Talk:Abnormal Development - Cytomegalovirus
| About Discussion Pages |
|---|

Glossary Links
Cite this page: Hill, M.A. (2024, April 23) Embryology Abnormal Development - Cytomegalovirus. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Talk:Abnormal_Development_-_Cytomegalovirus |
2019
2018
Sequelae of congenital cytomegalovirus (cCMV) following maternal primary infection are limited to those acquired in the first trimester of pregnancy
Clin Infect Dis. 2018 Dec 31. doi: 10.1093/cid/ciy1128. [Epub ahead of print]
Faure-Bardon V1,2, Magny JF1,3, Parodi M4, Couderc S5, Garcia P6, Maillotte AM7, Benard M8, Pinquier D9, Astruc D10, Patural H11, Pladys P12, Parat S13, Guillois B14,15, Garenne A16, Bussières L1,17, Guilleminot T1,18, Stirnemann J1,2, Ghout I19,20, Ville Y1,2, Leruez-Ville M1,18.
Abstract
BACKGROUND: Relationship between gestational age at maternal primary infection and outcome in cCMV was based on small retrospective studies between 1980 and 2011. They reported sequelae in 32% and 15% following maternal primary infection in first and second or third trimester respectively. We aimed to revisit this relationship prospectively between 2011 and 2017 using accurate virological tools.
METHODS: Women with primary infection and an infected child aged at least 1 year at the time of analysis. Accurate determination of the timing of primary infection was based upon serial measurement of IgM, IgG and IgG-avidity in sera collected at each trimester. Outcome was assessed according to a structured follow-up between birth and 48 months.
RESULTS: 255 women and their 260 fetuses/neonates were included. Dating maternal infection was prospective in 86% of cases and retrospective in 14%. At a median follow-up of 24 months, the proportion of SNHL and/or neurologic sequelae were 32.4% (95%IC 23.72, 42.09) after maternal primary infection in first trimester, and 0 (0, 6.49) and 0 (0, 11.95) after infection in second and third trimester respectively (p<.0001).
CONCLUSION: These results suggest that CMV infection can be severe only when the virus hits the fetus in the embryonic or early fetal period. Recent guidelines recommend auditory follow-up for at least 5 years of all infected children. This raises parental anxiety and generates significant cost. We suggest that auditory and specialized neurologic follow-up may be recommended only to children infected from maternal infection in the first trimester.
PMID: 30596974 DOI: 10.1093/cid/ciy1128
Neuroimaging Profiles and Neurodevelopmental Outcome in Infants With Congenital Cytomegalovirus Infection
Giannattasio A, Bruzzese D, Di Costanzo P, Capone E, Romano A, D'Amico A, Bravaccio C, Grande C, Capasso L & Raimondi F. (2018). Neuroimaging Profiles and Neurodevelopmental Outcome in Infants With Congenital Cytomegalovirus Infection. Pediatr. Infect. Dis. J. , 37, 1028-1033. PMID: 30222696 DOI.
Giannattasio A1, Bruzzese D2, Di Costanzo P1, Capone E1, Romano A1, D'Amico A3, Bravaccio C1, Grande C1, Capasso L1, Raimondi F1. Author information Abstract BACKGROUND: The accurate stratification of infants with congenital cytomegalovirus (CMV) infection at risk for more severe outcome may help in the management of patients. Aim of this study was to investigate the ability of a comprehensive neuroimaging investigation in predicting the long-term neurodevelopmental outcome in patients with congenital CMV. We analyzed the prognostic accuracy of a traditional score and a recently proposed scale applied to head ultrasound (HUS), computed tomography (CT) and magnetic resonance imaging (MRI). METHODS: All consecutive neonates born from 2002 to 2015 with congenital CMV infection were considered eligible for the study. Neuroimaging findings were scored according to both scores. RESULTS: One hundred seventy infants were included (112 symptomatic patients). One-hundred eighteen infants received both HUS, CT and MRI. CT and MRI were normal in all 56 asymptomatic patients, while 32% of them presented an abnormal HUS. The prevalence of abnormal findings differed according to the neuroimaging study. The sensitivity of the new neuroimaging score in detecting patients at risk for poor neurologic outcome was higher than the traditional one for all neuroimaging examinations. CT and MRI showed higher positive predictive value compared with HUS. No neuroimaging examination showed a negative predictive value equal to 100%. CONCLUSIONS: Although HUS is the safest neuroimaging technique, it performs less well in detecting some brain abnormalities that can be associated with a poor neurodevelopmental outcome. A comprehensive neuroimaging evaluation is mandatory in infants with congenital CMV infection to decide for treatment and make a prognostic evaluation.
