Book - Umbilicus (1916) 1
| Embryology - 17 Apr 2026 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Cullen TS. Embryology, anatomy, and diseases of the umbilicus together with diseases of the urachus. (1916) W. B. Saunders Company, Philadelphia And London.
| Historic Disclaimer - information about historic embryology pages |
|---|
 |
Chapter I. Embryology of the Umbilical Region
General Considerations
A comprehensive study of the diseases of the umbilicus necessarily calls for a thorough knowledge of the embryology of this region. In early fetal life, however, the changes are so rapid and varied that they might well be termed kaleidoscopic ; hence it becomes somewhat difficult to follow the various steps in the development of the umbilicus.[1]
Among the various authors who have discussed the diseases of the urachus and
who have dwelt briefly upon its development may be mentioned Cazin (1862),
Ahlfeld (1876), Freer (1887), Ledderhose (1890), Monod (1899), and Vaughan
(1905). The literature on the embryology of the umbilicus is, however, on the
whole very meager.
In order that the gradual development of the umbilicus may be clearly understood, it is necessary to begin with a very young embryo. Fig. 1 represents an embryo 0.7 mm. long. The embryo forms only a very small portion of the specimen.
On its dorsal surface, and forming a sort of cap, is the amnion (colored green).
The yolk-sac is relatively large, and lies in front of the embryo. Connecting
all the fetal structures with the placenta is the body-stalk. It will be noted
even at this stage that a portion of the yolk-sac is projecting into the body-stalk.
This is the commencement of the allantois, which is in reality a recess of the
yolk-sac.
When the embryo is about 1.7 mm. long (Fig. 2), its outlines are well defined
and the heart is clearly seen. The amniotic cavity is much larger, and the amnion,
both above and below, extends farther forward than the embryo. The yolk-sac,
although larger, has not kept pace in growth with the embryo and the amnion.
It is continued upward in the embryo, forming the fore-gut, and downward, forming the hind-gut. The allantois has projected farther into the body-stalk. At this period a depression exists where the amnion and yolk-sac join; this marks the in

Fig. 1. Sagittal Section Showing a Very Early Stage in the Formation of the Umbilicus and Allantois. (Human embryo, 0.7 mm. long.) Note the origin of the allantois from the cavity of the yolk-sac. The umbilical region will be formed by a gradua approximation of the cranial and caudal ends of the yolk-sac, as indicated by the arrows. The embryonic surface of the yolk-sac will later become the alimentary canal.

Fig. 2. A More Advanced Stage in the Formation of the Umbilical Region. (Human embryo, 1.7 mm. long. - Mall series, 391.) (This embryo has been very carefully described by Dr. Walter E. Dandy (Amer. Jour. Anat., 1910, x, 85).
Note the advancing approach of the cranial and caudal portions of the yolk-sac and its division into a main cavity and two recesses, the fore-gut and the hind-gut, into the latter of which the allantois now opens. The vitelline arteries and veins are clearly seen on the embryonic side of the yolk-sac. The amnion is now gradually enveloping the embryo. Compare the situation of the coelom in this with that in the subsequent pictures. There is as yet no umbilical cord. For the first stage of its development, Bee Kin. 3. folding of the exocoe1om. The arrows indicate the direction that it will follow later.
In Fig. 3 we have a composite picture representing the appearances in an embryo 2.5 mm. long. The embryo has now assumed a definite form, and many of its structures can be traced. The amnion has continued to grow and now almost completely encircles the embryo. The yolk-sac has increased little, if any, in size.

Fig. 3. A Composite Picture Showing the Formation of the Umbilicus in an Embryo 2.5 mm. Long. This drawing was made after a careful study of several embryos of this length described in the literature. Each author was interested in some particular region, but not in the embryo as a whole. The yolk-sac has now become greatly narrowed at its entrance into the body. The narrowed portion is now referred to as the vitelline or omphalomesenteric duct. In its wall are seen the right omphalomesenteric vessels. The digestive tract already shows well defined differentiation. The allantois now opens into the cloaca. The amnion almost completely encircles the embryo, and in so doing has combined the vitelline duct with the body-stalk, containing the chorionic vessels and the allantois, into a common cord. As the development advances this cord will become more compact, thinner, and longer. The exocoelom has been drawn into the embryo and will later unite with the coelom of the pleuroperitoneal cavity.
It has been forced away from the embryo by the increase in development of the embryo and of the amnion. The narrowed portion of the yolk-sac is now called the omphalomesenteric or vitelline duct. This duct naturally communicates with the digestive tract, which is now becoming more and more differentiated. The digestive tract ends below in the cloaca.
We can now for the first time really speak of an umbilical cord. This consists of the body-stalk and the omphalomesenteric duct, which have as yet not fused.
The portion of the yolk-sac now forming the cloaca has been carried far back, and opening into it is the allantois, which can be followed out in the body-stalk almost to the placenta. It terminates in a bulbous extremity. Its caliber in the cord may vary considerably.
At this stage the exoccelom has been carried in between the amnion and the yolk-sac. It fills in the space around the omphalomesenteric duct, and is destined to join the pleuroperitoneal cavity.

Fig. 4. A Diagrammatic Representation of a Human Embryo, about 3.5 mm. Long, Showing the Effect of the Expanding Amnion upon the Yolk-sac and Body-stalk. The amnion has now completely encircled the embryo, and with its increase in size has crowded the yolk-sac away. Outside the amnion the yolk-sac and body-stalk are separate structures; inside the amniotic ring they are fused, forming the umbilical cord. The amnion covers the cord as far as the embryo. It is probable that the tension produced on the yolk-Stalk by the amnion contributes to the primitive kink in the alimentary canal.
In Fig. 4 we have a diagrammatic representation of a human embryo 3.5 mm. long. The embryo is completely encircled by the amnion. The yolk-sac is somewhat larger than before, but is smaller than the fetal sac. The umbilical cord is formed of the body-stalk and omphalomesenteric duct. Externally to the amnion they are separate and distinct; within the cavity they are held together by a sheath consisting of amnion.
Fig. 5 represents a human embryo 5 mm. in length. The amnion is now much
larger than the yolk-sac, and the portion of the omphalomesenteric duct external
to the sac has become much smaller than the body-stalk. The esophagus, stomach,
liver, pancreatic buds, and first curve of the small intestine are clearly visible.
Attached to this, and extending out into the cord, is the omphalomesenteric or
vitelline duct, accompanied by the omphalomesenteric vessels. The allantois, which opens into the cloaca, can be followed outward in the cord almost to the
placenta. The cord now contains the omphalomesenteric duct and its vessels,
surrounded by exoccelom, as well as the two umbilical arteries, the umbilical vein,
and the allantois. By the time the embryo is 10 mm. long (Fig. 8) the yolk-sac is
relatively very small, the cord is well formed, and in its outer portion already shows some tendency to twist. The small intestine still consists of one loop, and the
greater portion of it has been drawn out into the cord apparently by the omphalomesenteric duct or its vessels. It lies in a cavity — the exoccelom. The
umbilical cord, on section near the fetus, is now seen to contain the umbilical vein,
the exoccelomic cavity with the major part of the small intestine and the omphalomesenteric vessels lying in it; in the lower wall of the cord the umbilical arteries
appear with the allantois between them.

