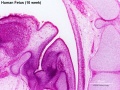
Fetal Development

Fetal oral cavity (week 12)
The Embryonic period involved transient structures to establish body and placental tissues, folding and form. The long human Fetal period (4x the embryonic period) is a time of extensive growth in size and mass as well as ongoing differentiation of organ systems established in the embryonic period. (More? See Fetal Notes)
As many students are new to embryology the majority of the practical class time has been spent introducing general concepts of early human development and combining this with the early formation of GIT structures. While the fetal period is substantially longer, there will be much less content to be covered.
Fetal developmental features include: the growth and rotation of intestines initially herniated outside the ventral body wall; changes in mesenteries; development of the blood supply and tract wall.
Finally consider the initial functions of the tract with amionic fluid swallowing and the accumulation of both secretions and swallowed components within the large intestine as meconium.
Early Fetus
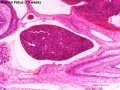
Midgut herniation (label)
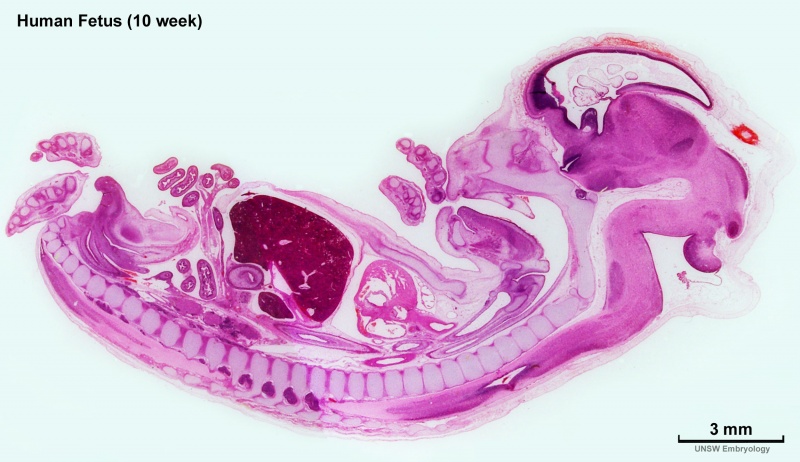
Begin by just looking at the fetal anatomy in sections taken through the above female fetus 10 week (GA week 12), approximately CRL 40 mm in size) and see how this compares with what you already know of adult GIT anatomy.
Related Images
Fetus (week 10) Planes A (most lateral), B (lateral), C (medial) and D (midline) from lateral towards the midline.
- Image Source: UNSW Embryology, no reproduction without permission.
There are 4 sections taken in the parasagittal and sagittal plane (moving from the right at Plane A towards the midline at Plane D). Click on the small images (or the text below) to open the linked large image pages.
Midgut Herniation
In the week 10 fetus (right) the midgut is still herniated (lying outside the ventral body wall) at the umbilicus. We saw in earlier pages that this heriation began back in the embryonic period (week 5) and the initial loop undergoes a series of rotations through embryonic and early fetal periods which position the midgut in its correct adult anatomical locations. These rotations are around the superior mesenteric artery (which supplies this region) and the associated mesentry. (Note this rotation is complicated and explained differently in different texts)
One week later (week 11) continued fetal body wall growth (and other factors) returns the midgut herniation returns to the abdominal cavity.