PMID: 30081449 PMCID: PMC6116058 DOI: 10.3390/v10080405
Maternal Immunity and the Natural History of Congenital Human Cytomegalovirus Infection
Britt WJ. (2018). Maternal Immunity and the Natural History of Congenital Human Cytomegalovirus Infection. Viruses , 10, . PMID: 30081449 DOI.
Britt WJ1. Author information Abstract Congenital human cytomegalovirus (HCMV) is the most common viral infection of the developing fetus, and a significant cause of neurodevelopmental abnormalities in infants and children. Congenital HCMV infections account for an estimated 25% of all cases of hearing loss in the US. It has long been argued that maternal adaptive immune responses to HCMV can modify both the likelihood of intrauterine transmission of HCMV, and the severity of fetal infection and risk of long term sequelae in infected infants. Over the last two decades, multiple studies have challenged this paradigm, including findings that have demonstrated that the vast majority of infants with congenital HCMV infections in most populations are born to women with established immunity prior to conception. Furthermore, the incidence of clinically apparent congenital HCMV infection in infants born to immune and non-immune pregnant women appears to be similar. These findings from natural history studies have important implications for the design, development, and testing of prophylactic vaccines and biologics for this perinatal infection. This brief overview will provide a discussion of existing data from human natural history studies and animal models of congenital HCMV infections that have described the role of maternal immunity in the natural history of this perinatal infection. KEYWORDS: congenital cytomegalovirus infection; human cytomegalovirus; intrauterine infection; maternal antiviral immunity
Pathogenesis of developmental anomalies of the central nervous system induced by congenital cytomegalovirus infection
Kawasaki H, Kosugi I, Meguro S & Iwashita T. (2017). Pathogenesis of developmental anomalies of the central nervous system induced by congenital cytomegalovirus infection. Pathol. Int. , 67, 72-82. PMID: 28074532 DOI.
Kawasaki H1, Kosugi I1, Meguro S1, Iwashita T1. Author information Abstract In humans, the herpes virus family member cytomegalovirus (CMV) is the most prevalent mediator of intrauterine infection-induced congenital defect. Central nervous system (CNS) dysfunction is a distinguishing symptom of CMV infection, and characterized by ventriculoencephalitis and microglial nodular encephalitis. Reports on the initial distribution of CMV particles and its receptors on the blood brain barrier (BBB) are rare. Nevertheless, several factors are suggested to affect CMV etiology. Viral particle size is the primary factor in determining the pattern of CNS infections, followed by the expression of integrin β1 in endothelial cells, pericytes, meninges, choroid plexus, and neural stem progenitor cells (NSPCs), which are the primary targets of CMV infection. After initial infection, CMV disrupts BBB structural integrity to facilitate the spread of viral particles into parenchyma. Then, the initial meningitis and vasculitis eventually reaches NSPC-dense areas such as ventricular zone and subventricular zone, where viral infection inhibits NSPC proliferation and differentiation and results in neuronal cell loss. These cellular events clinically manifest as brain malformations such as a microcephaly. The purpose of this review is to clearly delineate the pathophysiological basis of congenital CNS anomalies caused by CMV. KEYWORDS: blood brain barrier; central nervous system; cytomegalovirus; integrin β1; neural stem cells PMID: 28074532 DOI: 10.1111/pin.12502
Maternal and fetal cytomegalovirus infection: diagnosis, management, and prevention
F1000Res. 2018 Mar 1;7:255. doi: 10.12688/f1000research.12517.1. eCollection 2018.
Pass RF1, Arav-Boger R2.
