig. 18. No. 2077, an apparently normal specimen, partly surrounded by decidua. Natural size.
Fig. 19. A portion of the above clearly showing numerous typical hydatid cysts in area in focus. X 3.
Fig. 20. Sections of villi from specimen No. 690. X 50.
Fig. 21. A portion of specimen No. 865 still embedded within the uteras. X 4, reduced J.
Fig. 22. A portion of specimen No. 435", showing a small villus in mid-portion of the figure, which has an exceptionally long syncytial bud. X 50.
Fig. 23. A small portion of specimen No. 962", showing a framework of epitheUum arising from the chorionic membrane. X 50.
Fig. 24. Vacuolated masses of syncytium, nodules of trophoblast, and especially garlands com- posed in part of distinct cells of the Langhans type. Specimen No. 1324. X 300.
Fig. 25. An apical trophoblastic nodule from specimen No. 516. X 6.
Fig. 26. A portion of the chorionic membrane from No. 714, showing corrugation of the proliferating epithelium. X 50.
Fig. 27. A hydatid villus illustrating epithelial constrictions between successive portions. Specimen No. 714. X 50.
Fig. 28. Epithelial vesicles within the stroma. Specimen No. 872. X ISO.
Fig. 29. Extremity of an epithelial vesicle. Specimen No. 872. X 300.
Fig. 30. Marked syncytial budding and epithelial proliferation in specimen No. 874*. X 50.
Fig. 31. Very slight epithelial proliferation in specimen No. 134. X 50.
Fig. 32. Extremely marked epithelial proliferation on a small, glassy villus from specimen No. 415. X 95
Fig. 33. Disappearing capillaries represented by large, incomplete curved outlines. Specimen No. 749. X 50
Fig. 34. Collapsed capillaries in process of degeneration. Specimen No. 712. X 95.
Fig. 35. The degenerating capillaries show as faint lines only. Specimen No. 651g. X 50.
Fig. 36. Fenestrated hydatiform villi among others that are quite fibrous. Specimen No. 651d. X 50.
Fic. 37. A section of villus from No. 510, showing scattered Hofbauer cells. X 300.
Fig. 38. A small portion of a villus from No. 749, showing an accumulation of Hofbauer cells. X 300.
Fig. 39. A portion of a rather fibrous decidua. Specimen No. 874". X 300.
| Historic Disclaimer - information about historic embryology pages |
|---|
|
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, April 28) Embryology Book - Contributions to Embryology Carnegie Institution No.40. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Book_-_Contributions_to_Embryology_Carnegie_Institution_No.40
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G