Small intestine growth in length is initially linear (first half pregnancy to 32 cm CRL), followed by rapid growth in the last 15 weeks doubling the overall length to term. Growth continues postnatally but after 1 year slows again to a linear increase to adulthood. (More? Intestine Development)
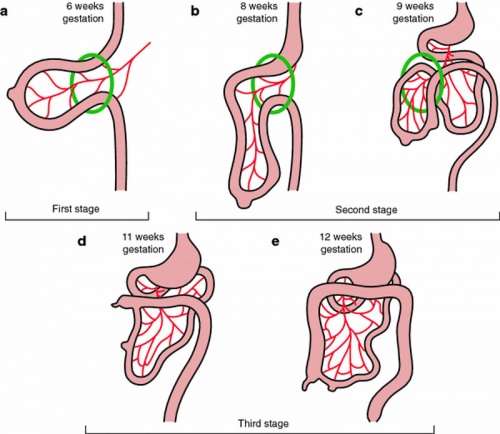
Normal intestinal rotation (note these are GA gestational age weeks).[1]
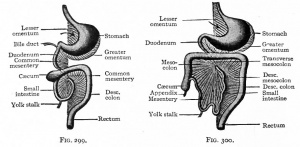
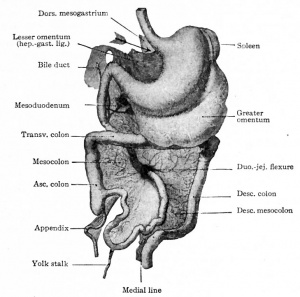
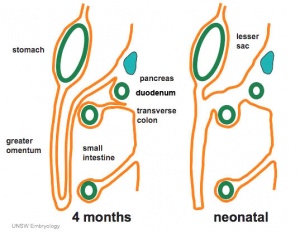
Stomach Mesentery
|
In the second trimester, the ventral and dorsal mesenteries associated with the stomach are still anatomically different from the newborn. The figure shows a lateral view of this process comparing the early second trimester arrangement with the newborn structure.
Ventral Mesogastrium
Attached to the superior end of the stomach will form the lesser omentum. This structure will connect the lesser curvature of the stomach to the liver as a ligamentous structure.
Dorsal Mesogastrium
Attached to the inferior end of the stomach initially as an extended fold, this later fuses as a single "apron-like" structure, the greater omentum. Fusion will also incorporate the transverse colon part of the large intestine.
This will also contribute the gastrosplenic ligament (gastrolienal ligament).
|
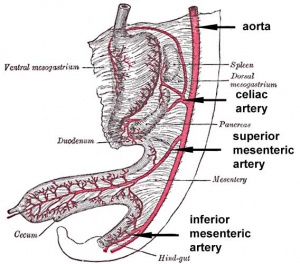
Blood Supply
|
|
Each region of the gastrointestinal tract has a specific arterial supply which historically defined the 3 gastrointestinal tract regions (foregut, midgut and hindgut).
- Foregut - celiac artery (Adult: pharynx, esophagus, stomach, upper duodenum, respiratory tract, liver, gallbladder pancreas)
- Midgut - superior mesenteric artery (Adult: lower duodenum, jejunum, ileum, cecum, appendix, ascending colon, half transverse colon)
- Hindgut - inferior mesenteric artery (Adult: half transverse colon, descending colon, rectum, superior part anal canal)
|
Fetal Tract Development
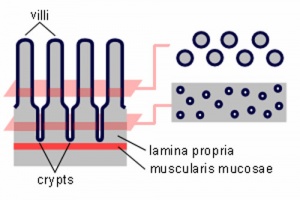
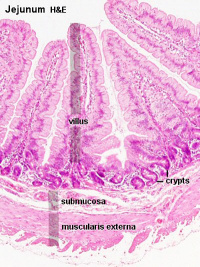
Small intestine villi and crypts
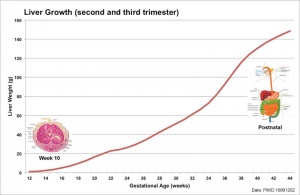
Liver weight 1 to 124 grams (birth)
Week 11 - villi begin to appear in small intestine, goblet cells present
Week 16 - villi apparent in entire intestine
Adult small intestine will be divided into 3 regions with the same basic histological organization.
- duodenum (25-30 cm)
- jejunum (about first two-fifths of the rest)
- ileum
Week 20 - Peyer's patches appear in small intestine
The adult intestinal immune system includes:
- Peyer's patches
- isolated lymphoid follicles
- cryptopatches - small clusters of lymphoid cells with an immature lymphocyte phenotype and dendritic cells.