Abstract
Congenital cytomegalovirus infection is a major cause of central nervous system and sensory impairments that affect cognition, motor function, hearing, language development, vestibular function, and vision. Although the importance of congenital cytomegalovirus infection is readily evident, the vast majority of maternal and fetal infections are not identified, even in developed countries. Multiple studies of prenatal cytomegalovirus infections have produced a body of knowledge that can inform the clinical approach to suspected or proven maternal and fetal infection. Reliable diagnosis of cytomegalovirus infection during pregnancy and accurate diagnosis of fetal infection are a reality. Approaches to preventing the transmission of cytomegalovirus from mother to fetus and to the treatment of fetal infection are being studied. There is evidence that public health approaches based on hygiene can dramatically reduce the rate of primary maternal cytomegalovirus infections during pregnancy. This review will consider the epidemiology of congenital cytomegalovirus infection, the diagnosis and management of primary infection during pregnancy, and approaches to preventing maternal infection. KEYWORDS: CMV hyperimmune globulin; CMV prevention; Congenital infection; Cytomegalovirus; Fetal diagnosis; Fetal infection; Prenatal infection; Valacyclovir PMID: 29560263 PMCID: PMC5832908 DOI: 10.12688/f1000research.12517.1
2017
Natural killer cells attenuate cytomegalovirus-induced hearing loss in mice
PLoS Pathog. 2017 Aug 31;13(8):e1006599. doi: 10.1371/journal.ppat.1006599. eCollection 2017 Aug.
Almishaal AA1, Mathur PD2,3, Hillas E4, Chen L5, Zhang A5, Yang J2,3, Wang Y5, Yokoyama WM6,7, Firpo MA4, Park AH5.
Abstract
Congenital cytomegalovirus (CMV) infection is the most common non-hereditary cause of sensorineural hearing loss (SNHL) yet the mechanisms of hearing loss remain obscure. Natural Killer (NK) cells play a critical role in regulating murine CMV infection via NK cell recognition of the Ly49H cell surface receptor of the viral-encoded m157 ligand expressed at the infected cell surface. This Ly49H NK receptor/m157 ligand interaction has been found to mediate host resistance to CMV in the spleen, and lung, but is much less effective in the liver, so it is not known if this interaction is important in the context of SNHL. Using a murine model for CMV-induced labyrinthitis, we have demonstrated that the Ly49H/m157 interaction mediates host resistance in the temporal bone. BALB/c mice, which lack functional Ly49H, inoculated with mCMV at post-natal day 3 developed profound hearing loss and significant outer hair cell loss by 28 days of life. In contrast, C57BL/6 mice, competent for the Ly49H/m157 interaction, had minimal hearing loss and attenuated outer hair cell loss with the same mCMV dose. Administration of Ly49H blocking antibody or inoculation with a mCMV viral strain deleted for the m157 gene rendered the previously resistant C57BL/6 mouse strain susceptible to hearing loss to a similar extent as the BALB/c mouse strain indicating a direct role of the Ly49H/m157 interaction in mCMV-dependent hearing loss. Additionally, NK cell recruitment to sites of infection was evident in the temporal bone of inoculated susceptible mouse strains. These results demonstrate participation of NK cells in protection from CMV-induced labyrinthitis and SNHL in mice. PMID: 28859161 PMCID: PMC5597263 DOI: 10.1371/journal.ppat.1006599 [Indexed for MEDLINE] Free PMC Article
Fetal cytomegalovirus infection
Best Pract Res Clin Obstet Gynaecol. 2017 Jan;38:97-107. doi: 10.1016/j.bpobgyn.2016.10.005. Epub 2016 Oct 20.
Leruez-Ville M1, Ville Y2.
Author information
Abstract
Cytomegalovirus (CMV) congenital infection affects 0.7% of live births worldwide and is the leading cause of congenital neurological handicap of infectious origin. However, systematic screening for this infection has not been implemented in pregnancy or at birth in any country. This apparent paradox had been justified by persisting gaps in the knowledge of this congenital infection: uncertain epidemiological data, difficulty in the diagnosis of maternal infection, absence of validated prenatal prognostic markers, unavailability of an efficient vaccine and scarcity of data available on the treatment. However, in the last decade, new data have emerged towards better management of this congenital infection, including solid epidemiological data, good evidence for the accuracy of diagnosis of maternal CMV infection and good evidence for the feasibility of predicting the outcome of fetal infection by a combination of fetal imaging and fetal laboratory parameters. There is also some evidence that valaciclovir treatment of mothers carrying an infected fetus is feasible, safe and might be effective. This review provides an update on the evidence for diagnosis, prognosis and treatment of congenital infection in the antenatal period. These suggest a benefit to a proactive approach for prenatal congenital infections.
