Talk:Abnormal Development - Cytomegalovirus: Difference between revisions
(→2010) |
(→2001) |
||
| Line 145: | Line 145: | ||
PMID 11229670 | PMID 11229670 | ||
==1993== | |||
===Cell types infected in human cytomegalovirus placentitis identified by immunohistochemical double staining=== | |||
Virchows Arch A Pathol Anat Histopathol. 1993;423(4):249-56. | |||
Sinzger C, Müntefering H, Löning T, Stöss H, Plachter B, Jahn G. | |||
Source | |||
Institut für Klinische und Molekulare Virologie, Universität Erlangen-Nürnberg, Germany. | |||
Abstract | |||
Chronic villitis is almost always present in intrauterine infection with human cytomegalovirus (HCMV). The inflammatory response to this virus has been described in detail. However, little is known about the types of placental cells that may be infected by HCMV and six cases of HCMV placentitis were thus investigated to identify the vulnerable cell types. Immunohistochemical double staining analyses were performed using antibodies to HCMV immediate early antigens and to specific cellular marker proteins. Fixed connective tissue cells could be demonstrated to be the predominantly infected cell type in each placental tissue. Endothelial cells and macrophages were also found to be infected in all six cases, whereas evidence of trophoblast infection was obtained in four cases. It is concluded that release of infectious virus by connective tissue cells, macrophages and endothelial cells may play a critical role in transplacental transmission of HCMV. The findings further suggest that the cytopathic effect of HCMV infection on these cells might be involved in the pathogenesis of intrauterine HCMV disease. | |||
PMID 8236822 | |||
==CDC Images== | ==CDC Images== | ||
Revision as of 14:29, 12 April 2012
| About Discussion Pages |
|---|

Glossary Links
Cite this page: Hill, M.A. (2024, May 18) Embryology Abnormal Development - Cytomegalovirus. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Talk:Abnormal_Development_-_Cytomegalovirus |
2012
Chronic Histiocytic Intervillositis with Cytomegalovirus Placentitis in a Case of Hydrops Fetalis
Fetal Pediatr Pathol. 2012 Mar 23.
Taweevisit M, Sukpan K, Siriaunkgul S, Thorner PS. Source Department of Pathology, Chulalongkorn University, Pathumwan , Bangkok , Thailand. Abstract Chronic histiocytic intervillositis (CHI) is an infrequent inflammatory placental disorder associated with unfavorable pregnancy outcomes and a high rate of recurrence. This disorder is thought to reflect a maternal delayed hypersensitivity response to fetal antigen(s) in placental tissue. We report a case of a 20-week-gestation hydropic fetus in which the placenta showed chronic histiocytic intervillositis with cytomegalovirus placentitis. Immunophenotyping studies supported a delayed hypersensitivity response. This is the first report of these two diseases co-occurring, raising the possibility of a relationship between chronic histiocytic intervillositis and infection. Chronic histiocytic intervillositis may represent an idiosyncratic immune response, in this case to cytomegalovirus.
PMID 22443234
2011
Update on the prevention, diagnosis and management of cytomegalovirus infection during pregnancy
Clin Microbiol Infect. 2011 Apr 25. doi: 10.1111/j.1469-0691.2011.03564.x. [Epub ahead of print]
Lazzarotto T, Guerra B, Gabrielli L, Lanari M, Landini MP. Source Department of Haematology, Oncology and Laboratory Medicine, Operative Unit of Clinical Microbiology Department of Obstetrics and Gynaecology, St Orsola Malpighi General Hospital, University of Bologna, Bologna Operative Unit of Paediatrics and Neonatology, La Scaletta Hospital, Imola-Bologna, Italy.