- mesenteric lymph nodes
Intestinal Length Growth
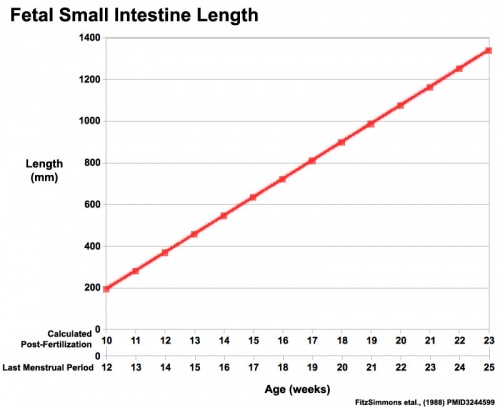
Small Intestine length (mm)
Amniotic Fluid
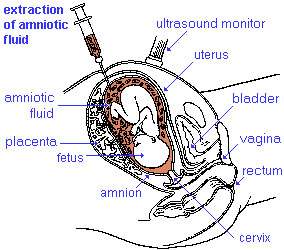
Amniocentesisis a prenatal diagnostic test, carried out by removing a small fluid sample.
- required for lung development.
- enables movement and symmetrical musculoskeletal development.
- maintains relatively constant temperature.
- protects by cushioning sudden blows or movements.
Volume - increases as the fetus grows.
- 34 weeks (GA) - peaks at about 800 mL.
- 40 weeks (GA) - about 600 mL at term.
- circulated by fetal inhaling and swallowing.
- replacing by fetal exhalation and urination.
- low magnesium levels associated with preeclampsia and diabetes.
Amniotic Fluid Swallowing
In early embryonic development both the buccopharyngeal and cloacal membranes degenerated, allowing the GIT to be filled with amniotic fluid. Towards the end of the fetal period the fetus is now swallowing approximately 500 ml of amniotic fluid / day.
<html5media width="480" height="360">https://www.youtube.com/embed/r9D7aiFG7N8</html5media>
This swallowed amniotic fluid moves through the GIT from esophagus, to stomach, to small intestine, stopping at the large bowel. In the large bowel the majority of fluid (water) is absorbed, along with electrolytes, glucose, urea and hormones. This process may contribute to fetal nutrition and prepare the GIT for its postnatal function. The process of swallowing amniotic fluid has been suggested to also help regulate fluid volume.
|
|
Polyhydramnios
|

|
Polyhydramnios (hydramnios, amniotic fluid disorder) refers to abnormally high amniotic fluid levels.
| Fetal Causes
|
| Decreased Fluid Swallowing or Absorption
|
Increased Fluid Production
|
|
|
- Lung disorders
- Multiple pregnancy
- Hydrops fetalis
|
| Maternal Causes - Poorly controlled diabetes.
|
|
Fetal Meconium
- Mixture of substances (debris, glandular secretions, fatty material and bile pigments) that accumulate in the large bowel (green fecal material).
- Will form the neonatal meconium which is the first (usually within 24h to 48h) postnatal excretion from the GIT.
- If no discharge (bowel motion) is observed in this early period it can be indicative of an abnormality of the GIT.
Meconium Aspiration
- Aspiration can occur near term or at delivery, if meconiumis discharged into the amiotic fluid (meconium stained amniotic fluid) and then injested by the fetus as it swallows amiotic fluid.
- Can then lead to meconium aspiration syndrome (MAS), meconium is drawn into the fetal/newborn lungs, causing inflammation, cell death and potentially perinatal death.
- Meconium can also damage the placenta and associated blood vessels.
| Gastrointestinal Tract Terms
|
- allantois - An extraembryonic membrane, endoderm in origin extension from the early hindgut, then cloaca into the connecting stalk of placental animals, connected to the superior end of developing bladder. In reptiles and birds, acts as a reservoir for wastes and mediates gas exchange. In mammals is associated/incorporated with connecting stalk/placental cord fetal-maternal interface.
