BGDB Gastrointestinal - Fetal: Difference between revisions
mNo edit summary |
|||
| (29 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{BGDB GIT}} | {{BGDB GIT}} | ||
==Fetal Development== | ==Fetal Development== | ||
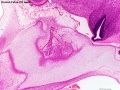
[[File: | [[File:Fetal head section 01.jpg|thumb|Fetal oral cavity (week 12)]] | ||
The Embryonic period involved transient structures to establish body and placental tissues, folding and form. The long human Fetal period (4x the embryonic period) is a time of extensive growth in size and mass as well as ongoing differentiation of organ systems established in the embryonic period. (More? See [[Fetal Development|Fetal Notes]]) | The Embryonic period involved transient structures to establish body and placental tissues, folding and form. The long human Fetal period (4x the embryonic period) is a time of extensive growth in size and mass as well as ongoing differentiation of organ systems established in the embryonic period. (More? See [[Fetal Development|Fetal Notes]]) | ||
| Line 11: | Line 11: | ||
==Early Fetus== | ==Early Fetus== | ||
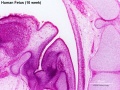
[[File: | [[File:Human week 10 fetus 01.jpg|800px]] | ||
<gallery> | |||
File:Human week 10 fetus 04.jpg|Oral cavity | |||
File:Human week 10 fetus 12.jpg|Olfactory | |||
File:Human week 10 fetus 10.jpg|Pituitary | |||
File:Human week 10 fetus 08.jpg|Epiglottis | |||
File:Human_week_10_fetus_07.jpg|Spleen | |||
File:Human_week_10_fetus_06.jpg|Midgut herniation | |||
File:Human_week_10_fetus_26.jpg|Midgut herniation (label) | |||
File:Human week 10 fetus 03.jpg|Pelvic region | |||
File:Human week 10 fetus 23.jpg|Pelvic region (label) | |||
</gallery> | |||
{{ | [[File:Human week 10 fetus 23.jpg|thumb|Pelvic region (week 10)]] | ||
Begin by just looking at the fetal anatomy in sections taken through the above female fetus 10 week ({{GA}} week 12), approximately CRL 40 mm in size) and see how this compares with what you already know of adult GIT anatomy. | |||
<br> | |||
{{10wkFetus}} | |||
There are 4 sections taken in the parasagittal and sagittal plane (moving from the right at Plane A towards the midline at Plane D). Click on the small images (or the text below) to open the linked large image pages. | There are 4 sections taken in the parasagittal and sagittal plane (moving from the right at Plane A towards the midline at Plane D). Click on the small images (or the text below) to open the linked large image pages. | ||
==Midgut Herniation== | ==Midgut Herniation== | ||
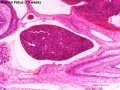
[[File:Human week 10 fetus 26.jpg|thumb|Week 10]] | |||
[[File:Human- fetal week 10 sagittal plane D.jpg|thumb|Week 10]] | [[File:Human- fetal week 10 sagittal plane D.jpg|thumb|Week 10]] | ||
In the week 10 fetus (right) the midgut is still herniated (lying outside the ventral body wall) at the umbilicus. We saw in earlier pages that this heriation began back in the embryonic period (week 5) and the initial loop undergoes a series of rotations through embryonic and early fetal periods which position the midgut in its correct adult anatomical locations. These rotations are around the superior mesenteric artery (which supplies this region) and the associated mesentry. (Note this rotation is complicated and explained differently in different texts) | In the week 10 fetus (right) the midgut is still herniated (lying outside the ventral body wall) at the umbilicus. We saw in earlier pages that this heriation began back in the embryonic period (week 5) and the initial loop undergoes a series of rotations through embryonic and early fetal periods which position the midgut in its correct adult anatomical locations. These rotations are around the superior mesenteric artery (which supplies this region) and the associated mesentry. (Note this rotation is complicated and explained differently in different texts) | ||
| Line 28: | Line 42: | ||
[[File:Bailey299_300.jpg|300px]] [[File:Bailey304.jpg|300px]] | [[File:Bailey299_300.jpg|300px]] [[File:Bailey304.jpg|300px]] | ||
[[File:Normal intestinal rotation cartoon.jpg|500px]] | [[File:Normal intestinal rotation cartoon.jpg|500px]] | ||
Normal intestinal rotation (note these are gestational age weeks) | Normal intestinal rotation (note these are {{GA}} gestational age weeks).{{#pmid:20549505|PMID20549505}} | ||
==Stomach Mesentery== | ==Stomach Mesentery== | ||
| Line 52: | Line 54: | ||
In the second trimester, the ventral and dorsal mesenteries associated with the stomach are still anatomically different from the newborn. The figure shows a lateral view of this process comparing the early second trimester arrangement with the newborn structure. | In the second trimester, the ventral and dorsal mesenteries associated with the stomach are still anatomically different from the newborn. The figure shows a lateral view of this process comparing the early second trimester arrangement with the newborn structure. | ||
Ventral Mesogastrium | '''Ventral Mesogastrium''' | ||
Attached to the superior end of the stomach will form the lesser omentum. This structure will connect the lesser curvature of the stomach to the liver as a ligamentous structure. | Attached to the superior end of the stomach will form the lesser omentum. This structure will connect the lesser curvature of the stomach to the liver as a ligamentous structure. | ||
