| ICD-11
|
LA8B.21 Coarctation of aorta
- A congenital cardiovascular malformation in which there is a discrete luminal narrowing of the junction between the aortic arch and the descending aorta. Coarctation of the aorta generally indicates a narrowing of the descending thoracic aorta just distal to the left subclavian artery. However, the term may also be accurately used to refer to a region of narrowing anywhere in the thoracic or abdominal aorta.
LA8B.22 Interrupted aortic arch
- A congenital cardiovascular malformation in which there is an absence of luminal continuity between the ascending and descending aorta. This includes luminal atresia with discontinuity between the aortic segments and also luminal atresia with fibrous continuity between the aortic segments. Interrupted aortic arch is defined as the loss of luminal continuity between the ascending and descending aorta. In most cases, blood flow to the descending thoracic aorta is through a patent arterial duct, and there is a large ventricular septal defect. Arch interruption is further defined by site of interruption. In type A, interruption is distal to the left subclavian artery; in type B, interruption is between the left carotid and left subclavian arteries; and in type C, interruption occurs between the innominate and left carotid arteries.
|
| ICD-11 Structural developmental anomalies of the circulatory system (draft)
|
| ICD-11 Beta Draft - NOT FINAL, updated on a daily basis, It is not approved by WHO, NOT TO BE USED for CODING except for agreed FIELD TRIALS.
20 Developmental Anomalies - Structural Developmental Anomalies
Beta coding and tree structure for "structural developmental anomalies" within this section are shown in the table below.
|
| Structural developmental anomalies of the circulatory system
|
- Structural developmental anomaly of heart and great vessels
- LB00 Congenital heart or great vessel related acquired abnormality
- LB01 Congenital anomaly of atrioventricular or ventriculo-arterial connections
- LB01.1 Transposition of the great arteries
- LB01.2 Double outlet right ventricle
- LB01.3 Double outlet left ventricle
- LB01.4 Common arterial trunk
- LB01.Y Other specified congenital anomaly of atrioventricular or ventriculo-arterial connections
- LB01.Z Congenital anomaly of atrioventricular or ventriculo-arterial connections, unspecified
- LB02 Congenital anomaly of the mediastinal veins Congenital anomaly of atria or atrial septum
- LB20 Congenital anomaly of atrioventricular valves or septum
- LB21 Congenital anomaly of ventricles and ventricular septum
- LB21.1 Congenital right ventricular outflow tract obstruction
- LB21.2 Double-chambered right ventricle
- LB21.3 Tetralogy of Fallot
- LB21.4 Congenital left ventricular outflow tract obstruction
- LB21.5 Congenital ventricular septal defects
- LB21.Y Other specified congenital anomaly of ventricles and ventricular septum
- LB21.Z Congenital anomaly of ventricles and ventricular septum, unspecified
- LB22 Functionally univentricular heart
- LB23 Congenital anomaly of ventriculo-arterial valves and adjacent regions
- LB24 Congenital anomaly of great arteries including arterial duct
- LB.1 Congenital aorto-pulmonary window
- LB.2 Congenital anomaly of pulmonary arterial tree
- LB.3 Congenital anomaly of aorta and its branches
- LB.4 Tracheo-oesophageal compressive syndrome
- LB.5 Patent arterial duct
- LB.Y Other specified congenital anomaly of great arteries including arterial duct
- LB.Z Congenital anomaly of great arteries including arterial duct, unspecified
- LB25 Anomalous position-orientation of heart
- LB26 Total mirror imagery
- LB27 Left isomerism
- LB28 Congenital anomaly of coronary arteries
- LB29 Structural developmental anomalies of the pericardium
- LB2Y Other specified structural developmental anomaly of heart and great vessels
- LB2Z Structural developmental anomaly of heart and great vessels, unspecified
- LB30 Structural developmental anomalies of the peripheral vascular system
- LB30.1 Capillary malformations
- LB30.2 Lymphatic malformations
- LB30.21 Macrocystic lymphatic malformation
- LB30.22 Microcystic lymphatic malformation
- LB30.23 Cystic hygroma in fetus
- BD23.1 Primary lymphoedema
- EK91 Yellow nail syndrome
- LC5F.26 Noonan syndrome
- LB30.2Y Other specified lymphatic malformations
- LB30.2Z Lymphatic malformations, unspecified
- LB30.3 Peripheral venous malformations
- LB30.4 Peripheral arteriovenous malformations
- LB30.5 Peripheral arterial malformations
- LB30.6 Pulmonary arteriovenous fistula
- LB30.Y Other specified structural developmental anomalies of the peripheral vascular system
- LB30.Z Structural developmental anomalies of the peripheral vascular system, unspecified
- LB3Y Other specified structural developmental anomalies of the circulatory system
- LB3Z Structural developmental anomalies of the circulatory system, unspecified
|
| CD-11 Beta Draft - NOT FINAL, updated on a daily basis, It is not approved by WHO, NOT TO BE USED for CODING except for agreed FIELD TRIALS.