Fig. 5. Sagittal View of a Human Embryo 5 mm. in Length.
In large part the left halves of the amnion and embryo have been removed, in order to bring clearly into view
the structure of the cord. The expanding amnion has almost reached the chorion, hence but little remains of the
extra-amniotic portion of the yolk-stalk and of the body-stalk. The umbilical cord has become longer. The caudal
portion of the cord is firm and contains the umbilical arteries and veins; the latter, soon pfter leaving the body, form
a common trunk, which usually curves toward the left. Between the two umbilical arteries lies the allantois, the
bulbous end of which still persists almost to the amnion. The cranial portion of the cord is looser in texture. It
contains the coelomic cavity, in which lies the omphalomesenteric duct, accompanied by its vessels. Note that the
superior mesenteric vein empties into the omphalomesenteric vein behind the pancreatic buds. The omphalomesenteric
artery still arises by several branches from the aorta.

Fig. 6. Anterior View and Transverse Section of a Human Embryo 7 mm. Long, Showing the Umbilical Region.
The umbilical cord has been cut off near the embryo in order to show the thick lower portion containing the umbilical vessels and allantois. The upper portion consists mainly of the exoccelomic cavity, which contains the intestinal loop and the omphalomesenteric vessels. The omphalomesenteric duct has been drawn to the right, in order that it may be more clearly seen. Note the narrow coelomic ring through which the intestine and vessels emerge. At the outer end of the intestinal loop the omphalomesenteric duct begins.
The lower diagram represents a transverse section of the body at the level indicated in the upper picture. The purpose of this diagram is to show the shifting of the left umbilical vein toward the mid-line of the body, as a result of the ventral growth of the body-wall. The right umbilical vein is destined to disappear.
By the time the embryo has reached 18 mm. in length (Fig. 10) the small intestine shows numerous convolutions, and nearly all the small bowel lies in the exoccelomic cavity in the cord outside of the embryo.
In a longitudinal section of the cord near the body, in an embryo 23 mm. in length (Fig. 11), the exoccelomic cavity is seen to contain convolutions of small bowel, having attached to them the omphalomesenteric vessels. In the lower wall of the cord are the umbilical arteries, the umbilical vein, and the allantois.
The small, cyst-like spaces in the wall of the cord are partially organized areas of
exocoelom.
By the time the embryo is 3 cm. long the exoccelomic cavity in the cord contains many loops of small bowel (Fig. 12).
With the growth of the embryo the intestines rapidly recede into the abdomen (Fig. 15). The exoccelom and all traces of the omphalomesenteric duct and its vessels disappear, but remnants of the allantois may or may not persist in the cord.
After this short survey of the gradual development of the umbilical region of the embryo it may be well to trace briefly the individual structures.

Fig. 7. Sagittal Section of the Umbilical Region in an Embryo 7 mm. in Length. This is a reconstruction from the Mall embryo No. 2. A detailed description of this embryo by Mall will be found in the Journal of Morphology, 1S91, vol. v, p. 459. The exoccelom in the cord contains the omphalomesenteric stalk, in the body of which are seen the omphalomesenteric vessels and the duct. The connection of the duct with the intestine has disappeared, but the duct still persists in the cord and shows a bulbous dilatation at its proximal end. If it still persists in later life, we shall have a cyst in the abdominal wall or in the structures of the umbilicus. The junction of the superior mesenteric vein with the omphalomesenteric vein is clearly seen in the mesentery.
The Amnion
A clear idea of the way in which the amnion develops is essential, inasmuch as this membrane plays an important role in the formation of the umbilical cord, and occasionally of the umbilical region itself. In the very early embryo (Fig. 1) it is a small, flaccid sac, covering the posterior surface of the embryo.
By the time the embryo reaches 1.7 mm. in length (Fig. 2), the amnion has increased in size to such an extent that it not only covers the posterior surface of the embryo, but has also extended beyond the head and tail, and already shows a tendency to arch over the anterior surface.
When the embryo reaches 2.5 mm. in length, the amnion is seen to have almost engulfed the embryo, surrounding it on all sides except where the yolk-sac and bodystalk enter its ventral surface. Fig. 3 clearly indicates that the expansile force of the amnion and of the embryo has pushed the major portion of the yolk-sac away leaving only its narrowed portion — now called the omphalomesenteric duct — to connect it with the digestive tract.
Fig. 4 shows the amniotic sac of an embryo 3.5 mm. long. Here the fetus and the major portion of the omphalomesenteric duct and of the body-stalk are contained in the amniotic cavity, which is approximately spherical.
By the time the embryo is 5 mm. in length the amniotic sac is much larger than the yolk-sac (Fig. 5), and the amnion is reflected in on the cord to the umbilicus. In rare instances, as noted on page 67, when the skin is lacking at the umbilicus, the amnion covers over this defect, forming an amnion umbilicus.

Fig. 8. Sagittal View of the Umbilical Region of a Human Embryo 10 mm. in Length.
The yolk-sac now lies far removed from the umbilical cord; its vessels and stalk follow a tortuous course. The
umbilical cord here shows the first indication of a twist, which may be caused by the embryo rotating toward the right.
In the embryos examined by us there has been but one exception to this rule. The small intestine extends a
considerable distance into the exocoelom of the cord. At the outer end of the intestinal loop is situated the delicate
omphalomesenteric duct. The omphalomesenteric vein passes on the left side of the intestinal loop; the artery, on the
right side.
When the embryo reaches 10 mm. in length, the amnion is well developed (Fig. 8). The amnion of an embryo 23 mm. long (Fig. 11) presents essentially the same picture.

Fig. 9. Graphic Reconstruction of the Umbilical Cord of a Human Embryo 12.5 mm. in Length. (Mall collection, No. 317.)
The figure to the left shows the manner in which the cord has been cut into the portions I, II, and III. On the right are shown frontal views of the three sections. They are represented as being seniitransparent, in order to give a clear idea of the course of the contained structures.
Section I: Embryonic end of cord, showing ccelomic ring through which protrudes the primitive intestine. Note
the position of the proximal intestine (jejunum) and the distal intestine (ileum). To the right and above, the
omphalomesenteric vessels are seen emerging by the side of the intestine. The vein comes from above the gut and
the artery from below; between them lies the duct, which is still connected with the intestine. A delicate mesenteriolum accompanies these structures for a short distance into the cord (cf. also Fig. 7). The umbilical arteries and
vein are seen in the lower part of the cord. Here the allantois lies between the arteries and becomes obliterated.
Section II: This section of the cord is farther from the umbilicus, and shows a twist of the structures, somewhat
after the manner of the left turn of a screw. The exoccelom with its contents now lies to the right ; the umbilical vessels
and allantois have shifted to the left. The allantois has again increased in size, and lies between the umbilical arteries
and the exoccelom.
Section III: This section of the cord is still farther from the umbilicus. It shows the amniotic ring, through which
emerge the omphalomesenteric duct and its vessels. The allantois decreases rapidly in size and becomes lost between
the left umbilical artery and the umbilical vein.
The Yolk-Sac
In an early pregnancy, when the embryo is about 0.7 mm. long (Fig. 1), the yolk-sac is represented by a nearly circular cyst, intimately blended with the anterior surface of the embryo. The sac has relatively thin walls, which are traversed by delicate traceries of blood-vessels. Even in this early stage a small prolongation of the yolk-sac extends into the body-stalk. This prolongation is the beginning of the allantois.