Dorsal Mesogastrium | '''Dorsal Mesogastrium''' | ||
Attached to the inferior end of the stomach initially as an extended fold, this later fuses as a single "apron-like" structure, the greater omentum. Fusion will also incorporate the transverse colon part of the large intestine. | Attached to the inferior end of the stomach initially as an extended fold, this later fuses as a single "apron-like" structure, the greater omentum. Fusion will also incorporate the transverse colon part of the large intestine. | ||
| Line 80: | Line 82: | ||
[[File:Small intestine villi and crypts.jpg|thumb|Small intestine villi and crypts]] | [[File:Small intestine villi and crypts.jpg|thumb|Small intestine villi and crypts]] | ||
[[File:Peyer%27s_patch_01.jpg|thumb|Adult Peyer's patch]] | [[File:Peyer%27s_patch_01.jpg|thumb|Adult Peyer's patch]] | ||
[[File:Fetal_liver_weight_growth_graph.jpg|thumb| Liver weight 1 to 124 grams (birth)]] | |||
'''Week 11''' - villi begin to appear in small intestine, goblet cells present | '''Week 11''' - villi begin to appear in small intestine, goblet cells present | ||
| Line 99: | Line 102: | ||
* mesenteric lymph nodes | * mesenteric lymph nodes | ||
===Intestinal Length Growth=== | |||
[[File:Fetal small Intestine length growth graph.jpg|500px]] | |||
Small Intestine length (mm) | |||
==Amniotic Fluid | ==Amniotic Fluid== | ||
[[File:Amniocentesis.jpg|thumb|[[Amniocentesis]]is a prenatal diagnostic test, carried out by removing a small fluid sample.]] | |||
# required for lung development. | # required for lung development. | ||
# enables movement and symmetrical musculoskeletal development. | # enables movement and symmetrical musculoskeletal development. | ||
| Line 124: | Line 121: | ||
* circulated by fetal inhaling and swallowing. | * circulated by fetal inhaling and swallowing. | ||
* replacing by fetal exhalation and urination. | * replacing by fetal exhalation and urination. | ||
* low magnesium levels associated with preeclampsia and diabetes. | |||
===Amniotic Fluid Swallowing=== | |||
In early embryonic development both the buccopharyngeal and cloacal membranes degenerated, allowing the GIT to be filled with amniotic fluid. Towards the end of the fetal period the fetus is now swallowing approximately 500 ml of amniotic fluid / day. | |||
== | <html5media width="480" height="360">https://www.youtube.com/embed/r9D7aiFG7N8</html5media> | ||
This swallowed amniotic fluid moves through the GIT from esophagus, to stomach, to small intestine, stopping at the large bowel. In the large bowel the majority of fluid (water) is absorbed, along with electrolytes, glucose, urea and hormones. This process may contribute to fetal nutrition and prepare the GIT for its postnatal function. The process of swallowing amniotic fluid has been suggested to also help regulate fluid volume. | This swallowed amniotic fluid moves through the GIT from esophagus, to stomach, to small intestine, stopping at the large bowel. In the large bowel the majority of fluid (water) is absorbed, along with electrolytes, glucose, urea and hormones. This process may contribute to fetal nutrition and prepare the GIT for its postnatal function. The process of swallowing amniotic fluid has been suggested to also help regulate fluid volume. | ||
{| | |||
| | |||
! Polyhydramnios | |||
|- | |||
| width=405px|[[File:Fetal polyhydramnios MRI-01.jpg|400px]] | |||
|valign=top|Polyhydramnios (hydramnios, amniotic fluid disorder) refers to abnormally high amniotic fluid levels. | |||
<br> | |||
{{PolyhydramniosTable}} | |||
== | |} | ||
==Fetal Meconium== | |||
* Mixture of substances (debris, glandular secretions, fatty material and bile pigments) that accumulate in the large bowel (green fecal material). | |||
* Will form the '''neonatal meconium''' which is the first (usually within 24h to 48h) postnatal excretion from the GIT. | |||
** If no discharge (bowel motion) is observed in this early period it can be indicative of an abnormality of the GIT. | |||
===Meconium Aspiration=== | |||
* Aspiration can occur near term or at delivery, if meconiumis discharged into the amiotic fluid (meconium stained amniotic fluid) and then injested by the fetus as it swallows amiotic fluid. | |||
* Can then lead to '''meconium aspiration syndrome''' (MAS), meconium is drawn into the fetal/newborn lungs, causing inflammation, cell death and potentially perinatal death. | |||
* Meconium can also damage the placenta and associated blood vessels. | |||
''' | {{GIT terms}} | ||
==Additional Information== | |||
{{Med Prac additional Information}} | |||
===Stem Cells=== | |||
{| | |||
| Stem cells in the adult epithelium of the intestine (and stomach) divide continuously throughout life to replace the 4 cell types within the epithelium: | |||
# '''Brush-border cells''' - these absorptive cells in intestine microvilli increase the active surface area. | |||
# '''Goblet cells''' - secreting mucus to protect the epithelium and to aid movement. | |||
# '''Paneth cells''' - innate immune system and secrete cryptdins that kill bacteria. | |||
# '''Enteroendocrine cells''' - (15+ subtypes) secrete serotonin and other peptide hormones acting on neurons and other cells to regulate many different functions. | |||
| [[File:Intestine histology 004.jpg|200px]] | |||
|} | |||
<references/> | |||
| Line 147: | Line 174: | ||
{{ | {{BGDBFooter}} | ||
Latest revision as of 15:28, 28 April 2018
Fetal Development