- amnion - An extra-embryonic membrane, ectoderm and extraembryonic mesoderm in origin, also forms the innermost fetal membrane, that produces amniotic fluid. This fluid-filled sac initially lies above the trilaminar embryonic disc and with embryoic disc folding this sac is drawn ventrally to enclose (cover) the entire embryo, then fetus. The presence of this membrane led to the description of reptiles, bird, and mammals as amniotes.
- amniotic fluid - The fluid that fills amniotic cavity totally encloses and cushions the embryo. Amniotic fluid enters both the gastrointestinal and respiratory tract following rupture of the buccopharyngeal membrane. The late fetus swallows amniotic fluid.
- atresia - is an abnormal interruption of the tube lumen, the abnormality naming is based upon the anatomical location.
- buccal - (Latin, bucca = cheek) A term used to relate to the mouth (oral cavity).
- bile salts - Liver synthesized compounds derived from cholesterol that function postnatally in the small intestine to solubilize and absorb lipids, vitamins, and proteins. These compounds act as water-soluble amphipathic detergents. liver
- buccopharyngeal membrane - (oral membrane) (Latin, bucca = cheek) A membrane which forms the external upper membrane limit (cranial end) of the early gastrointestinal tract. This membrane develops during gastrulation by ectoderm and endoderm without a middle (intervening) layer of mesoderm. The membrane lies at the floor of the ventral depression (stomodeum) where the oral cavity will open and will breakdown to form the initial "oral opening" of the gastrointestinal tract. The equivilent membrane at the lower end of the gastrointestinal tract is the cloacal membrane.
- celiac artery - (celiac trunk) main blood supply to the foregut, excluding the pharynx, lower respiratory tract, and most of the oesophagus.
- cholangiocytes - epithelial cells that line the intra- and extrahepatic ducts of the biliary tree. These cells modify the hepatocyte-derived bile, and are regulated by hormones, peptides, nucleotides, neurotransmitters, and other molecules. liver
- cloaca - (cloacal cavity) The term describing the common cavity into which the intestinal, genital, and urinary tracts open in vertebrates. Located at the caudal end of the embryo it is located on the surface by the cloacal membrane. In many species this common cavity is later divided into a ventral urogenital region (urogenital sinus) and a dorsal gastrointestinal (rectal) region.
- cloacal membrane - Forms the external lower membrane limit (caudal end) of the early gastrointestinal tract (GIT). This membrane is formed during gastrulation by ectoderm and endoderm without a middle (intervening) layer of mesoderm. The membrane breaks down to form the initial "anal opening" of the gastrointestinal tract.
- coelomic cavity - (coelom) Term used to describe a space. There are extra-embryonic and intra-embryonic coeloms that form during vertebrate development. The single intra-embryonic coelom forms the 3 major body cavities: pleural cavity, pericardial cavity and peritoneal cavity.
- crypt of Lieberkühn - (intestinal gland, intestinal crypt) intestinal villi epithelia extend down into the lamina propria where they form crypts that are the source of epithelial stem cells and immune function.
- duplication - is an abnormal incomplete tube recanalization resulting in parallel lumens, this is really a specialized form of stenosis. (More? Image - small intestine duplication)
- esophageal - (oesophageal)
- foregut - first embryonic division of gastrointestinal tract extending from the oral (buccopharyngeal) membrane and contributing oesophagus, stomach, duodenum (to bile duct opening), liver, biliary apparatus (hepatic ducts, gallbladder, and bile duct), and pancreas. The forgut blood supply is the celiac artery (trunk) excluding the pharynx, lower respiratory tract, and most of the oesophagus.
- galactosemia - Metabolic abnormality where the simple sugar galactose (half of lactose, the sugar in milk) cannot be metabolised. People with galactosemia cannot tolerate any form of milk (human or animal). Detected by the Guthrie test.
- gastric transposition - clinical term for postnatal surgery treatment for esophageal atresia involving esophageal replacement. Typically performed on neonates between day 1 to 4. (More? gastrointestinal abnormalities | PMID 28658159
- gastrointestinal divisions - refers to the 3 embryonic divisions contributing the gastrointestinal tract: foregut, Midgut and hindgut.