See also International Classification of Diseases | Abnormalities
|
Introduction
- 5-8% of Congenital Heart Disease
- Aortic constriction.
- Treatment aims at maintaining the ductus arteriosus via prostaglandins and by surgical intervention.
A review suggests it may:[1]
- affect the aortic arch in a highly variable manner
- be associated with a host of other left sided heart lesions
- represent a wider vasculopathy within the pre-coarctation arterial tree
- Links: Search PubMed | PMID 21947983 | 2011 Review PDF
Some Recent Findings
- Confirmation of the role of pathogenic SMAD6 variants in bicuspid aortic valve-related aortopathy[2] Progressive dilatation of the thoracic aorta leads to thoracic aortic aneurysm (TAA), which is often asymptomatic but predisposes to lethal aortic dissections and ruptures. TAA is a common complication in patients with bicuspid aortic valve (BAV). Recently, rare loss-of-function SMAD6 variants were shown to contribute significantly to the genetic aetiology of BAV/TAA. ...Here, we report on the results of a SMAD6-variant analysis in 473 unrelated non-syndromic TAA patients, of which the SMAD6-positive individuals were also studied for the presence of the BMP2 risk allele. Although only 14% of the TAA patients also presented BAV, all novel likely pathogenic SMAD6 variants (N = 7) were identified in BAV/TAA individuals, further establishing the role of SMAD6 variants to the aetiology of BAV/TAA and revealing limited contribution to TAA development in patients with a tricuspid aortic valve."
- Multicenter experience with endovascular treatment of aortic coarctation in adults[3] "The objective of this study was to evaluate outcomes of endovascular treatment of aortic coarctation in adults. Clinical data and imaging studies of 93 consecutive patients treated at nine institutions from 1999 to 2015 were reviewed. We included newly diagnosed aortic coarctation (NCO), recurrent coarctation, and aneurysmal/pseudoaneurysmal degeneration (ANE) after prior open surgical repair (OSR) of coarctation. Primary end points were morbidity and mortality. Secondary end points were stent patency and freedom from reintervention. Endovascular repair is effective with an acceptable safety profile in the treatment of NCO and postsurgical complications of coarctation after initial OSR. Aortic rupture is an infrequent (2%) but devastating complication with high mortality. Balloon-expandable covered stents are preferred for NCO, whereas stent grafts are used for ANE. The rate of reinterventions is acceptable, with high procedural and long-term clinical success."
- Inherited Deletion of 1q, Hyperparathyroidism and Signs of Y-chromosomal Influence in a Patient with Turner syndrome[4] "We report a detailed phenotypic, cytogenetic and molecular characterization of a patient prenatally diagnosed with Turner syndrome (TS). In addition to having typical TS clinical characteristics including webbed neck, high arched palate and coarctation of the aorta, the patient had features less frequently seen in TS."
- A complex case of aortic arch interruption and hypoplastic descending aorta[5] "The case of a newborn with a post-ductal interrupted aortic arch combined with severe hypoplasia of the thoracic descending aorta and intracardiac defects is described. Extraanatomic bypass surgery was performed in the neonatal period to connect the ascending and descending parts of the aorta. Closure of a ventricular septal defect and excision of hypertrophied bands in the right ventricle with subsequent ventriculotomy were delayed beyond neonatal age."
|
| More recent papers
|
|
This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
- This search now requires a manual link as the original PubMed extension has been disabled.
- The displayed list of references do not reflect any editorial selection of material based on content or relevance.
- References also appear on this list based upon the date of the actual page viewing.
References listed on the rest of the content page and the associated discussion page (listed under the publication year sub-headings) do include some editorial selection based upon both relevance and availability.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References
Search term: Coarctation of the Aorta
|
| Older papers
|
| These papers originally appeared in the Some Recent Findings table, but as that list grew in length have now been shuffled down to this collapsible table.
See also the Discussion Page for other references listed by year and References on this current page.
- The effect of including increased arterial stiffness in the upper body when modelling Coarctation of the Aorta[6] "Coarctation of the Aorta is a congenital narrowing of the aorta and diagnosis can be difficult. Treatments result in idiopathic sequelae including hypertension. Untreated patients are known to develop increased arterial stiffness in the upper body, which worsens with time. We present results from simulations with a one-dimensional mathematical model, about the effect of stiffness, stenting, surgery and coarctation severity on blood pressure, Pulsatility and Resistivity Index. One conclusion is that increased stiffness may explain both hypertension in treated patients and why diagnosis can be difficult."