The Embryonic period involved transient structures to establish body and placental tissues, folding and form. The long human Fetal period (4x the embryonic period) is a time of extensive growth in size and mass as well as ongoing differentiation of organ systems established in the embryonic period. (More? See Fetal Notes)
As many students are new to embryology the majority of the practical class time has been spent introducing general concepts of early human development and combining this with the early formation of GIT structures. While the fetal period is substantially longer, there will be much less content to be covered.
Fetal developmental features include: the growth and rotation of intestines initially herniated outside the ventral body wall; changes in mesenteries; development of the blood supply and tract wall.
Finally consider the initial functions of the tract with amionic fluid swallowing and the accumulation of both secretions and swallowed components within the large intestine as meconium.
Early Fetus


Oral cavity
Olfactory

Pituitary
Epiglottis
Spleen

Midgut herniation

Midgut herniation (label)

Pelvic region

Pelvic region (label)









Begin by just looking at the fetal anatomy in sections taken through the above female fetus 10 week (GA week 12), approximately CRL 40 mm in size) and see how this compares with what you already know of adult GIT anatomy.
Related Images
Fetus (week 10) Planes A (most lateral), B (lateral), C (medial) and D (midline) from lateral towards the midline.
- Human Fetus - most lateral | lateral | medial | midline
- Head - most lateral | lateral | medial | midline
- Cerebellum - most lateral | lateral | medial | midline
- Urogenital Unlabelled - most lateral | lateral | medial | midline
- Urogenital Labelled - most lateral | lateral | medial | midline
- Large Images - midline
- Image Source: UNSW Embryology, no reproduction without permission.
There are 4 sections taken in the parasagittal and sagittal plane (moving from the right at Plane A towards the midline at Plane D). Click on the small images (or the text below) to open the linked large image pages.
Midgut Herniation

In the week 10 fetus (right) the midgut is still herniated (lying outside the ventral body wall) at the umbilicus. We saw in earlier pages that this heriation began back in the embryonic period (week 5) and the initial loop undergoes a series of rotations through embryonic and early fetal periods which position the midgut in its correct adult anatomical locations. These rotations are around the superior mesenteric artery (which supplies this region) and the associated mesentry. (Note this rotation is complicated and explained differently in different texts)
One week later (week 11) continued fetal body wall growth (and other factors) returns the midgut herniation returns to the abdominal cavity.
Small intestine growth in length is initially linear (first half pregnancy to 32 cm CRL), followed by rapid growth in the last 15 weeks doubling the overall length to term. Growth continues postnatally but after 1 year slows again to a linear increase to adulthood. (More? Intestine Development)