- gastrula - (Greek, gastrula = little stomach) A stage of an animal embryo in which the three germ layers (endoderm/mesoderm/ectoderm) have just formed. All of these germ layers have contributions to the gastrointestinal tract.
- gastrulation - The process of differentiation forming a gastrula. Term means literally means "to form a gut" but is more in development, as this process converts the bilaminar embryo (epiblast/hypoblast) into the trilaminar embryo (endoderm/mesoderm/ectoderm) establishing the 3 germ layers that will form all the future tissues of the entire embryo. This process also establishes the the initial body axes. (More? gastrulation)
- Guthrie test - (heel prick) A neonatal blood screening test developed by Dr Robert Guthrie (1916-95) for determining a range of metabolic disorders and infections in the neonate. (More? Guthrie test)
- heterotaxia - (Greek heteros = different; taxis = arrangement) is the right/left transposition of thoracic and/or abdominal organs.
- hindgut - final embryonic division of gastrointestinal tract extending to the cloacal membrane and contributing part of the transverse colon (left half to one third), descending colon, sigmoid colon, rectum, part of anal canal (superior), urinary epithelium (bladder and most urethra). The hindgut blood supply is the inferior mesenteric artery.
- inferior mesenteric artery - main blood supply to the hindgut
- intestine - (bowel) part of the gastrointestinal tract (GIT) lying between the stomach and anus where absorption of nutrients and water occur. This region is further divided anatomically and functionally into the small intestine or bowel (duodenum, jejunum and ileum) and large intestine or bowel (cecum and colon).
- intestinal perforation - gastrointestinal abnormality identified in neonates can be due to necrotizing enterocolitis, Hirschsprung’s disease or meconium ileus.
- intraembryonic coelom - The "horseshoe-shaped" space (cavity) that forms initially in the third week of development in the lateral plate mesoderm that will eventually form the 3 main body cavities: pericardial, pleural, peritoneal. The intraembryonic coelom communicates transiently with the extraembryonic coelom.
- meconium ileus intestine obstruction within the ileum due to abnormal meconium properties.
- mesentery - connects gastrointestinal tract to the posterior body wall and is a double layer of visceral peritoneum.
- mesothelium - The mesoderm derived epithelial covering of coelomic organs and also line their cavities.
- Midgut - middle embryonic division of gastrointestinal tract contributing the small intestine (including duodenum distal bile duct opening), cecum, appendix, ascending colon, and part of the transverse colon (right half to two thirds). The midgut blood supply is the superior mesenteric artery.
- neuralation - The general term used to describe the early formation of the nervous system. It is often used to describe the early events of differentiation of the central ectoderm region to form the neural plate, then neural groove, then neural tube. The nervous system includes the central nervous system (brain and spinal cord) from the neural tube and the peripheral nervous system (peripheral sensory and sympathetic ganglia) from neural crest. In humans, early neuralation begins in week 3 and continues through week 4.
- neural crest - region of cells at the edge of the neural plate that migrates throughout the embryo and contributes to many different tissues. In the gastrointestinal tract it contributes mainly the enteric nervous system within the wall of the gut responsible for peristalsis and secretion.
- peritoneal stomata - the main openings forming the pathways for drainage of intra-peritoneal fluid from the peritoneal cavity into the lymphatic system.
- pharynx - uppermost end of gastrointestinal and respiratory tract, in the embryo beginning at the buccopharyngeal membrane and forms a major arched cavity within the phrayngeal arches.
- recanalization - describes the process of a hollow structure becoming solid, then becoming hollow again. For example, this process occurs during GIT, auditory and renal system development.