Fig. 10. Anterior View of the Umbilical Cord of a Human Embryo 18 mm in Length. A portion of the cord has been removed, as shown by the dotted line. The exoccelomic cavity has increased materially in size and contains several loops of intestine, including the cecum and budding appendix, seen on the extreme left (right in picture). The narrow ccelomic ring is obscured by the intestine. The omphalomesenteric duct has disappeared, and we now have only the omphalomesenteric vessels passing out into the exoccelom. This more rapid disappearance of the delicate epithelial structure of the vitelline duct, as contrasted with the preservation of the stronger tissues of the blood-vessels, is probably caused by the continued tension to which the yolk-stalk is subjected. (See Figs. 11 and 12 ) The exoccelomic cavity rapidly tapers to a narrow chink, as seen in the upper and more distal section. In the mid-line of the cord below are the two umbilical arteries, with the allantois between and slightly below them. The umbilical vein lies to the left. The characteristic twist of the cord, including all of its structures, is clearly seen.
When the embryo has reached a length of about 1.7 mm. (Fig. 2), the yolk-sac is larger, but has not kept pace in development with either the embryo or the amnion. It has extended* into the anterior surface of the embryo, above forming the fore-gut, below the hind-gut. The allantois, which has originated from the yolk-sac and is still connected with it, extends much farther into the body-stalk.
- In reality it is the forward growth of the upper and lower ends of the embryo, as indicated
by the arrows, that produces the recesses destined to become the alimentary canal.
By the time the embryo is 2.5 mm. in length (Fig. 3) the yolk-sac is smaller than either the embryo or the amnion. With the increase in size of the amniotic sac the yolk-sac has been forced away from the embryo. The cavity of the yolksac, however, still communicates freely with the digestive tract by a broad channel — the omphalomesenteric or vitelline duct. During the development of the embryo and its digestive tract the allantois has been carried downward and backward. It now opens into the cloaca, and can be traced out in the body-stalk as far as the placenta.

Fig. 11. Sagittal Section of the Umbilical Region in a Human Embryo 23 mm. in Length.
The small drawing to the left, which is of natural size, accurately depicts the relation of the yolk-sac to the
cord and amnion. Its stalk is very long, and the yolk-sac has become relatively smaller. The umbilical cord now
shows very marked twisting. The exoccelomic cavity in the umbilical cord now contains practically all the intestine
with the exception of the jejunum and descending colon. The distal portion of the cavity is funnel-shaped, the apex
being directed away from the embryo. The omphalomesenteric duct has disappeared, but its vessels persist. The
small cystic spaces in the upper wall of the cord mark the beginning obliteration of the exoccelom. The umbilical
vein has been partly removed in order to bring into view the deeper structures. The two umbilical arteries, accompanied by the allantois, are in their usual position in the lower part of the cord. Note the slight spindle-shaped dilatation of the allantois in its course.
By the time the embryo is 3.5 mm. long (Fig. 4) the amnion has completely encircled the embryo. The yolk-sac has increased somewhat in size, is pear-shaped, covered with a tracery of blood-vessels, and appears to have small, shallow, cyst like elevations on its surface. It is still intimately connected with the embryo through its omphalomesenteric duct, which joins the body-stalk, passing into the amniotic sac and thence to the embryo.
When the embryo reaches 5 mm. in length (Fig. 5), the yolk-sac is about the same size. It is now beginning to play a minor role, and its omphalomesenteric duct is much smaller in caliber.

Fig. 12. A Graphic Reconstruction of the Umbilical Region of a Human Embryo 3 cm. Long. (Mall collection, No. 86.) The small sketch in the right upper corner indicates the points at which the sections of the cord have been made. This stage marks the maximal development of the exoccelom, the intestine completely filling its cavity. Section I, the nearest to the embryo, gives a frontal view of the narrow coelomic ring, which, on account of the solid tissue containing i he vascular structures below, appears in the form of a crescent. Emerging from the ring we see the small intestine to the right of the embryo, and the large intestine to the left, with the accompanying mesentery between them. In the cross-section of the mesentery are seen numerous sections of its arteries and vein. The omphalomesenteric vein passes outside of and above the mesentery; the omphalomesenteric artery comes from below, as seen in Section II. They soon leave the intestine and pass out into the funnel-shaped exocoelom.
In an embryo 10 mm. long (Fig. 8) the yolk-sac is found pushed to one side. It is now connected with the extra-amniotic portion of the umbilical cord by the attenuated omphalomesenteric duct and its blood-vessels. These present a twisted appearance. The omphalomesenteric vessels still persist in the cord near the embryo, but the duct at this point has usually disappeared.

Fig. 13. Sagittal Section of the Umbilical Region in a Human Embryo 4.5 cm. in Length. The intestine has receded completely into the abdominal cavity. The exoccelomic cavity, although small in size is still clearly recognizable in the cord, where it shows spindle-shaped dilatations. It now contains only the omphalomesenteric vessels, which have become embedded in its wall. The allantois (urachus) is the distal prolongation of the urinary bladder, and shows already the characteristic dilatations noticeable in older embryos and occasionally found after birth. The structures of the cord show the characteristic twisting of the embryo to the right.
By the time the embryo has reached a length of 23 mm. (Fig. 11) the yolk-sac is relatively insignificant, and, although still attached to the cord, is far removed from the site of its insertion into the placenta.
When the embryo is about 5.5 cm. in length (Fig. 31), the yolk-sac, now called the umbilical vesicle, is a small, translucent, elongated, and flattened cyst, about 3 by 5 mm., attached to the insertion of the cord into the placenta by a delicate
vascular thread — all that remains of the omphalomesenteric structures. The
vesicle remains about the same size until birth. It is then recognized as a small,
blunt or pear-shaped cyst, lying between the amnion and placenta (Fig. 32). Its
pedicle can be traced for a variable distance in the substance of the umbilical cord.
In short, the yolk-sac in the very beginning of life is an important structure.
From it the allantois and the gastro-intestinal tract develop, the connecting link with the body being the omphalomesenteric duct. The omphalomesenteric or
vitelline duct in time usually disappears, but, as will be noted elsewhere, traces of
the allantois not infrequently persist.

Fig. 14. A Graphic Reconstruction of the Umbilical Region op a Human Embryo 4.5 cm. in Length as viewed from within the abdomen.
Coming from below are the two umbilical arteries with the urachus between them. Above is the umbilical vein, inclosed in a bulbous thickening of the surrounding tissue. The body-wall of the embryo at the cord has closed, save for an irregular slit. The exoccelom outside the general peritoneal cavity dilates, as indicated by the dotted line; it soon becomes obliterated. Plunging into the upper corner of the exoccelom, and adherent to its wall, are the omphalomesenteric vessels, accompanied by a thick cord of embryonic connective tissue, which, near the intestine, has an epithelial center but no lumen. This is undoubtedly a remnant of the omphalomesenteric duct. The section of the cord shown above is taken from near the embryo. It depicts the characteristic position of the allantois, and the narrow, slit-like termination of the exoccelom with the omphalomesenteric vein in its wall, the artery having disappeared.
Those wishing for a more detailed description of the umbilical vesicle or yolksac, together with the histologic findings, should read the article by Arthur Meyer,
published in 1904. Meyer studied the umbilical vesicles of 18 normal human
embryos from the Mall collection. In addition he examined a number of pathologic specimens and also some taken from the placenta at birth. He pointed out
that the vesicle in the early embryo is lined with one layer of cuboidal epithelium, and that, passing out into the walls of the vesicle, are little bays or tubules. He
also drew attention to the calcareous material found in the cavity of the vesicle at
term. A further consideration of this subject here would carry us too far afield.

