File:Hertig1956 plate16.jpg: Difference between revisions
(Z8600021 uploaded a new version of File:Hertig1956 plate16.jpg) |
mNo edit summary |
||
| Line 1: | Line 1: | ||
==Plate 16== | |||
Two abnormal ova showing malposition of the germ disc and, in one of the specimens, shallow implantation. Whether these ova would ultimately have aborted it is impossible to say. | |||
81 A surface view of the normal appearing implantation site of the abnormal ovum shown in figure 82. Note endometrial defect. over the ovum, normal for this stage of development. [[:Category:Carnegie Embryo 8299|Carnegie 8299]], Sequence 4. X 22. | |||
82 A medium-power view of the section through the greatest diameter of a 12-day abnormal ovum shown in figures 81 and 83. Note the malposition of the embryonic disc. The normal amniotic development indicates that the malorientation is of recent development since the amnion has been shown to delaminate in situ from adjacent trophoblast at about 7 days of age (Hertig, ’-15). Hence it appears that this normal appearing embryonic. disc has only recently shifted its position due to some unknown factor. It is possible that this maloricntation would have been corrected as the ovum grew and that tile germ disc would have become reoriented. Whether this patient would have aborted ultimately it is impossible to predict, though probably not. It is impossible to say what effect, if any, such an abnormality would have upon the development of the body stalk and the embryo. [[:Category:Carnegie Embryo 8299|Carnegie 8299]], Section 11-4-5. X 100. | |||
83 A surface view of the posterior wall of a uterus showing the position and sim of the implantation site shown in figures 81 and 82. [[:Category:Carnegie Embryo 8299|Carnegie 8299]] | |||
84 A low-power view of a section of an abnormal 13-day villous ovum showing shallow implantation and malorientation of the germ disc. Note polypoid type of implantation which may have resulted from failure of proper trophoblastic development at the embryonic pole. The polypoid protrusion may have caused mechanical pressure from the opposite wall of the uterus resulting in distortion of the chorionic. cavity with consequent buckling of the germ disc. This feature is shown in detail in figure 86. [[:Category:Carnegie Embryo 8290|Carnegie 8290]], Section 25-2-4. X 20. | |||
85 Profile view of implantation site of ovum shown in figures 8-1 and 86. Note polypoid structure due to shallow implantation of ovum rather than to intrinsic endomctrial polyp formation. The superficial hemorrhage is normal. [[:Category:Carnegie Embryo 8290|Carnegie 8290]], Sequence 7. X 5. | |||
86 A medium-power view of a section of the abnormal ovum shown in figures 84. and 85. Note the malorientation of the embryonic disc with a portion of it still attached to the poorly developed avillous trophoblast at the embryonic pole. The fate of an ovum such as this is unpredictable. This shallowly implanted ovum. with its excellent nbembryonic trophoblast, potentially capable of covering the internal 0a, is possibly related to llofl‘meier’s concept of the etiology of placenta previa. It is interesting to note that 8 months prior to h,vsterectom_v this patient (a para X), delivered a slightly premature stillborn baby whose death was caused by placenta previa, a condition which tends to be somewhat repetitive. [[:Category:Carnegie Embryo 8290|Carnegie 8290]], Section 25-2-4. X 100. | |||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Revision as of 23:39, 22 February 2017
Plate 16
Two abnormal ova showing malposition of the germ disc and, in one of the specimens, shallow implantation. Whether these ova would ultimately have aborted it is impossible to say.
81 A surface view of the normal appearing implantation site of the abnormal ovum shown in figure 82. Note endometrial defect. over the ovum, normal for this stage of development. Carnegie 8299, Sequence 4. X 22.
82 A medium-power view of the section through the greatest diameter of a 12-day abnormal ovum shown in figures 81 and 83. Note the malposition of the embryonic disc. The normal amniotic development indicates that the malorientation is of recent development since the amnion has been shown to delaminate in situ from adjacent trophoblast at about 7 days of age (Hertig, ’-15). Hence it appears that this normal appearing embryonic. disc has only recently shifted its position due to some unknown factor. It is possible that this maloricntation would have been corrected as the ovum grew and that tile germ disc would have become reoriented. Whether this patient would have aborted ultimately it is impossible to predict, though probably not. It is impossible to say what effect, if any, such an abnormality would have upon the development of the body stalk and the embryo. Carnegie 8299, Section 11-4-5. X 100.
83 A surface view of the posterior wall of a uterus showing the position and sim of the implantation site shown in figures 81 and 82. Carnegie 8299
84 A low-power view of a section of an abnormal 13-day villous ovum showing shallow implantation and malorientation of the germ disc. Note polypoid type of implantation which may have resulted from failure of proper trophoblastic development at the embryonic pole. The polypoid protrusion may have caused mechanical pressure from the opposite wall of the uterus resulting in distortion of the chorionic. cavity with consequent buckling of the germ disc. This feature is shown in detail in figure 86. Carnegie 8290, Section 25-2-4. X 20.
