File:Placenta spiral artery conversion.jpg: Difference between revisions
No edit summary |
No edit summary |
||
| Line 11: | Line 11: | ||
'''SMC''' - smooth muscle cells | '''SMC''' - smooth muscle cells | ||
'''Links:''' [[:File:Uterine_and_placental_vasculature.jpg|Figure - Uterine and placental vasculature]] | |||
===Reference=== | |||
<pubmed>19375795</pubmed>| [http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2697319 PMC2697319] | |||
Placenta. 2009 June; 30(6): 473–482. doi: 10.1016/j.placenta.2009.02.009. | |||
Copyright © 2009 Elsevier Ltd. “This is an unofficial translation of an article that appeared in an Elsevier publication. Elsevier has not endorsed this translation.” | Copyright © 2009 Elsevier Ltd. “This is an unofficial translation of an article that appeared in an Elsevier publication. Elsevier has not endorsed this translation.” | ||
http://www.elsevier.com/wps/find/authorsview.authors/supplementalterms1.0 | http://www.elsevier.com/wps/find/authorsview.authors/supplementalterms1.0 | ||
[[Category:Placenta]] [[Category:Cartoon]] | [[Category:Placenta]] [[Category:Cardiovascular]] [[Category:Cartoon]] | ||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Revision as of 08:56, 16 August 2010
Diagrammatic representation (not to scale) of the effects of spiral artery conversion on the inflow of maternal blood into the intervillous space and on lobule architecture predicted by modelling.
Dilation of the distal segment in normal pregnancies will reduce the velocity of incoming blood, and the residual momentum will carry the blood into the central cavity (CC) of the lobule, from where it will disperse evenly through the villous tree. Transit time to the uterine vein is estimated to be in the order of 25–30 s, allowing adequate time for oxygen exchange.
The pressure of the maternal blood, indicated in mmHg by the figures in blue, will drop across the non-dilated segment of the spiral artery, the dimensions of which are given alongside.
In pathological pregnancies, where no or very limited conversion occurs, the maternal blood will enter the intervillous space at speeds of 1–2 m/s. The high Reynolds number predicts turbulent flow, indicated by the circular arrows. We suggest that the high momentum ruptures anchoring villi (asterisked) and displaces others to form echogenic cystic lesions (ECL) lined by thrombus (brown). The transit time will be reduced, so that oxygen exchange is impaired and blood leaves in the uterine vein with a higher oxygen concentration than normal. Trophoblastic microparticulate debris (dotted) may be dislodged from the villous surface, leading to maternal endothelial cell activation. Finally, the retention of smooth muscle cells (SMC) around the spiral artery will increase the risk of spontaneous vasoconstriction and ischaemia–reperfusion injury.
ECL - echogenic cystic lesions
SMC - smooth muscle cells
Links: Figure - Uterine and placental vasculature
{kind=link}
Reference
<pubmed>19375795</pubmed>| PMC2697319
Placenta. 2009 June; 30(6): 473–482. doi: 10.1016/j.placenta.2009.02.009.
Copyright © 2009 Elsevier Ltd. “This is an unofficial translation of an article that appeared in an Elsevier publication. Elsevier has not endorsed this translation.”
http://www.elsevier.com/wps/find/authorsview.authors/supplementalterms1.0
File history
Click on a date/time to view the file as it appeared at that time.
| Date/Time | Thumbnail | Dimensions | User | Comment | |
|---|---|---|---|---|---|
| current | 10:26, 16 August 2009 | 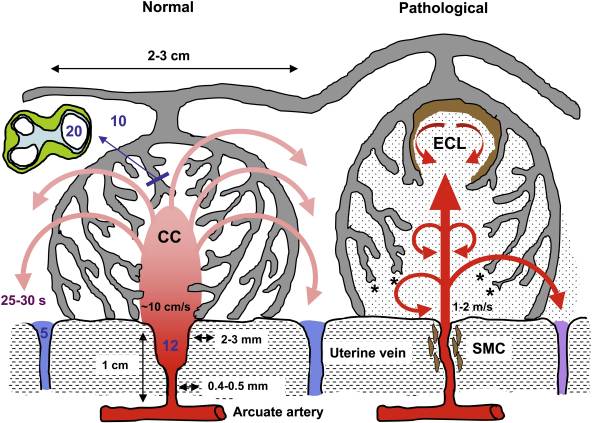 | 592 × 423 (65 KB) | S8600021 (talk | contribs) | Diagrammatic representation (not to scale) of the effects of spiral artery conversion on the inflow of maternal blood into the intervillous space and on lobule architecture predicted by modelling. Dilation of the distal segment in normal pregnancies wil |
You cannot overwrite this file.
{kind=link}