Fig. 15. Sagittal View of a Graphic Reconstruction of the Umbilical Region of a Human Embryo 5.2 cm. in Length.
From within, the relations of the umbilical arteries to the vein are clearly seen. They surround the funnel-shaped
remnant of the exoccelom. No trace of the omphalomesenteric vessels is to be seen in the peritoneal cavity, but in
cross-sections of the cord near the embryo the lumen of the umbilical vein still persists, as indicated in the small drawing to the left. It is embedded in the wall of the exoccelom, but has no connection with any other vascular structure.
The bladder bulges out between the umbilical arteries. The urachus (allantois) passes out into the cord between and
below the umbilical arteries. This is the characteristic arrangement. The urachus shows two dilatations.
The Body-Stalk
In the early stages the embryo rests upon the body-stalk. This fact is clearly shown in Fig. 1. The stalk at this period is much larger than the embryo. It also supports the yolk-sac and the amnion, and through it the blood-vessels of the placenta pass to and from the embryo. When the embryo reaches about 1.7 mm. in length (Fig. 2) , the body-stalk is found to be still of about the same size, but its upper or embryonic portion passes more ventral ward and its upper end lies almost directly below the hind-gut. Its blood-vessels have increased materially in diameter. With the development of the embryo and the expansion of the amnion the body-stalk becomes longer and assumes more the appearance of a cord, which is inserted into the ventral surface of the embryo. This is particularly well seen in Fig. 3, which is from an embryo 2.5 mm. long.
When the embryo reaches a length of 3.5 mm. (Fig. 4), the body-stalk closely resembles an umbilical cord. Together with the omphalomesenteric duct, it passes into the amniotic cavity, where the two fuse and become the umbilical cord.
In an embryo 5 mm. long (Fig. 5) the body-stalk, as such, lying outside the amniotic sac, is very short, the amnion lying in almost direct contact with the chorion.
The intra-amniotic portion of the body-stalk will be considered when we come to speak of the umbilical cord.
The Allantois and Urachus
The allantois is one of the first structures differentiated in the embryo. For example, in an embryo 0.7 mm. long (Fig. 1) it is recognized as a recess of the yolk-sac extending into the body-stalk. It rapidly increases in length, and in an embryo 1.7 mm. long has penetrated deeply into the body-stalk (Fig. 2).
In an embryo 2.5 mm. long (Fig. 3) a portion of the yolk-sac has been definitely differentiated into the digestive tract. Its caudal portion has been carried downward and forward, terminating in the cloaca. The allantois now starts from the cloaca, and, after curving upward, passes outward in the body-stalk to end in a bulbous extremity near the placenta.
In the embryo 5 mm. long (Fig. 5) it still communicates with the cloaca, and, after emerging from the abdomen, passes out in the body-stalk, which now forms an integral part of the umbilical cord.
By the time the embryo is 7 mm long the allantois has been partially separated from the bowel by the urorectal septum. The lower portion of the allantois has been converted into the bladder (Fig. 7), and its upper part now passes off from the fundus, extending upward and forward and passing out in the cord as heretofore.
Fig. 6, also from an embryo 7 mm long, shows the relation of the allantois to
the umbilical arteries. It lies between and slightly below them, and, whenever
found either in the early or in the late stages of fetal life or after birth, it invariably occupies this position.
The patency of the allantois in the umbilical cord varies markedly. Sometimes, even in the early embryo, the duct may be impervious at some points and
dilated at others. Thus, in an embryo 12.5 mm. long (Fig. 9) the allantois is obliterated in a cross-section of the cord near the fetus; in a second section a little farther
out in the cord it is seen as a somewhat flattened tube, nearly as large as an umbilical artery; in a third section of the cord, still farther out, the allantois forms an
irregular sac, the distal end of which terminates in a thread-like process.
Examination of an embryo 23 mm. long (Fig. 11) shows a urachus patent at the
point where it emerges from the abdomen. It then becomes impervious, and farther
out forms a delicate, spindle-like dilatation.
The intra-abdominal portion of the allantois in the well-differentiated embryo is called the urachus. Fig. 13, from an embryo 4.5 cm. long, shows the urachus passing
upward from the summit of the bladder. In some places it is recognized as a
slender filament, but in its course it has two delicate, spindle-like dilatations. The
allantois in the cord contains several similar dilatations.
As the embryo becomes larger the bladder may extend somewhat high up, reaching almost to the umbilicus. This is seen in Fig. 15, from an embrj-o 5.2 cm. long.
The urachus is short, and just where it enters the cord is seen a spindle-shaped
dilatation. A similar dilatation is noted in the outer or allantoic portion. The
upward extension of the bladder is well shown in Fig. 16. from an embryo 6.5 cm.
in length. A cross-section a little below the umbilicus shows that the bladder at this point is almost tubular. It gradually tapers off, and ends just below the
umbilical depression.

Fig. 16. Intra-abdominal View of the Umbilical Region" of a Human Embryo 6.5 cm. in" Length. (X 9.) A portion of the abdominal wall, including the umbilicus, has been excised. The bladder lies between the umbilical arteries and gradually diminishes in caliber toward the umbilicus. This is clearly seen in the cross-section projected in the lower picture. The umbilical vein emerges from the abdominal wall just above the umbilical region. The umbilical opening is closed, its former position being now recognized as several shallow pits in the peritoneum. To the left is a cross-section of the flattened cord, containing, in addition to the umbilical vessels, the allantois, which is obliterated at this point. There are no remnants of either exocoelom or omphalomesenteric structures.

Fig. 17. Intra-abdominal View of the Umbilical Region in a Human Embryo 7.5 cm. Long. (X6.) In this case the allantois (urachus) is very narrow, as seen in the cross-section of the abdominal wall, as well as in the cross-section of the cord. The tissues containing the umbilical arteries and urachus are attached to the abdominal wall by a well-defined but narrow mesentery. This, however, is exceptional. At the umbilicus the coelomic ring is obliterated and appears as a crescent between the umbilical arteries and vein. Farther out in the cord, however the exocoelom can still be clearly seen as a small, star-shaped cavity. The cord is markedly twisted.

Fig. 18. Intra-abdominal View of the Umbilical Region in a Human Embryo 9 cm. in Length. (X 7.) The urachus shows a spindle-shaped widening at its upper portion. Microscopically it could, however, be traced in its continuity not only to the umbilicus, but also out into the cord, as indicated by the cross-section of the cord, where it occupies its characteristic position in relation to the umbilical arteries. The umbilical ring is entirely bridged over by a band of subperitoneal connective tissue. A considerable space exists between the umbilical vein and the umbilical arteries. This arrangement closely resembles that noted in the adult. There is no trace of the omphalomesenteric structures in the cord.

Fig. 19. Intra-abdominal View of the Umbilical Region in a Human Embryo 10 cm. in Length. (X 6.) The urachus is very narrow, but is continued out into the cord (allantois). In this cross-section of the cord it was recognized as a nest of polygonal cells devoid of a lumen, and surrounded by several bundles of well-defined non-striped muscle. This muscle surrounded the urachus down to, and merged into, that of the bladder. The umbilical ring is completely sealed over by a broad connective-tissue band. In the cross-section of the cord no remnants of the exoccelomic cavity were demonstrable, but in its place were traces of blood-vessels, evidently remains of the omphalomesenteric vessels.