- A new anatomic approach of the ventricular septal defect in the interruption of the aortic arch[7] "The aim of this study was to analyse the anatomy of the ventricular septal defect (VSD) in heart specimens with interruption of the aortic arch (IAA) in order to explore the hypothesis of different embryologic mechanisms for the different anatomic types of IAA. We examined 42 human heart specimens, 25 with IAA as the main disease with concordant atrioventricular and ventriculo-arterial connections and two distinct great arteries, and 17 hearts with IAA associated with other malformations [six common arterial trunk (CAT), five double-outlet right ventricle (DORV), three transposition of the great arteries (TGA), three atrioventricular septal defect (AVSD)]. The interruption was classified according to Celoria and Patton. ...These results reinforce the hypothesis that different pathogenic mechanisms are responsible for the two types of IAA, and the inclusion of IAA type B in the group of neural crest defects. Conversely, IAA type A could be due to overlapping mechanisms: flow-related defect (coarctation-like) and neural crest contribution."
|
Sex Ratios
Clinical Imaging
Ultrasound
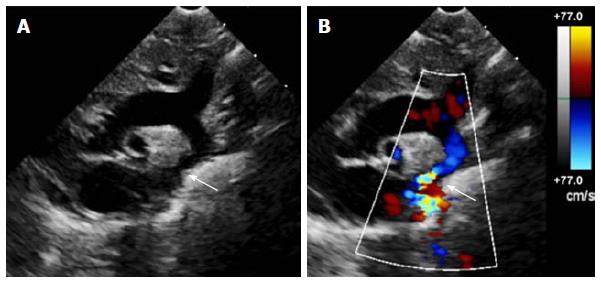
Echocardiography uses standard two-dimensional, three-dimensional, and Doppler ultrasound to create images of the heart.
| Echocardiogram Coarctation of the Aorta[9]
|
|
| A Two-dimensional transthoracic echocardiogram image obtained from the suprasternal notch in an 11-day-old infant demonstrating discrete coarctation (arrow).
|
B Colour Doppler of the same image with aliasing of flow at the site of coarctation (arrow).
|
Magnetic Resonance Imaging
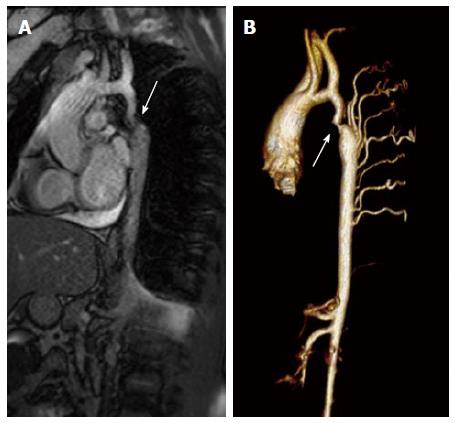
| Coarctation of the Aorta MRI[9]
|
|
| A Magnetic resonance image (steady-state free precession) in a sagittal projection demonstrating transverse arch hypoplasia and long segment coarctation of the aorta distal to the left subclavian artery (arrow) in a 12-year-old male.
|
B Three-dimensional reconstruction of a gated contrasted angiogram for the same patient, which demonstrates transverse arch hypoplasia, coarctation at the aorta at the distal transverse aortic arch and isthmus (arrow), and dilated intercostal arteries (collaterals).
|
References
- ↑ Kenny D & Hijazi ZM. (2011). Coarctation of the aorta: from fetal life to adulthood. Cardiol J , 18, 487-95. PMID: 21947983
- ↑ Luyckx I, MacCarrick G, Kempers M, Meester J, Geryl C, Rombouts O, Peeters N, Claes C, Boeckx N, Sakalihasan N, Jacquinet A, Hoischen A, Vandeweyer G, Van Lent S, Saenen J, Van Craenenbroeck E, Timmermans J, Duijnhouwer A, Dietz H, Van Laer L, Loeys B & Verstraeten A. (2019). Confirmation of the role of pathogenic SMAD6 variants in bicuspid aortic valve-related aortopathy. Eur. J. Hum. Genet. , , . PMID: 30796334 DOI.
- ↑ Erben Y, Oderich GS, Verhagen HJM, Witsenburg M, van den Hoven AT, Debus ES, Kölbel T, Arko FR, Torsello GB, Torsello GF, Lawrence PF, Harlander-Locke MP, Bacharach JM, Jordan WD, Eskandari MK & Hagler DJ. (2019). Multicenter experience with endovascular treatment of aortic coarctation in adults. J. Vasc. Surg. , 69, 671-679.e1. PMID: 30528403 DOI.