Abstract
Clin Microbiol Infect ABSTRACT: Human cytomegalovirus (CMV) is the leading cause of congenital infection, with morbidity and mortality at birth and sequelae. Each year approximately 1-7% (Rev Med Virol 2010; 20: 311) of pregnant women acquire a primary CMV infection. Of these, about 30-40% transmit infection to their fetuses. The risk of serious fetal injury is greatest when maternal infection develops in the first trimester or early in the second trimester. Between 10 and 15% of congenitally infected infants are acutely symptomatic at birth and most of the survivors have serious long-term complications. Until a few years ago, laboratory testing was not possible to precisely define the maternal immune status, the recent development of advanced serological tests (IgG avidity test, IgM immunoblot and neutralizing antibody testing) allow us to identify, among pregnant women with suspected CMV, those with primary infection who are therefore at high risk of transmitting CMV to the fetus. This is done with the use of a screening test. As most maternal infections are asymptomatic, the only way to disclose primary infection is to implement specific serological testing as early in pregnancy as possible (before week 12-16 of gestation). Given the high risk of mother-fetus transmission and fetal damage, prenatal diagnosis is recommended to women with primary CMV infection contracted in the first half of pregnancy and in case of fetal abnormalities suggestive of infection. The correct interpretation of serological and virological tests followed by appropriate counselling by an expert physician is an effective tool to reduce the number of unnecessary pregnancy terminations by over 70% (Am J Obstet Gynecol 2007; 196: 221.e1).
© 2011 The Authors. Clinical Microbiology and Infection © 2011 European Society of Clinical Microbiology and Infectious Diseases.
PMID 21631642
2010
Neurodevelopmental outcome following congenital cytomegalovirus infection in preterm infants with twin-to-twin transfusion syndrome: a case report
Klin Padiatr. 2010 Sep;222(5):312-4. Epub 2010 Aug 30.
Griesmaier E, Neubauer V, Blum S, Trawöger R, Keller M, Kiechl-Kohlendorfer U. Source Innsbruck Medical University, Department of Pediatrics IV, Innsbruck, Austria. Elke.Griesmaier@i-med.ac.at
Abstract
Twin-to-twin transfusion syndrome and conital cytomegalovirus infection bear the risk of brain damage. In the 27th week of gestation of a twin pregnancy a Caesarean section was performed because of pathological cardiotocogram and Doppler ultrasonography of the second twin (recipient). Both infants presented with severe, persistent thrombocytopenia, elevated liver enzymes and direct hyperbilirubinemia. Primary congenital CMV infection was diagnosed. Both twins showed severe neuropathological symptoms, pathological aEEG with seizure activity and severe neurodevelopmental delay at corrected age of 12 months. The severity of brain pathology, the complex etiology, its consequence for neurotion with extreme prematurity make this case of special interest. Georg Thieme Verlag KG Stuttgart, New York.
PMID 20806166
Transmission of cytomegalovirus via breast milk to the prematurely born infant: a systematic review
Clin Microbiol Infect. 2010 Aug;16(8):1172-8.
Kurath S, Halwachs-Baumann G, Müller W, Resch B. Source Paediatric Department, Division of Neonatology, Research Unit for Neonatal Infectious Diseases and Epidemiology, Medical University of Graz, Graz, Austria.
Abstract
To analyse current data on transmission of human cytomegalovirus (HCMV) via breast milk with subsequent symptomatic HCMV infection of the preterm infant and to report on long-term follow-up, a systematic literature review was performed using EMBASE, MEDLINE and CINAHL (January 1966 to December 2008) Studies were included for analysis if congenital HCMV infection was excluded and transmission via breast milk was either confirmed or strongly suspected. Twenty-six studies were included for analysis. Maternal HCMV-IgG-positivity was reported to be in the range 51.6-100% (median 81.6%), HCMV-IgG detection in breast milk in the range 67-97.2% (median 80%) and HCMV-positivity of the infants in the range 5.7-58.6%. Symptomatic HCMV disease occurred in 0-34.5% (median 3.7%) and severe sepsis-like syndrome in 0-13.8% (median 0.7%). Data on long-term outcome of preterm infants with symptomatic HCMV infection revealed a low risk for mild neurological and cognitive sequelae, without hearing impairment. Recommendations for high-risk preterm infants diverged markedly. The current data report low rates of symptomatic disease after transmission of HCMV via breast milk to the preterm infant without evidence of certain long-term sequelae. The results of our review do not support a general approach, either by avoidance or pasteurization of breast milk, in high-risk preterm infants.