Fig. 20. Intra-abdominal View of the Umbilical Region in a Human Embryo 12 cm. Long. (X 3.)
The bladder is unusually distended, and reaches almost to the umbilicus. Both it and the umbilical vessels have
a well-defined mesenteric attachment to the abdominal wall. The bladder was closed above, and the urachus was
recognized as a solid cord. In the umbilical cord, however, the allantois showed here and there traces of a lumen.
The umbilical ring was completely closed. At its site was a crescent-shaped pit. The exocoelom had disappeared
in the cord, but traces of the omphalomesenteric vessels were still visible.
It would seem, from an examination of numerous embryos, that the degree of extension of the bladder upward is subject to much variation. Fig. 17 is from an embryo 7.5 cm long. The bladder is evidently low. Cross-sections near the bladder and also in the neighborhood of the umbilicus show a patent urachus, and a cross-section of the cord, at some distance from the body, shows that the allantois (urachus) is patent here also.

Fig. 21. Intra-abdominal View of the Umbilical Region in a Human Embryo 12 cm. in Length. (X 3.) The urachus gradually narrows, but microscopically could be traced as a cord for a considerable distance out into the umbilical cord. In the main it was solid, but here and there appeared to have a lumen. The umbilical vessels now have very well-developed muscular coats, the inner longitudinal layer being especially thick. The umbilical ring shows a puckering, possibly due to the hardening. It is obliterated. Note the oval, funnel-shaped depression between the umbilical arteries and vein. Adherent to the bottom of this is a cord which was attached to a loop of small bowel. This is the remnant of the omphalomesenteric duct or vessels. In the cord the exoccelom is recognized as a slit-like cavity traversed by delicate trabecular of young connective tissue. At one side of this slit is a dense mass of tissue containing the patent omphalomesenteric vessels, and the duct which appeared as a mass of epithelial cells but showed no lumen.
In Fig. 19, from an embryo 10 cm. long, the cord near the umbilicus shows the allantois, which, however, is obliterated and represented by a solid nest of polygonal cells surrounded by cross-sections of groups of non-striped muscle, showing that the
urachus has a longitudinal outer muscular covering.
Figs. 22 and 23, from an embryo 12 cm. long, are very instructive. Fig. 22 shows a rross-section of the abdominal wall made near the umbilicus. Here the urachus is very small and almost solid. In a section of the cord, at a short distance from the embryo, the allantois is found to be patent and surrounded by one or more layers of the characteristic polygonal cells. This polygonal character of the cells is also clearly shown in Fig. 23, which was taken from the same cord close to the abdominal wall. In Fig. 20, also from an embryo 12 cm. long, the bladder extends almost to the umbilicus.
Figs. 28 and 29 show the relation of the bladder to the umbilicus in embryos of five and about six and one-half months respectively: in both cases it extended almost to the umbilicus.

Fig. 22. Intra-abdominal View of the Umbilical Region" in a Human Embryo 12 cm. in Length. (X 3.)
The urachus is very narrow, as seen in the lower cross-section. In the cord, however, it (the allantois) has at several points a definite lumen lined with polygonal cells. The umbilical ring is completely closed. Fig. 23 gives an external view of the umbilical region of the same embryo.
From the foregoing it is seen that the allantois develops from the yolk-sac; that it is one of the earliest structures to make its appearance, and that, after a time, it is carried downward and forward, coming off from the cloaca. The bladder develops from the lower portion of the allantois. The upper portion of the allantois is continued to the umbilicus and then passes to the cord. Its intra-abdominal portion is now called the urachus.
The urachus and allantois soon become solid cords in a part of their course, but show an inherent tendency to develop spindle-like dilatations at irregular intervals. These dilatations are characteristic of the urachus and allantois, and
it should occasion no surprise if they are found at any period in the development of the embryo. They undoubtedly persist in many persons and account for the small cysts not infrequently noted at operation. That the urachus occasionally remains patent at birth is attested by the number of children with a urinary umbilical fistula at birth. This phase is discussed at length in Chapter XXIX.
The tube composing the urachus and allantois is lined with from one to three layers of transitional epithelium, similar to that of the bladder, and is surrounded by a coat of longitudinal non-striped muscle.

Fig. 23. Cross-section of the Umbilical Cord at the Umbilicus in a Human Embryo 12 cm in Length. (X 8.)
This drawing is also from the embryo shown in Fig. 22 In the upper figure the cord has been cut across about 1 mm. from the abdominal wall. The umbilical arteries are surrounded by Wharton's jelly. In the triangle below and between them is a small, opaque cord, the allantois. Above the right umbilical artery an irregular lumen, continued as a slit on either side, represents the disappearing exocoelomic cavity. The slit-like portion above the vein is already partially organized. Surrounding the entire mass is a dense layer of connective tissue, and external to this is the subcutaneous adipose tissue traversed by numerous cutaneous vessels. The lower picture shows a microscopic section still nearer the embryo. The slit-like exoccelom (c, c) stands out much more clearly. In its upper wall are seen the omphalomesenteric vessels and duct. An enlarged view of these is given on the left. Here the omphalomesenteric duct is recognized as a solid nest of epithelial cells. The allantois is visible slightly below and between the umbilical arteries, whose lumina are star-shaped. The drawing to the right shows that the allantois is patent and surrounded by polygonal cells. The allantois here is inclosed in embryonic connective tissue which is devoid of muscle.
The Coelom
Without a clear conception of the exoccelom, the early embryologic appearances of the umbilical region cannot well be understood. In the embryo 1.7 mm long (Fig. 2) a small depression exists at or near the point where the yolk-sac and amnion merge. The arrows indicate the direction that the exoccelom will later follow.
When the embryo has reached a length of 2.5 mm (Fig. 3), the exoccelom has extended inward between the yolk-sac and amnion; it now completely encircles the omphalomesenteric duct, and has extended upward toward the stomach and downward toward the cloaca. From this picture it can be readily understood why at a later stage the omphalomesenteric duct and its vessels lie in the exoccelomic cavity in the umbilical cord.
The exoccelom, which has extended into the embryo, later unites with the coelomic or pleuroperitoneal cavity.
By the time the embryo reaches a length of 5 mm (Fig. 5) the body-stalk and
the omphalomesenteric duct with its vessels have merged into the umbilical cord, and with the fusion it is but natural that the omphalomesenteric structures should
still be surrounded by the exoccelom. The portion of the ccelom outside the abdomen is referred to as the exoccelom, whereas the intra-abdominal portion, with
which it is still continuous, is called the ccelom.
Fig. 24. — Internal View of the Umbilical Region in a Human Embryo 15 cm. Long. (X 4). The urachus is very much attenuated, but is still continuous as a cord, with the partially obliterated allantois seen in the cross-section of the cord. The umbilical ring is closed by a firm transverse fibrous band.
As the embryo continues to develop, the omphalomesenteric duct, which is still a part of the small bowel and lies in the exoccelom, evidently makes traction on the gut and draws it out into the exoccelomic cavity. In an embryo 7 mm. long this cavity (Fig. 6) contains the cecum. In another embryo of the same length (Fig. 7) the free opening between the ccelom and the exoccelom of the cord is clearly depicted.
When the embryo reaches a length of 10 mm. (Fig. 8), the small bowel, which consists of one long loop, is found extending for quite a distance out into the cord.
It lies free in the exoccelom, and is accompanied by the vessels of the omphalomesenteric duct. A somewhat similar picture was noted in the cord of an embryo 12.5
mm. long (Fig. 9).
Fig. 25. — A Composite Representation of Abnormal Umbilical Structures Based on the Work op Keibel, Lowy, and Others. The bladder gradually tapers into the urachus and is obliterated at the umbilicus. In the cord are seen numerous dilatations of the allantois (urachus). The omphalomesenteric duct (Meckel's diverticulum) goes to the umbilicus, where it becomes lost in the ecelomic funnel. It is accompanied by the omphalomesenteric vessels. The artery terminates in its wall; the vein continues and becomes lost in the exoccelom of the cord.
{kind=link}
Fig. 26. A Composite Representation of Abnormal Umbilical Structures Based on the Work of Keibel, Lowy, and Others. The allantois in the cord shows one large and one small dilatation. The large dilatation is lined with one layer of flattened epithelium. The obliterated cord between the dilatations consists of closely packed epithelial cells. The inner end of the omphalomesenteric duct persists as a sac-shaped Meckel's diverticulum. Its vessels continue on into the coelomic funnel at the umbilicus, but become lost in the exocoelom of the cord.
{kind=link}
Fig. 27. A Composite Representation of Abnormal Umbilical Structures Based on the Work of Keibel, Lowy, and Others. The allantois shows numerous spindle-shaped dilatations in the cord, with obliterated portions between. The omphalomesenteric duct has disappeared, but the vessels still persist, the vein continuing farther out than the artery.