Normal intestinal rotation (note these are GA gestational age weeks).[1]
Stomach Mesentery

|
In the second trimester, the ventral and dorsal mesenteries associated with the stomach are still anatomically different from the newborn. The figure shows a lateral view of this process comparing the early second trimester arrangement with the newborn structure. Ventral Mesogastrium Attached to the superior end of the stomach will form the lesser omentum. This structure will connect the lesser curvature of the stomach to the liver as a ligamentous structure. Dorsal Mesogastrium Attached to the inferior end of the stomach initially as an extended fold, this later fuses as a single "apron-like" structure, the greater omentum. Fusion will also incorporate the transverse colon part of the large intestine. This will also contribute the gastrosplenic ligament (gastrolienal ligament). |
Blood Supply
|
|
Each region of the gastrointestinal tract has a specific arterial supply which historically defined the 3 gastrointestinal tract regions (foregut, midgut and hindgut).
|

Fetal Tract Development



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Week 11 - villi begin to appear in small intestine, goblet cells present
Week 16 - villi apparent in entire intestine
Adult small intestine will be divided into 3 regions with the same basic histological organization.
- duodenum (25-30 cm)
- jejunum (about first two-fifths of the rest)
- ileum
Week 20 - Peyer's patches appear in small intestine
The adult intestinal immune system includes:
- Peyer's patches
- isolated lymphoid follicles
- cryptopatches - small clusters of lymphoid cells with an immature lymphocyte phenotype and dendritic cells.
- mesenteric lymph nodes
Intestinal Length Growth

Small Intestine length (mm)
Amniotic Fluid

- required for lung development.
- enables movement and symmetrical musculoskeletal development.
- maintains relatively constant temperature.
- protects by cushioning sudden blows or movements.
Volume - increases as the fetus grows.
- 34 weeks (GA) - peaks at about 800 mL.
- 40 weeks (GA) - about 600 mL at term.
- circulated by fetal inhaling and swallowing.
- replacing by fetal exhalation and urination.
- low magnesium levels associated with preeclampsia and diabetes.
Amniotic Fluid Swallowing
In early embryonic development both the buccopharyngeal and cloacal membranes degenerated, allowing the GIT to be filled with amniotic fluid. Towards the end of the fetal period the fetus is now swallowing approximately 500 ml of amniotic fluid / day.
<html5media width="480" height="360">https://www.youtube.com/embed/r9D7aiFG7N8</html5media>
This swallowed amniotic fluid moves through the GIT from esophagus, to stomach, to small intestine, stopping at the large bowel. In the large bowel the majority of fluid (water) is absorbed, along with electrolytes, glucose, urea and hormones. This process may contribute to fetal nutrition and prepare the GIT for its postnatal function. The process of swallowing amniotic fluid has been suggested to also help regulate fluid volume.
| Polyhydramnios | |||||||||
|---|---|---|---|---|---|---|---|---|---|

|
Polyhydramnios (hydramnios, amniotic fluid disorder) refers to abnormally high amniotic fluid levels.
| ||||||||
Fetal Meconium
- Mixture of substances (debris, glandular secretions, fatty material and bile pigments) that accumulate in the large bowel (green fecal material).
- Will form the neonatal meconium which is the first (usually within 24h to 48h) postnatal excretion from the GIT.
- If no discharge (bowel motion) is observed in this early period it can be indicative of an abnormality of the GIT.
Meconium Aspiration
- Aspiration can occur near term or at delivery, if meconiumis discharged into the amiotic fluid (meconium stained amniotic fluid) and then injested by the fetus as it swallows amiotic fluid.
- Can then lead to meconium aspiration syndrome (MAS), meconium is drawn into the fetal/newborn lungs, causing inflammation, cell death and potentially perinatal death.
- Meconium can also damage the placenta and associated blood vessels.
| Gastrointestinal Tract Terms | ||
|---|---|---|
| ||
|
Additional Information
| Additional Information - Content shown under this heading is not part of the material covered in this class. It is provided for those students who would like to know about some concepts or current research in topics related to the current class page. |
Stem Cells
Stem cells in the adult epithelium of the intestine (and stomach) divide continuously throughout life to replace the 4 cell types within the epithelium:
|

|
BGDB: Lecture - Gastrointestinal System | Practical - Gastrointestinal System | Lecture - Face and Ear | Practical - Face and Ear | Lecture - Endocrine | Lecture - Sexual Differentiation | Practical - Sexual Differentiation | Tutorial
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, June 10) Embryology BGDB Gastrointestinal - Fetal. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/BGDB_Gastrointestinal_-_Fetal
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G