PMID 20670291
2009
Histological findings in foetuses congenitally infected by cytomegalovirus
J Clin Virol. 2009 Dec;46 Suppl 4:S16-21. Epub 2009 Oct 30.
Gabrielli L, Bonasoni MP, Lazzarotto T, Lega S, Santini D, Foschini MP, Guerra B, Baccolini F, Piccirilli G, Chiereghin A, Petrisli E, Gardini G, Lanari M, Landini MP. Source St. Orsola Malpighi GH, University of Bologna, Italy. liliana.gabrielli@aosp.bo.it Abstract BACKGROUND: Congenital cytomegalovirus (CMV) infection is a major cause of central nervous system damage leading to sensorineural hearing loss, mental retardation and cerebral palsy. OBJECTIVES: Identify the type of organ involvement and understand the histopathogenesis of damage in foetuses of women with a CMV-highly positive amniotic fluid. STUDY DESIGN: 34 foetuses with congenital CMV infection documented by prenatal diagnosis were studied. Three foetuses died in utero. The remaining pregnancies were electively terminated at 20-21 weeks gestation. RESULTS: Foetal organs positive for CMV antigens were: placenta (100%), pancreas (100%), lung (87%), kidney (87%), liver (71%), brain (55%) and heart (44%). Inflammatory infiltrate was almost always present in CMV-infected foetal organs and the severity of the inflammatory response was correlated with the organ damage. Brain damage with necrosis was observed in 33% (9/27) and a mild telencephalic leukoencephalopathy in 22% (6/27) of foetuses studied. CONCLUSIONS: Focal necrosis was observed very frequently in organs such as pancreases, livers, hearts and kidneys. However the damage in these organs is likely to be resolved by parenchymal regeneration. Brain damage, which seems to be the results of a combined effect of viral infection, inflammatory infiltration and hypoxia due to severe placentitis, is less likely to be resolved because of the low regeneration ability of this organ.
PMID 19879801
2007
Translational mini-review series on infectious disease: congenital cytomegalovirus infection: 50 years on
Clin Exp Immunol. 2007 Aug;149(2):205-10. Hassan J, Connell J. Source National Virus Reference Laboratory and Centre for Research into Infectious Disease, University College Dublin, Dublin, Ireland. jaythoon.hassan@ucd.ie
Abstract
Cytomegalovirus (CMV) is the leading cause of congenital viral infection, with an incidence of 0.5-3% of live births worldwide. Clinical evidence has shown hearing and vision loss, mental retardation and sometimes death in affected newborns. Primary maternal CMV infection during gestation poses a 40% risk of intrauterine transmission in contrast to recurrent infection. European laboratories have made significant progress in the last decade in solving diagnostic problems linked to infection in pregnancy. With the advances in CMV serology, such as detection of anti-CMV IgM by enzyme immunoassays (EIA), confirmed by Western blot, together with seroconversion and anti-CMV IgG avidity evaluation in pregnant mothers, can help to identify recent infection. Preventative measures such as screening for CMV in the routine serological work-up of pregnant women have been introduced in countries such as Spain and Italy. The development of specific T cell-mediated immune responses in mothers, fetus and neonates is now emerging with regard to antigen-specific CD4 and CD8 T cells, differentiation status, proliferative and cytokine responses. A protective vaccine against CMV is a major public health priority and the study of vaccines in animal model systems has identified potential strategies for interrupting transmission and preventing disease in newborns. Congenital CMV infection has a variable outcome and therefore novel diagnostic methods are required to identify those at risk and therapeutic interventions are needed to improve the long-term prognosis of those infected. CMV was first isolated in 1957. We are now 50 years on, so procrastination is not an option.
PMID 17635529
Cytomegalovirus-induced mirror syndrome associated with elevated levels of circulating antiangiogenic factors
Obstet Gynecol. 2007 Feb;109(2 Pt2):549-52.