Fig. 28. The Umbilical Region in a Fetus about Five Months Old Viewed from the Left. Note the portion of the triangular falciform Ligament between the umbilical vein and the ventral abdominal wall. The bladder and allantois (urachus) are in the usual position; the latter is becoming obliterated. In the cord it appears below and between the umbilical arteries. In the center of the cord is the sickle-shaped lumen of the exoccelom, which, however, is bridged over in many places by delicate strands of connective tissue. In the abdomen a shallow pit still marks the position of the umbilical ring.
{kind=link}
Fig. 29. Side and Posterior Views of the Umbilical Region in a Fetus of Six to Seven Months. The left figure shows the characteristic recesses (a, b) between the umbilical artery and the abdominal wall. (See also Figs. 17, 20, and 24.) The bladder reaches nearly to the umbilicus, the urachus being very short. In the section of the cord shown, neither the allantois nor the omphalomesenteric structures could be demonstrated. The falciform ligament of the liver is very short ; hence the close union between the umbilical vein and the abdominal wall. The umbilical ring is closed by a broad band of connective tissue. The figure to the right shows the characteristic triangular shape of the upper part of the bladder, and also its sudden narrowing into the urachus above.
With the continued development of the embryo and the simultaneous increase in the number of the intestinal loops, more and more of the intestine develops in the exoccelomic cavity. Fig. 10 represents the findings in an embryo 18 mm. long; Fig. 11, those in an embryo 23 mm. in length.
The maximal size of the exoccelomic cavity in the cord is probably reached when
the embryo is about 30 mm in length (Fig. 12). In this picture the exoccelomic
cavity appears to the right of the solid portion of the cord. It contains nearly all
of the bowel.
By the time the embryo has reached a length of 4.5 cm (Figs. 13 and 14) the
intestine has receded into the abdomen and a section of the cord near the body will
reveal only a trace of the exoccelomic cavity. This is recognized as a more or less
triangular slit, containing only the omphalomesenteric vessels. In Fig. 15, taken
from an embryo 5.2 cm. long, a small exoccelomic cavity still exists, and adherent to
its upper wall is the patent omphalomesenteric vein.
Even in embryos 12 cm long (Figs. 21 and 23) slit-like traces of the exoccelom
may be found in the cord near the fetus.
To the clinician the chief interest in the exocoelom lies in the fact that in rare instances the intestine does not entirely recede, but remains incarcerated in this extra-abdominal cavity, giving rise to the large ventral hernise occasionally noted at birth.
The Umbilical Vessels
These consist of two arteries, and in the beginning of two veins, the right and the left. The left vein is the larger and persists; the right disappears before the embryo is 10 mm. long.
Even in the very early embryo, 0.7 mm long (Fig. 1), the umbilical arteries and
veins are seen in the body-stalk. At this stage they convey the placental blood
to and from the primitive embryo. By the time the embryo is 1.7 mm. long
(Fig. 2) the umbilical arteries, after passing along the primitive digestive tract,
enter the body-stalk beside the allantois and divide into many placental branches.
Just before entering the embryo, the umbilical vein divides into two branches.
These pass up the right and left abdominal wall to unite with the hepatic circulation.
In the embryo 2.5 mm in length (Fig. 3), the cord is seen to contain two umbilical arteries and one umbilical vein, which at the embryo divides into two trunks,
the right and the left. The umbilical arteries pass downward toward the caudal
extremity of the embryo ; the vein goes upward toward the liver.
When the embryo has reached 5 mm in length (Fig. 5), we still find the two
umbilical arteries, which, after passing along the cord, enter the ventral surface of
the embryo and pass downward.
Fig. 6, from an embryo 7 mm long, shows clearly the relations of the right and
left umbilical veins. The left umbilical vein is very large and runs upward to the liver. The right vein is much smaller, lies partly embedded in the abdominal wall,
and is soon completely lost.
In the embryo 23 mm long (Fig. 11) the umbilical vein is clearly seen entering
the substance of the liver. The umbilical arteries, in the cord as well as in the
abdomen, lie on either side of the allantois. They pass downward to the pelvis.
In the embryo 4.5 cm. long (Fig. 13) the vein is seen at the umbilicus, curving
from the lower to the upper portion of the cord, and passing directly into the substance of the liver, which at this time reaches almost to the umbilicus. The umbilical arteries at this period in the development of the embryo, after passing to
either side of the allantois (urachus), skirt along each side of the bladder. They
originate from the lower portion of the aorta.
The subsequent relation of the umbilical vessels is clearly depicted in Figs. 28 and 29. The relation of the umbilical vessels at term is well shown in Fig. 30.
The umbilical vein is of large size, and passes directly from the umbilicus to the
substance of the liver. It is supported by the suspensory ligament of the liver, as
is graphically shown in Figs. 28 and 29. The umbilical arteries he on either side
of the urachus, pass downward on each side of the bladder, and are connected with
the anterior division of the internal iliac arteries. After birth the distal portions
of their lumina become narrower, and the vessels finally appear as the obliterated
hypogastric arteries. Their last pervious branches are the superior vesical arteries.

Fig. 30. Theee Diagrams of the Umbilical Ring and its Significance in the Development of Ventral Hernia.
I. Dissection of the umbilical ring in a human embryo eight months old, viewed from within. The peritoneum and subperitoneal connective tissue, containing a small amount of fat, have been carefully removed, exposing a funnelshaped opening above and to the right of the umbilical arteries. The umbilical vein lies to the left of this weak spot. The umbilical arteries are the strongest structures in the wall of the ring, and a hernial protrusion usually occurs above or to one side of them. Occasionally the umbilical vein is situated to the right of the ring, in which case the weak spot would be on the left side.
II. Side-view of the umbilical ring, showing the favorite position of the small hernial protrusion often seen in newborn babes.
III. A larger hernia, representing a later stage of the same type. Note how the umbilicus becomes lodged at the lower portion of the hernial pouch.
It was along the umbilical vein and the umbilical arteries that infections of the new-born were so prone to occur in preaseptic days. (See Chapter III.)
The inner appearance of the umbilicus at birth is shown in Fig. 32. Shortly after birth the umbilical vein and the umbilical arteries become impervious (Fig.
61). In the adult the thickened outer edge of the suspensory ligament of the liver
represents what remains of the umbilical vein; below the umbilicus are three cords
which are usually solid, the central one passing to the summit, the others to the
right and left of the bladder. These three cords are the remnants of the urachus
and of the umbilical arteries.