85 Profile view of implantation site of ovum shown in figures 8-1 and 86. Note polypoid structure due to shallow implantation of ovum rather than to intrinsic endomctrial polyp formation. The superficial hemorrhage is normal. Carnegie 8290, Sequence 7. X 5.
86 A medium-power view of a section of the abnormal ovum shown in figures 84. and 85. Note the malorientation of the embryonic disc with a portion of it still attached to the poorly developed avillous trophoblast at the embryonic pole. The fate of an ovum such as this is unpredictable. This shallowly implanted ovum. with its excellent nbembryonic trophoblast, potentially capable of covering the internal 0a, is possibly related to llofl‘meier’s concept of the etiology of placenta previa. It is interesting to note that 8 months prior to h,vsterectom_v this patient (a para X), delivered a slightly premature stillborn baby whose death was caused by placenta previa, a condition which tends to be somewhat repetitive. Carnegie 8290, Section 25-2-4. X 100.
File history
Click on a date/time to view the file as it appeared at that time.
| Date/Time | Thumbnail | Dimensions | User | Comment | |
|---|---|---|---|---|---|
| current | 23:38, 22 February 2017 | 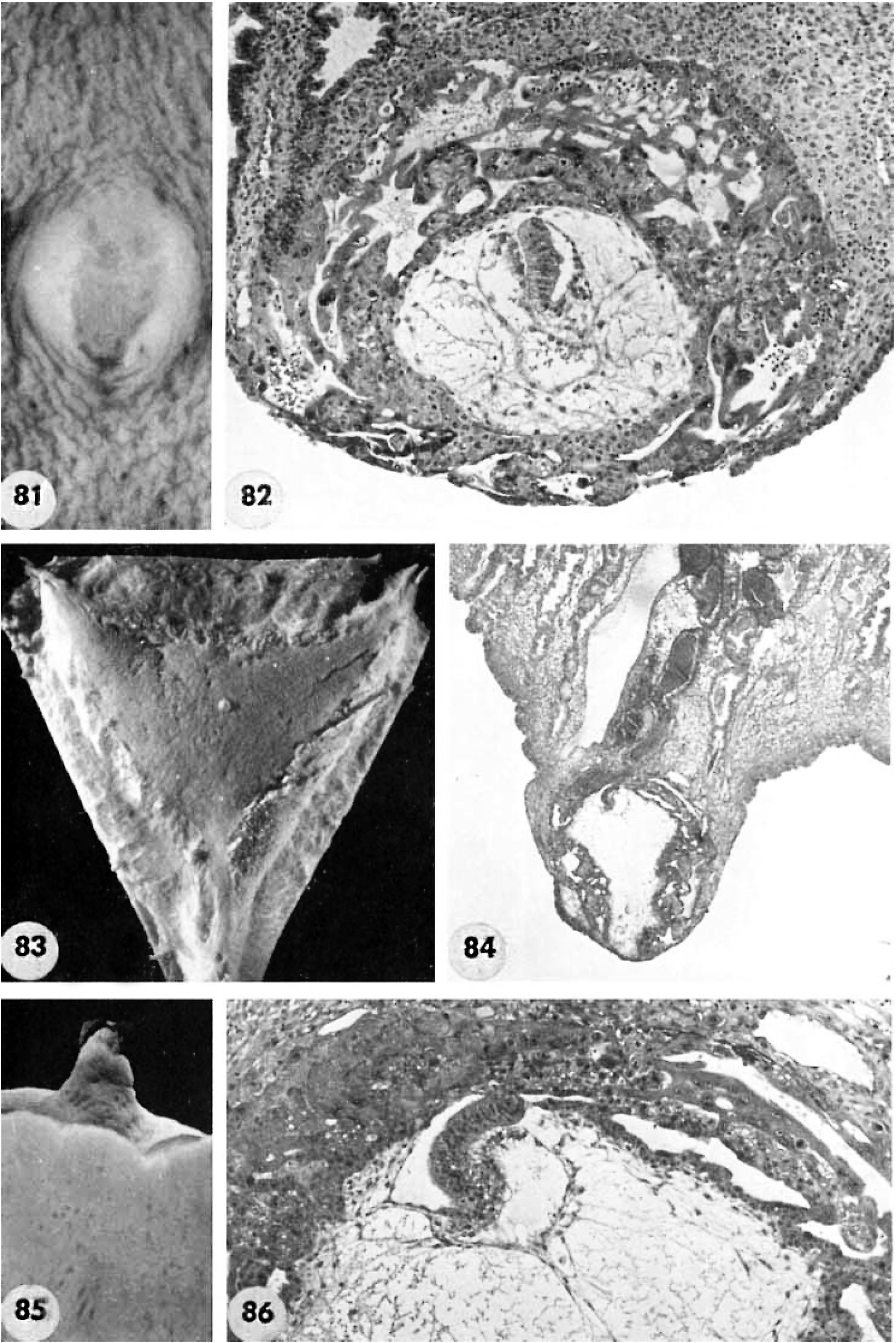 | 1,488 × 2,230 (590 KB) | Z8600021 (talk | contribs) | |
| 23:38, 22 February 2017 | 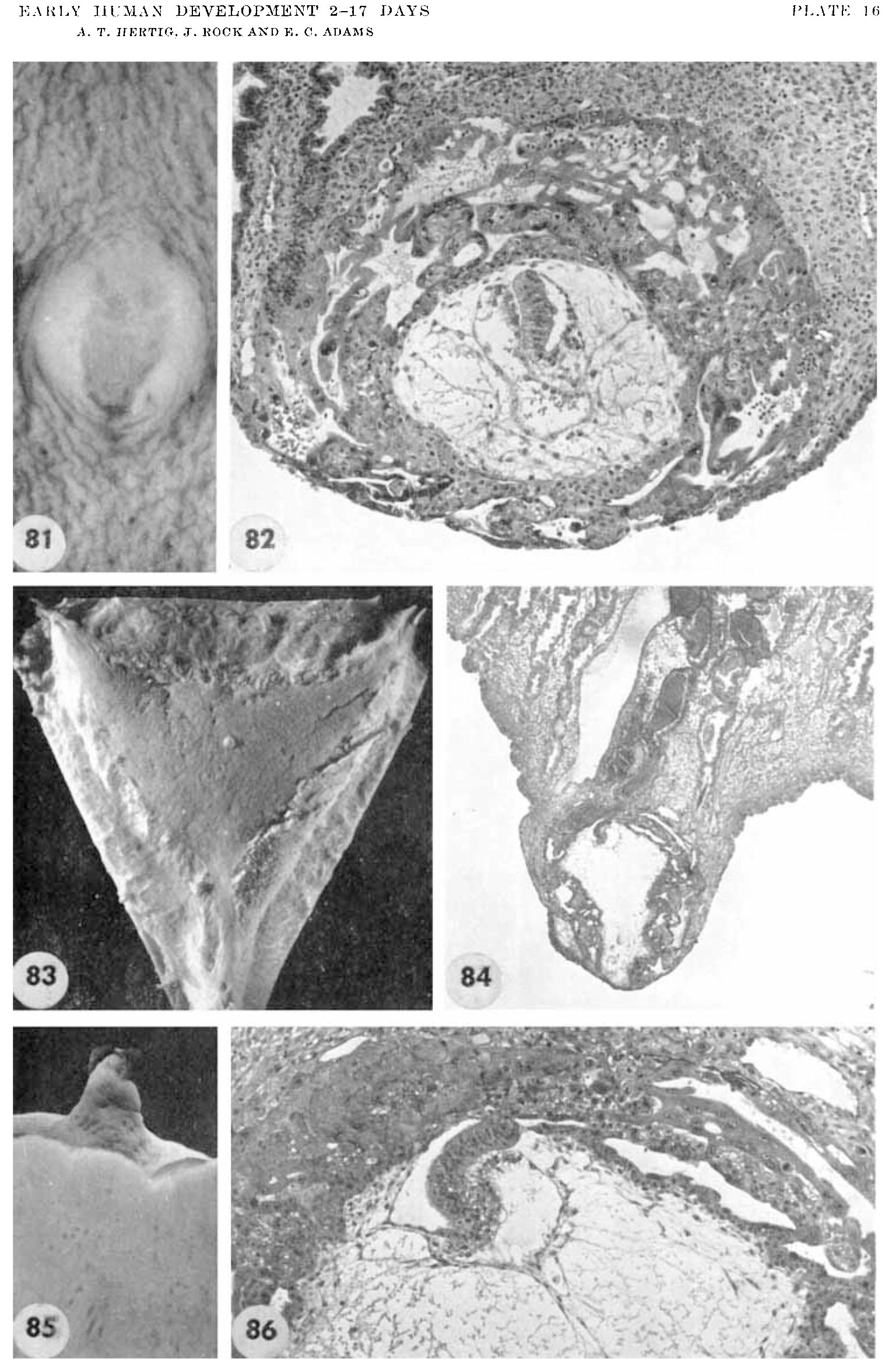 | 1,537 × 2,353 (521 KB) | Z8600021 (talk | contribs) |
You cannot overwrite this file.
File usage
The following page uses this file:
{kind=link}