Rana S, Venkatesha S, DePaepe M, Chien EK, Paglia M, Karumanchi SA. Source Maternal Fetal Medicine Division, Department of Obstetrics and Gynecology, Women and Infants Hospital, Brown University, Providence, Rhode Island 02905, USA. saroshrana@gmail.com Erratum in Obstet Gynecol. 2007 May;109(5):1207. Abstract BACKGROUND: We describe a case where Mirror syndrome was characterized by altered levels of antiangiogenic proteins (soluble fms-like tyrosine kinase 1 [sFlt1] and soluble endoglin). CASE: We describe a pregnant patient with severe fetal and placental edema induced by congenital cytomegalovirus (CMV) infection that was associated with preeclampsia. Fetal CMV was confirmed histologically, whereas antiangiogenic factors were demonstrated to be elevated in maternal but not fetal blood. The levels of sFlt1 and soluble endoglin in our patient's serum before delivery were 116.5 ng/mL (normal pregnancy 19.3 ng/mL and preeclampsia 66.0 ng/mL, representing mean values before delivery) and 107.4 ng/mL (normal pregnancy 18.7 ng/mL and preeclampsia 52.6 ng/mL, representing mean values before delivery), respectively. In contrast, the values of sFlt1 and soluble endoglin in the cord blood were relatively low at 2.1 ng/mL and 8.2 ng/mL, respectively. CONCLUSION: If this observation is confirmed, CMV infection may be cited as a cause of Mirror syndrome and preeclampsia phenotypes associated with this disorder may be related to increased circulating antiangiogenic factors. Comment in Obstet Gynecol. 2007 May;109(5):1205-6; author reply 1206.
PMID 17267891
2001
Epidemiology of transmission of cytomegalovirus from mother to preterm infant by breastfeeding
Lancet. 2001 Feb 17;357(9255):513-8.
Hamprecht K, Maschmann J, Vochem M, Dietz K, Speer CP, Jahn G. Source Institute of Medical Virology and Epidemiology of Viral Diseases, University Hospital of Tübingen, Germany. kshampre@med.uni-tuebingen.de
Abstract
BACKGROUND: Breastfeeding practices strongly influence the epidemiology of human cytomegalovirus infection. By contrast with term neonates, few data are available on transmission of infection from mothers to preterm infants during breastfeeding.
METHODS: 151 mothers and their 176 preterm infants (gestational age at birth <32 weeks or birthweight <1500 g) were prospectively screened for cytomegalovirus infection by serology, virus culture, and PCR. The roles of cell-free and cell-associated cytomegalovirus excretion during lactation were analysed longitudinally in relation to transmission, by maximum-likelihood estimates.
FINDINGS: Of the 69 seronegative breastfeeding control mothers, none had detectable cytomegalovirus DNA in breastmilk and none of their 80 infants shed the virus in urine. The proportion of cytomegalovirus reactivation in seropositive breastfeeding mothers was 96% (73 of 76). The early appearance of viral DNA in milk whey (median 3.5 days post partum in transmitters; 8 days in non-transmitters; p=0.025) and infectious virus in milk whey (10 days and 16 days, respectively; p=0.005) were risk factors for transmission. The cumulative rate of transmission was 37% (27 of 73 mothers; 33 infants). The infection of the neonates had a mean incubation time of 42 days (95% CI 28-69). About 50% of the infected infants had no symptoms, but four had sepsis-like symptoms.
INTERPRETATION: The proportion of cytomegalovirus reactivation during lactation almost equals maternal seroprevalence. Breastfeeding as a source of postnatal cytomegalovirus infection in preterm infants has been underestimated and may be associated with a symptomatic infection.
Comment in Lancet. 2001 Jun 2;357(9270):1800. Lancet. 2001 Jun 2;357(9270):1799-800. PMID 11229670
1993
Cell types infected in human cytomegalovirus placentitis identified by immunohistochemical double staining
Virchows Arch A Pathol Anat Histopathol. 1993;423(4):249-56.
Sinzger C, Müntefering H, Löning T, Stöss H, Plachter B, Jahn G. Source Institut für Klinische und Molekulare Virologie, Universität Erlangen-Nürnberg, Germany.