- ↑ Siller AF, Shimony A, Shinawi M, Amarillo I, Dehner LP, Semenkovich K & Arbeláez AM. (2019). Inherited Deletion of 1q, Hyperparathyroidism and Signs of Y-chromosomal Influence in a Patient with Turner Syndrome. J Clin Res Pediatr Endocrinol , 11, 88-93. PMID: 29739732 DOI.
- ↑ Pérez-Andreu J, Fernández-Doblas J, Giralt García G, Roses F & Abella RF. (2019). A complex case of aortic arch interruption and hypoplastic descending aorta. Asian Cardiovasc Thorac Ann , , 218492318804948. PMID: 30754985 DOI.
- ↑ Pathirana D, Johnston B & Johnston P. (2019). The effect of including increased arterial stiffness in the upper body when modelling Coarctation of the Aorta. Comput Methods Biomech Biomed Engin , , 1-15. PMID: 30714407 DOI.
- ↑ Mostefa Kara M, Houyel L & Bonnet D. (2019). A new anatomic approach of the ventricular septal defect in the interruption of the aortic arch. J. Anat. , 234, 193-200. PMID: 30525196 DOI.
- ↑ Michalski AM, Richardson SD, Browne ML, Carmichael SL, Canfield MA, VanZutphen AR, Anderka MT, Marshall EG & Druschel CM. (2015). Sex ratios among infants with birth defects, National Birth Defects Prevention Study, 1997-2009. Am. J. Med. Genet. A , 167A, 1071-81. PMID: 25711982 DOI.
- ↑ 9.0 9.1 Torok RD, Campbell MJ, Fleming GA & Hill KD. (2015). Coarctation of the aorta: Management from infancy to adulthood. World J Cardiol , 7, 765-75. PMID: 26635924 DOI.
Reviews
Law MA & Tivakaran VS. (2018). Coarctation of the Aorta. , , . PMID: 28613663
Batlivala SP & Goldstein BH. (2019). Current Transcatheter Approaches for the Treatment of Aortic Coarctation in Children and Adults. Interv Cardiol Clin , 8, 47-58. PMID: 30449421 DOI.
Doshi AR & Chikkabyrappa S. (2018). Coarctation of Aorta in Children. Cureus , 10, e3690. PMID: 30761242 DOI.
Hoffman JI. (2018). The challenge in diagnosing coarctation of the aorta. Cardiovasc J Afr , 29, 252-255. PMID: 29293259 DOI.
Ghi T, Dall'Asta A, Cavalli C, Galli L, Weiss A, Pedrazzi G, Kaihura CT, Volpe N, Agnetti A & Frusca T. (2018). How often an isolated cardiac disproportion predicts a coarctation of the aorta? Single center experience and systematic review of the literature. J. Matern. Fetal. Neonatal. Med. , 31, 1350-1357. PMID: 28366040 DOI.
Suradi H & Hijazi ZM. (2015). Current management of coarctation of the aorta. Glob Cardiol Sci Pract , 2015, 44. PMID: 26779519 DOI.
Hartman EM, Groenendijk IM, Heuvelman HM, Roos-Hesselink JW, Takkenberg JJ & Witsenburg M. (2015). The effectiveness of stenting of coarctation of the aorta: a systematic review. EuroIntervention , 11, 660-8. PMID: 26499220 DOI.
Buyens A, Gyselaers W, Coumans A, Al Nasiry S, Willekes C, Boshoff D, Frijns JP & Witters I. (2012). Difficult prenatal diagnosis: fetal coarctation. Facts Views Vis Obgyn , 4, 230-6. PMID: 24753914
Articles
Iriart X, Laïk J, Cremer A, Martin C, Pillois X, Jalal Z, Roubertie F & Thambo JB. (2019). Predictive factors for residual hypertension following aortic coarctation stenting. J Clin Hypertens (Greenwich) , 21, 291-298. PMID: 30585428 DOI.
Search Pubmed
Search Pubmed: Coarctation of the Aorta
Search OMIM: Coarctation of the Aorta
External Links
External Links Notice - The dynamic nature of the internet may mean that some of these listed links may no longer function. If the link no longer works search the web with the link text or name. Links to any external commercial sites are provided for information purposes only and should never be considered an endorsement. UNSW Embryology is provided as an educational resource with no clinical information or commercial affiliation.
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2026, July 10) Embryology Cardiovascular System - Coarctation of the Aorta. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Cardiovascular_System_-_Coarctation_of_the_Aorta
- What Links Here?
- © Dr Mark Hill 2026, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G