Fig. 31. The Appearance of the Yolk-sac (Umbilical Vesicle) in a Pregnancy, with the Embryo 5.5 cm. Long. The chorion has been split and turned back on the uterine wall. The amniotic cavity is still intact, appearing as a tensely filled oval cyst containing the embryo. Coming from the placental attachment of the umbilical cord is a delicate vaseular thread which passes to the flattened, yellowish, opaque yolk-sac, now referred to as the umbilical vesicle. It remains approximately this size until birth. (See Fig. 32.)
The Umbilical Cord
In the very early embryo, as shown in Figs. 1 and 2, there is no umbilical cord as such, but it is represented by its chief constituent, the body-stalk.
By the time the embryo reaches 2.5 mm in length there has come into existence what might be termed the primitive cord (Fig. 3). This is composed of the omphalomesenteric duct and the body-stalk, both of which pass into the ventral surface
of the embryo. The omphalomesenteric duct occupies the upper or fragile part of the cord, and is surrounded by exocoelom. The lower and firmer part of the cord contains the umbilical arteries, the umbilical vein, and the allantois.
When the embryo reaches 3.5 mm in length (Fig. 4), the amnion has completely encircled the embryo. Outside the amniotic sac the omphalomesenteric duct and body-stalk are separate, but within the sac they have become more or less fused, forming the umbilical cord.
In the embryo 5 mm long this fusion of the cord is clearly seen (Fig. 5). The
outer walls of the cord show some degree of organization. In the upper part of the
cord is the exoccelomic cavity, communicating with the intra-abdominal portion,
and containing the omphalomesenteric duct and its vessels. In the lower part of
the cord are the component parts of the body-stalk, the umbilical vein, the two
umbilical arteries, and the allantois.

Fig. 32. The Umbilical Region, the Cord, and the Placenta at Term. (About half natural size.) The greater part of the cord has been omitted as irrelevant. The yolk-sac still persists as the umbilical vesicle, between the amnion and the chorion. Its duct, however, after traveling a short distance, becomes lost in the cord.
A similar picture is shown in the embryo 7 mm. long (Figs. 6 and 7). In
the former picture it will be noted that the exoccelomic cavity, that is, the portion
in the cord, has increased in size, and that it contains, in addition to the omphalomesenteric duct, a small portion of the bowel. The umbilical arteries lie in the lower
portion of the cord, and between them, and at a slightly lower level, is the allantois.
The umbilical vein usually lies to the left of the arteries (to the right in the
picture) .
When the embryo is 10 mm. in length (Fig. 8) , the vein lies in the upper wall of the cord. The exoccelomic cavity contains the omphalomesenteric duct, to which a loop of small bowel is attached; and situated in the lower part of the cord are the umbilical arteries and the allantois. The outer part of the cord, even at this early date, shows a tendency to become twisted.
Examination of the cord in an embryo 12.5 mm. long (Fig. 9) shows an exoccelomic cavity varying considerably in diameter. This cavity near the body contains small intestine and the omphalomesenteric artery and vein, but a little farther out only the omphalomesenteric duct and its vessels. The remaining portion of the cord contains the umbilical arteries, the umbilical vein, and the allantois. The allantois at some points is a flaccid tube, but at other points shows sac-like dilatations. It finally tapers off and ends in a point.
In the embryo 18 mm long (Fig. 10) the cord near the umbilicus is distinctly
enlarged. This enlargement is due to a marked dilatation of the exoccelomic cavity, which contains almost all the bowel, including the cecum and the omphalomesenteric vessels. A section farther out in the cord shows a small prolongation of
the exoccelom, containing the omphalomesenteric vessels and cross-sections of the
umbilical arteries, the umbilical vein, and the allantois.
A longitudinal section of the cord in an embryo 23 mm long presents an
interesting picture (Fig. 11). Near the embryo the upper wall of the cord contains
small, cyst-like spaces, which represent areas undergoing organization. The exoccelomic cavity is large, and contains nearly all the small bowel. Passing out between the coils of small intestine are the omphalomesenteric artery and vein,
which are continued far out into the solid portion of the cord. In the lower wall of
the cord are the umbilical arteries, the umbilical vein, and the allantois, which at
some points is solid and at other points can be recognized as spindle-like dilatations.
At this stage the cord shows marked twisting in its outer portion, and a cross-section
here shows the umbilical arteries and vein, with remnants of the omphalomesenteric
vessels and of the allantois.
The umbilical cord of an embryo 30 mm. long (Fig. 12) shows an even greater
enlargement near the embryo. This is due to the passive increase in size of the
exoccelomic cavity, which now contains many loops of small bowel. Passing out
between these loops are the omphalomesenteric vessels, which traverse the exoccelomic cavity, and continue their course outward in a narrow chink of the exoccelom. The solid portion of the cord is small in comparison with the exoccelomic cavity. It contains the umbilical arteries and vein, as well as the allantois.
By the time the embryo reaches 45 mm. in length (Figs. 13 and 14) the intestine
has usually receded into the abdomen. The exoccelomic cavity is very small, and
contains only the omphalomesenteric vessels. A cross-section of the cord near the
umbilicus now contains, in addition to the umbilical arteries and vein, a small
chink of exoccelom with the omphalomesenteric vessels in its interior, and the allantois. The allantois varies much in diameter: in some places it is a solid cord; at
other points it shows spindle-like dilatations (Fig. 13). A cross-section of an embryo 5.2 cm. in length presents a precisely similar picture. In Fig. 15 a crosssection of the omphalomesenteric vein is seen adherent to a small exoccelomic
space.
From this time until birth the cord shows only a few minor variations. The
relation of the vein to the arteries naturally varies according to the amount of
twisting of the cord, but the relation of the allantois to the arteries is constant. It
lies between and slightly below the arteries.
- Cross-section of the cord

Fig. 16 gives a cross-section of the cord in an embryo 6.5 cm long.
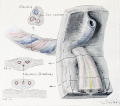
Fig. 17 gives a cross-section of the cord in an embryo 7.5 cm long.

Fig. 18 gives a cross-section of the cord in an embryo 9.0 cm long.
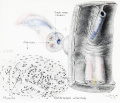
Fig. 19 gives a cross-section of the cord in an embryo 10.0 cm long.
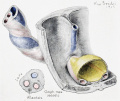
Fig. 20 gives a cross-section of the cord in an embryo 12.0 cm long.
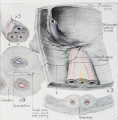
Fig. 21 gives a cross-section of the cord in an embryo 12.0 cm long.

Fig. 22 gives a cross-section of the cord in an embryo 12.0 cm long.