Abstract
Chronic villitis is almost always present in intrauterine infection with human cytomegalovirus (HCMV). The inflammatory response to this virus has been described in detail. However, little is known about the types of placental cells that may be infected by HCMV and six cases of HCMV placentitis were thus investigated to identify the vulnerable cell types. Immunohistochemical double staining analyses were performed using antibodies to HCMV immediate early antigens and to specific cellular marker proteins. Fixed connective tissue cells could be demonstrated to be the predominantly infected cell type in each placental tissue. Endothelial cells and macrophages were also found to be infected in all six cases, whereas evidence of trophoblast infection was obtained in four cases. It is concluded that release of infectious virus by connective tissue cells, macrophages and endothelial cells may play a critical role in transplacental transmission of HCMV. The findings further suggest that the cytopathic effect of HCMV infection on these cells might be involved in the pathogenesis of intrauterine HCMV disease.
PMID 8236822
CDC Images
http://phil.cdc.gov/phil_images/20030425/14/PHIL_3646_lores.jpg
{kind=link}
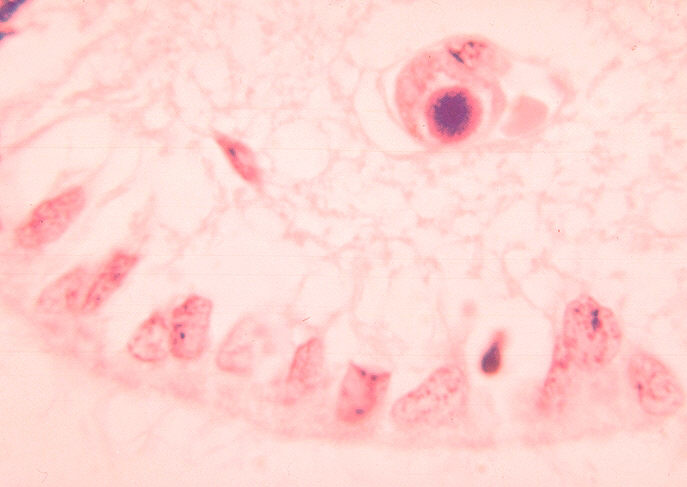
Histopathology of cytomegalovirus infection of brain
http://phil.cdc.gov/PHIL_Images/06011999/00021/09G0041_lores.jpg
{kind=link}
ID#:1160 Description: Histopathology of cytomegalovirus infection of brain.
Histopathology of cytomegalovirus infection of brain capillary endothelial cell.
High Resolution: High resolution download is not available for this image
Content Providers(s):CDC/ Dr. HarasztiCreation Date:1964
Copyright Restrictions:None - This image is in the public domain and thus free of any copyright restrictions. As a matter of courtesy we request that the content provider be credited and notified in any public or private usage of this image.
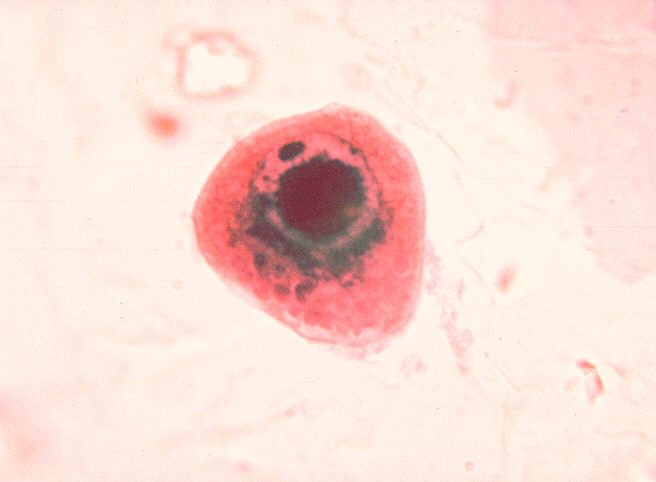
Cytomegalovirus infection of cell in urine
http://phil.cdc.gov/PHIL_Images/06011999/00018/09G0038_lores.jpg
{kind=link}
High Resolution: High resolution download is not available for this image
Content Providers(s):CDC/ Dr. HarasztiCreation Date:1964
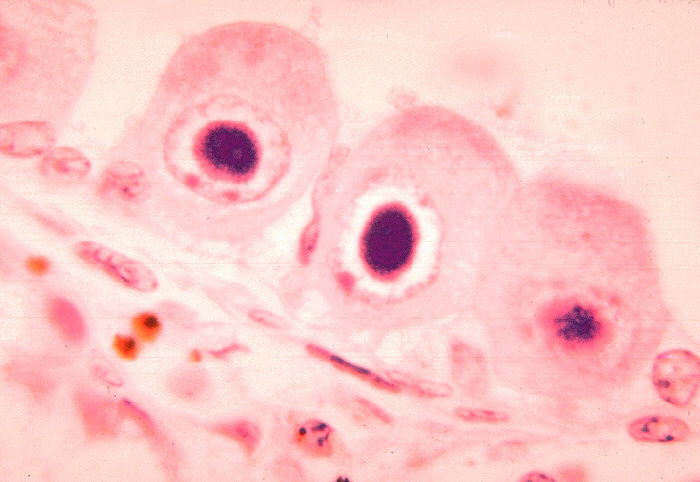
Histopathology of cytomegalovirus infection of kidney=
http://phil.cdc.gov/PHIL_Images/06011999/00016/09G0036_lores.jpg
{kind=link}
Description: Histopathology of cytomegalovirus infection of kidney.