KEYWORDS:
cytomegalovirus; fetus; hyperimmune globulin; imaging; serology; valaciclovir
PMID: 27923540 DOI: 10.1016/j.bpobgyn.2016.10.005
Congenital Cytomegalovirus Infection in the Absence of Maternal Cytomegalovirus-IgM Antibodies
Fetal Diagn Ther. 2017 Mar 4. doi: 10.1159/000456615. [Epub ahead of print]
Gunkel J1, van der Knoop BJ, Nijman J, de Vries LS, Manten GT, Nikkels PG, Murk JL, de Vries JI, Wolfs TF.
Abstract
BACKGROUND: Congenital cytomegalovirus (cCMV) infections are the most prevalent intrauterine infections worldwide and are the result of maternal primary or non-primary infections. Early maternal primary infections are thought to carry the highest risk of fetal developmental abnormalities as seen by ultrasound; however, non-primary infections may prove equally detrimental. METHODS/RESULTS: This case series presents 5 cases with fetal abnormalities detected in the second and third trimester, in which cCMV infection was ruled out due to negative maternal CMV-IgM. DISCUSSION: This series highlights the possible pitfalls in serology interpretation and fetal diagnosis necessary for appropriate parental counseling. Once fetal abnormalities have been confirmed and cCMV is suspected, maternal CMV serostatus and fetal infection should be determined. Maternal CMV serology may be ambiguous; therefore, caution should be exercised when interpreting the results. © 2017 S. Karger AG, Basel.
PMID 28259882 DOI: 10.1159/000456615
Prenatal diagnosis of congenital cytomegalovirus infection in 115 cases: a 5 years' single center experience
Prenat Diagn. 2017 Feb 16. doi: 10.1002/pd.5025. [Epub ahead of print]
Enders M1, Daiminger A1, Exler S1, Ertan K2, Enders G1, Bald R2.
Abstract
OBJECTIVE: The objective of this study is to investigate the diagnostic value of invasive prenatal diagnosis (PD) of congenital cytomegalovirus (CMV) infection from amniotic fluid (AF) and fetal blood (FB). METHODS: A retrospective study was conducted on 115 pregnancies with CMV primary infection. A total of 111 AF and 106 FB samples were investigated for various virological and non-virological markers. Detailed ultrasound examinations were performed at time of PD. RESULTS: Overall sensitivity of CMV PCR in FB (75.6%; 95%CI 60-87) and AF (72.7%; 95%CI 57-85) was comparable. In women with amniocentesis >8 weeks between seroconversion and PD, we did not observe significant differences between amniocentesis performed ≥17 + 0 (sensitivity 90.9%; 95%CI 71-99) and ≥20 + 0 gestational weeks (sensitivity 90.0%; 95%CI 68-99). Virological markers in FB were higher in symptomatic compared with asymptomatic fetuses (p < 0.05). No significant differences were observed for non-virological markers. However, platelet counts <120 × 10e9/L and beta-2 microglobulin values >14 mg/L were more frequently found in fetuses with severe ultrasound abnormalities compared with fetuses with no or mild abnormalities (p < 0.001). CONCLUSION: Optimal timing of amniocentesis in women with primary infection in early gestation should be reevaluated in a prospective study. Analysis of FB markers may be beneficial in the individual management of pregnant women with confirmed congenital CMV infection. © 2017 John Wiley & Sons, Ltd. © 2017 John Wiley & Sons, Ltd.
PMID 28207161 DOI: 10.1002/pd.5025
Congenital cytomegalovirus infection: management update
Curr Opin Infect Dis. 2017 Mar 23. doi: 10.1097/QCO.0000000000000368. [Epub ahead of print]
Khalil A1, Jones C, Ville Y.