Fig. 23 gives a cross-section of the cord in an embryo 12.0 cm long.
- Cullen1916 fig24.jpg
Fig. 24 gives a cross-section of the cord in an embryo 15.0 cm long.
In embryos 12 cm in length the patent allantois may be detected in the cord at a considerable distance from the fetus (Fig. 22).
Remnants of the omphalomesenteric duct in the cord, as seen in Fig. 21, are very rare.
The Omphalomesenteric Duct
In the very early embryo the yolk-sac is intimately attached to its ventral surface (Fig. 1), and in a short time extends into the embryo, forming the fore-gut and the hind-gut (Fig. 2). The amnion rapidly encompasses the embryo, and pushes the yolk-sac away. Inasmuch as part of the yolk-sac already forms the digestive tract, it is firmly anchored to the embryo. The rest of the yolk-sac still retains its connection with the digestive tract by a drawn-out and narrow portion, which is called the omphalomesenteric or vitelline duct (Fig. 3). The yolk-sac proper, the omphalomesenteric duct, and the primitive digestive tract, at this stage, form various portions of one and the same cavity. The omphalomesenteric duct can be recognized in the embryo 2.5 mm. long. It will be noted in Fig. 3 that the omphalomesenteric du-ct is surrounded on all sides by exocoelom; in other words, it lies in the exocoelomic cavity.
In an embryo 5 mm in length (Fig. 5) the first loop of small bowel is seen, and
passing off from its convexity is the omphalomesenteric or vitelline duct. This
duct, accompanied by the omphalomesenteric artery and vein, passes outward in
the exoccelomic cavity of the cord, and emerging from the amniotic sac reaches
the yolk-sac.
When the embryo reaches 7 mm in length (Fig. 6) a loop of small bowel can be
seen in the exoccelomic cavity of the cord, and projecting from its convex surface
the patent omphalomesenteric duct. Accompanying the duct are the omphalomesenteric artery and vein.
In another embryo of the same length (Fig. 7) we note that the duct has already
lost its connection with the small bowel. Beyond this point, however, it is patent
and appears as a bulbous dilatation in the cord a short distance from the embryo.
Hence it is evident that variations may exist and that the duct may or may not still
be connected with the small bowel when the embryo is 7 mm long.
A study of Fig. 8, from an embryo 10 mm in length, shows that the first loop of
small bowel extends far outward in the exoccelomic cavity of the cord. It is
accompanied by the omphalomesenteric vessels, which are continued out into the
cord for the entire length, terminating in the yolk-sac. The duct accompanies the
vessels as far as the yolk-sac.
In Fig. 9, from an embryo 12.5 mm long, the omphalomesenteric duct is patent
in the exoccelom, and apparently still communicates with the small bowel. The duct is lined with one layer of low cuboid epithelium. The patent portion can be
traced outward in the cord; it forms a bulbous dilatation near the yolk-sac, into
which it opens. The yolk-sac also is lined with one layer of cuboid epithelium.
In the embryo of 18 mm (Fig. 10) all trace of the omphalomesenteric duct is
lost, but its vessels are still found in the cord. They lie in a funnel-shaped prolongation of the exoccelom. These vessels can be easily followed in Figs. 11, 12, 13, 14, and 20. Generally speaking, the omphalomesenteric duct usually disappears
when the embryo is between 4 and 12 mm. in length, but its vessels persist long after the duct has disappeared.

Fig. 33. A Diagrammatic Representation of the Umbilical Region of a Fetus at Term. An exceptional feature of the picture is the persistence of the omphalomesenteric structures in the form of a welldefined vascular Meckel's diverticulum. Note the relationship between the omphalomesenteric vessels, the superior mesenteric artery, and the portal vein. In the cord the vitelline vessels still persist in the organized exoccelom. At birth all trace of the omphalomesenteric structure has usually disappeared, but the allantoic cord often persists, and is seen between and below the umbilical arteries. It is continuous with the urachus, which may have a number of spindleshaped dilatations down to the bladder. These may or may not have lumina.
In the earliest stages the omphalomesenteric arteries are two in number; they pass out on each side of the yolk-sac. They arise from a plexus of from two to four smaller vessels directly from the aorta. The left artery disappears, the right persists, follows the omphalomesenteric duct, and terminates in a network over the entire yolk-sac (Figs. 2, 4, and 5). The proximal portion of the omphalomesenteric artery later becomes converted into the superior mesenteric artery.
In the beginning the omphalomesenteric veins are two in number. The right disappears; the left collects the blood from the entire yolk-sac and from the omphalomesenteric duct, and in the liver anastomoses with the left umbilical vein. Before entering the liver it receives tributaries from the intestine (vena mesenterica superior, Fig. 7). It later forms the portal vein.
In Fig. 14, from an embryo 4.5 cm. long, the omphalomesenteric duct still persists as a cord passing from the intestine to the abdominal wall. It consists of embryonic connective tissue and has an epithelial center, but no lumen.
Fig. 23 is a cross-section of the umbilical cord near the abdominal wall of an embryo 12 cm. long. The omphalomesenteric duct is recognized as a solid epithelial cord. Its blood-vessels are still patent.
Although the duct usually disappears early in the embryologic development, it is occasionally found patent at birth. In other cases only a portion of the duct remains. When the duct remains patent, an umbilical fecal fistula develops as soon as the cord comes away. If the inner end be patent, we have a Meckel's diverticulum (Fig. 26). This may or may not be adherent to the umbilicus (Fig. 25). In rare instances the duct is obliterated both at the intestine and at the umbilicus, but the median portion persists. In such a case we have an intestinal cyst. In a few cases remnants of the duct haye been detected in the umbilical region between the peritoneum and the abdominal walL One of the most frequent sites for remains of the duct is at the point of attachment of the umbilical cord. In such cases, when the cord comes away, a small, raspberry-like mass will be noted at the
navel. Occasionally the omphalomesenteric vessels may still persist as impervious fibrous cords (Fig. 21). These have in some instances given rise to intestinal obstruction. All these conditions which produce definite clinical entities will be discussed fully in subsequent chapters.
- ↑ The illustrations in this chapter are arranged chiefly according to the age of the embryo from which they were obtained.
Literature
Literature Consulted On Embryology Of The Umbilical Region.
Ahlfeld, Fr. : Die Allantois des Menschen und ihr Verhaltnis zur Nabelschnur. Arch, f . Gynak., 1876, x, 81.
Cazin, Henry: Etude anatomique et pathologique sur les diverticules de l'intestin. These de Paris, 1862, No. 138.
Freer, James A.: Abnormalities of the Urachus. Ann. of Surg., 1887, v, 107.
Ledderhose, G.: Chirurgische Erkrankungen des Nabels. Deutsche Chirurgie, 1890, Lief. 45 b.
Lowy, H: Die Riickbildung der Allantois beim Menschen. Arch, fiir Anat. und Physiologie, Anat, Abth., 1905, 159-176.
Meyer, Arthur: On the Structure of the Human Umbilical Vesicle. Amer. Jour. Anat., 1904, iii, 155.
Monod, J.: Des fistules urinaires ombilicales dues a la persistance de l'ouraque. These de Paris, 1899, No. 62.
Vaughan, George T.: Patent Urachus. Review of the cases reported. Operation on a case complicated with stones in the kidneys. A note on tumors and cysts of the urachus. Trans. Amer. Surg. Assoc, 1905, xxiii, 273.
Mall, Franklin P.: Jour. Morphology, 1891, v, 459-477.
Reference
Cullen TS. Embryology, anatomy, and diseases of the umbilicus together with diseases of the urachus. (1916) W. B. Saunders Company, Philadelphia And London.
| Historic Disclaimer - information about historic embryology pages |
|---|
|
Cite this page: Hill, M.A. (2026, April 17) Embryology Book - Umbilicus (1916) 1. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Book_-_Umbilicus_(1916)_1
- © Dr Mark Hill 2026, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G