High Resolution:High resolution download is not available for this image
Content Providers(s):CDC/ Dr. Haraszti
Creation Date:1964
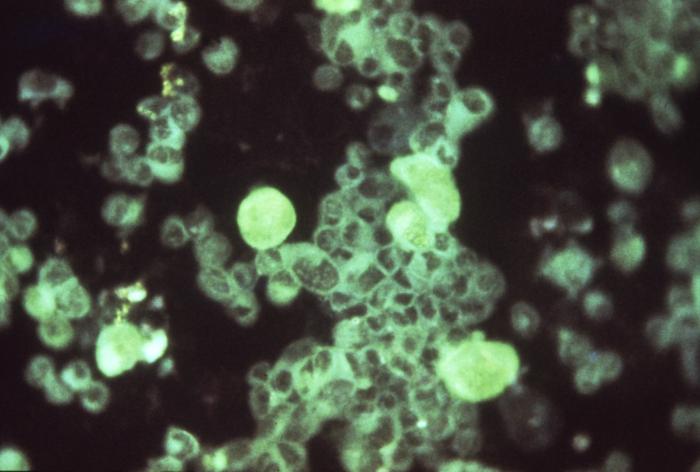
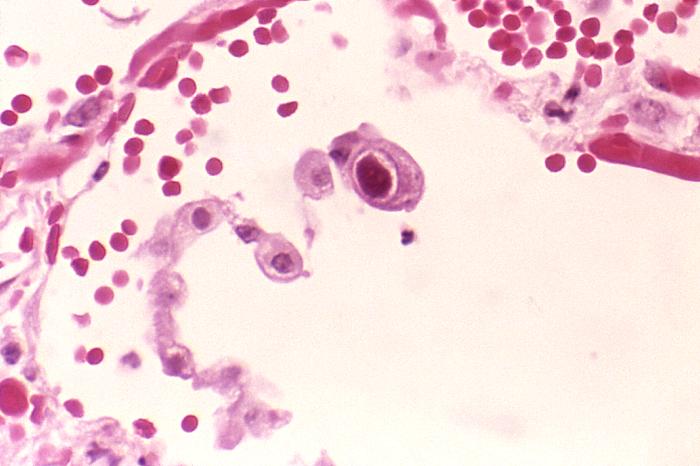
Active cytomegalovirus infection of lung in AIDS
http://phil.cdc.gov/PHIL_Images/958/958_lores.jpg
{kind=link}
Description:Active cytomegalovirus infection of lung in AIDS.
Histopathology of lung shows cytomegalic pneumocyte containing characteristic intranuclear inclusion.
High Resolution:Right click here and select "Save Target As..." for hi-resolution image (6.52 MB)Content Providers(s):CDC/ Dr. Edwin P. Ewing, Jr.Creation Date:1982Copyright Restrictions:None - This image is in the public domain and thus free of any copyright restrictions. As a matter of courtesy we request that the content provider be credited and notified in any public or private usage of this image.