Abstract
PURPOSE OF REVIEW: Until recently, management options in congenital cytomegalovirus (cCMV) infection have been either conservative or termination of pregnancy. However, medical therapies aimed at reducing the risk of infection and/or its severity have recently been investigated. RECENT FINDINGS: In a phase 2 open label, nonrandomized trial, valaciclovir (ValACV) was given to women carrying a CMV-infected fetus. ValACV was associated with a greater proportion of asymptomatic neonates when compared with a historical cohort (82 vs. 43%). However, the study design and the small number of treated women limit its applicability. Even though initial observational data suggested that hyperimmune globulin (HIG) therapy in pregnancy was associated with a significantly lower risk of cCMV, its efficacy has not been borne out in a subsequent phase 2 randomized, placebo controlled, double-blind study [cCMV 30% in the HIG group, 44% in the placebo group (P = 0.13)]. Furthermore, 11% of fetuses in the HIG group had transient or permanent abnormalities, compared with 16% in the placebo group. SUMMARY: ValACV might have a promising role in the antenatal treatment of cCMV infection, but definitive recommendations require further research. The use of HIG should currently be limited to the research setting.Video abstract http://links.lww.com/COID/A18.
PMID 28338486 DOI: 10.1097/QCO.0000000000000368
2016
Cytomegalovirus Infection during Pregnancy and Its Impact on the Intrauterine Fetal Development - Case Report
Open Access Maced J Med Sci. 2016 Sep 15;4(3):449-452. Epub 2016 Aug 8.
Angelova M1, Kovachev E2, Todorov N1. Author information Abstract AIM: The aim of this publication is to present a case of CMV infection during pregnancy, with clinical manifestations of the development of microcephaly and simultaneous dilatation of the 3rd and 4th brain ventricle at 23 weeks gestation. This article discusses the role of ultrasound screening in the second trimester of pregnancy. CASE PRESENTATION: We present the case of a 25-year-old woman with the initials S.K. in her second pregnancy that came to our antenatal Consulting Centre. The first screening for blood count, blood group, biochemistry and serology showed results within the reference range. The patient came for a second comprehensive biochemical screening at 17 - 18 weeks gestation. The results showed the low genetic risk of congenital anomalies. Fetal morphology of the fetus was normal. S.K. came again for consultation at 22 weeks gestation in connection with the admittance of her first 3-year-old child to the hospital because of pneumonia. Serological tests of the child had shown elevated CMV titer - specific IgM. Then we made new serological tests of the patient and the results have shown that the patient was most likely infected by CMV primarily in the first trimester of pregnancy. After consulting about the risk of transmission of CMV to the fetus, the woman chose monthly ultrasound scans and refused amniocentesis. At 36 weeks gestation, in addition to the microcephaly already established, enlargement of the IV brain ventricle at the expense of underdevelopment of the cerebellum was noticed. Also, 2nd to 3rd stage of placenta maturity and low quantity of amniotic fluid was established. A male fetus of weight 2,890 g and height 50 cm was delivered. The fetus was with skin petechiae and hepatosplenomegaly. Neurological examination showed no abnormalities. CONCLUSIONS: In the described case the time interval between infection and ultrasonic manifestations is more than 17 weeks. The long interval between infection and occurrence of ultrasound markers can be a good prediction sign, as it may reflect less aggressive viral infection than present in cases where similar ultrasound findings were obtained shortly after infection of the mother. KEYWORDS: Cytomegalovirus infection; a case report; pregnancy PMID: 27703572 PMCID: PMC5042632 DOI: 10.3889/oamjms.2016.078
Clinical Implications for Children Born With Congenital Cytomegalovirus Infection Following a Negative Amniocentesis
Clin Infect Dis. 2016 Apr 24. pii: ciw237. [Epub ahead of print]
Bilavsky E1, Pardo J2, Attias J3, Levy I4, Magny JF5, Ville Y6, Leruez-Ville M7, Amir J1.