- retroperitoneal - (retroperitoneum) is the anatomical space (sometimes a potential space) in the abdominal cavity behind (retro) the peritoneum. Developmentally parts of the GIT become secondarily retroperitoneal (part of duodenum, ascending and descending colon, pancreas)
- somitogenesis The process of segmentation of the paraxial mesoderm within the trilaminar embryo body to form pairs of somites, or balls of mesoderm. A somite is added either side of the notochord (axial mesoderm) to form a somite pair. The segmentation does not occur in the head region, and begins cranially (head end) and extends caudally (tailward) adding a somite pair at regular time intervals. The process is sequential and therefore used to stage the age of many different species embryos based upon the number visible somite pairs. In humans, the first somite pair appears at day 20 and adds caudally at 1 somite pair/4 hours (mouse 1 pair/90 min) until on average 44 pairs eventually form.
- splanchnic mesoderm - Gastrointestinal tract (endoderm) associated mesoderm formed by the separation of the lateral plate mesoderm into two separate components by a cavity, the intraembryonic coelom. Splanchnic mesoderm is the embryonic origin of the gastrointestinal tract connective tissue, smooth muscle, blood vessels and contribute to organ development (pancreas, spleen, liver). The intraembryonic coelom will form the three major body cavities including the space surrounding the gut, the peritoneal cavity. The other half of the lateral plate mesoderm (somatic mesoderm) is associated with the ectoderm of the body wall.
- stomodeum - (stomadeum, stomatodeum) A ventral surface depression on the early embryo head surrounding the buccopharyngeal membrane, which lies at the floor of this depression. This surface depression lies between the maxillary and mandibular components of the first pharyngeal arch.
- stenosis - abnormal a narrowing of the tube lumen, the abnormality naming is based upon the anatomical location.
- superior mesenteric artery - main blood supply to the Midgut.
- viscera - the internal organs in the main cavities of the body, especially those in the abdomen, for example the Template:Intestines.
- visceral peritoneum - covers the external surfaces of the intestinal tract and organs within the peritoneum. The other component (parietal peritoneum) lines the abdominal and pelvic cavity walls.
- yolk sac - An extraembryonic membrane which is endoderm origin and covered with extraembryonic mesoderm. Yolk sac lies outside the embryo connected initially by a yolk stalk to the midgut with which it is continuous with. The endodermal lining is continuous with the endoderm of the gastrointestinal tract. The extra-embryonic mesoderm differentiates to form both blood and blood vessels of the vitelline system. In reptiles and birds, the yolk sac has a function associated with nutrition. In mammals the yolk sac acts as a source of primordial germ cells and blood cells. Note that in early development (week 2) a structure called the "primitive yolk sac" forms from hypoblast, this is an entirely different structure.
- yolk stalk - (vitelline duct, omphalomesenteric duct, Latin, vitellus = yolk of an egg) The endodermal connection between the midgut and the yolk sac. See vitelline duct.
|
|
|
Additional Information
| Additional Information - Content shown under this heading is not part of the material covered in this class. It is provided for those students who would like to know about some concepts or current research in topics related to the current class page.
|
Stem Cells
Stem cells in the adult epithelium of the intestine (and stomach) divide continuously throughout life to replace the 4 cell types within the epithelium:
- Brush-border cells - these absorptive cells in intestine microvilli increase the active surface area.
- Goblet cells - secreting mucus to protect the epithelium and to aid movement.
- Paneth cells - innate immune system and secrete cryptdins that kill bacteria.
- Enteroendocrine cells - (15+ subtypes) secrete serotonin and other peptide hormones acting on neurons and other cells to regulate many different functions.
|
|
- ↑ Martin V & Shaw-Smith C. (2010). Review of genetic factors in intestinal malrotation. Pediatr. Surg. Int. , 26, 769-81. PMID: 20549505 DOI.
BGDB: Lecture - Gastrointestinal System | Practical - Gastrointestinal System | Lecture - Face and Ear | Practical - Face and Ear | Lecture - Endocrine | Lecture - Sexual Differentiation | Practical - Sexual Differentiation | Tutorial
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2026, Mayıs 5) Embryology BGDB Gastrointestinal - Fetal. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/BGDB_Gastrointestinal_-_Fetal
- What Links Here?
- © Dr Mark Hill 2026, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G


























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