Abstract
BACKGROUND: Recently, congenital cytomegalovirus (cCMV) infection was reported irrespective of a negative amniotic fluid prenatal analysis for cytomegalovirus (CMV). The question of whether this phenomenon represents low sensitivity of the test or late development of fetal infection (after amniocentesis) was discussed, but not answered. However, if late transmission is the rule, then infants born with cCMV after negative amniocentesis would be expected to carry better prognosis than those who tested positive. METHODS: Data of all infants with cCMV infection, followed in 2 pediatric centers from 2006 to 2015, were reviewed. Infant outcome after birth of symptomatic vs asymptomatic disease was compared with infants born after a negative amniocentesis (study group) and those with a positive amniocentesis (control group). RESULTS: Amniocentesis was performed in 301 pregnancies of our cohort of infants with cCMV and was negative for CMV in 47 (15.6%). There were fewer symptomatic cCMV neonates in the study group than in the control group (4.3% vs 25%; P < .001). Hearing impairment at birth was also less frequent in the study group (2.2% vs 17.4%; P = .012). None of the children in the study group had neurologic sequelae at long-term follow up, compared with 13 (14.1%) in the control group (P < .001). CONCLUSIONS: Although negative amniocentesis does not exclude cCMV, infants with cCMV born after a negative amniocentesis seldom present with mild clinical symptoms or cerebral ultrasound features at birth. These children also have a very good long-term outcome. Our findings support the theory of a late development of fetal infection, after the time of the amniocentesis. © The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail journals.permissions@oup.com. KEYWORDS: amniocentesis; congenital cytomegalovirus; congenital infection; cytomegalovirus; pregnancy
PMID 27114380
2015
Neuro-Imaging Findings in Infants with Congenital Cytomegalovirus Infection: Relation to Trimester of Infection
Neonatology. 2015 Mar 10;107(4):289-296.
Oosterom N1, Nijman J, Gunkel J, Wolfs TF, Groenendaal F, Verboon-Maciolek MA, de Vries LS.
Abstract
BACKGROUND: Congenital cytomegalovirus (cCMV) infection early in pregnancy may result in major disabilities. Cerebral abnormalities detected using cranial ultrasound (cUS) and magnetic resonance imaging (MRI) have been related to neurological sequelae. OBJECTIVE: To evaluate the additional value of MRI and assess the relationship between time of infection during pregnancy and outcome in infants with cCMV infection. METHODS AND STUDY DESIGN: Demographic and clinical data were collected in infants with cCMV infection (1992-2013). Trimester of infection, neuro-imaging results and outcome were reviewed. Cerebral abnormalities were categorized into none, mild (lenticulostriate vasculopathy, germinolytic cysts, high signal intensity on T2-weighted images) and severe (migrational disorder, ventriculomegaly, cerebellar hypoplasia). Results were statistically analysed. RESULTS: Thirty-six infants were eligible for analysis. cUS was performed in all and cranial MRI in 20 infants. Migrational disorders were only diagnosed using MRI (p < 0.01). In 17 infants trimester of infection was ascertained. Seven out of 10 infants infected during the first trimester had severe abnormalities on cUS (5 confirmed on MRI) and adverse sequelae; 3 had no/mild abnormalities on cUS/MRI and normal outcome. Two out of 3 infants infected during the second trimester with no/mild abnormalities on cUS/MRI had normal outcome; 1 with mild cUS and MRI abnormalities developed sensorineural hearing loss. Four infants infected during the third trimester with no/mild abnormalities on cUS/MRI had normal outcome. CONCLUSION: Infants with a first trimester cCMV infection are most at risk of severe cerebral abnormalities and neurological sequelae. MRI, and not cUS, enables an early diagnosis of migrational disorders, which can improve prediction of outcome. © 2015 S. Karger AG, Basel.
PMID 25790782
2013
Human fetal inner ear involvement in congenital cytomegalovirus infection
Acta Neuropathol Commun. 2013 Oct 2;1(1):63.
Gabrielli L, Bonasoni MP, Santini D, Piccirilli G, Chiereghin A, Guerra B, Landini MP, Capretti MG, Lanari M, Lazzarotto T. Source Operative Unit of Clinical Microbiology, St, Orsola-Malpighi General Hospital, University of Bologna, Via Massarenti 9, 40138, Bologna, Italy. liliana.gabrielli@aosp.bo.it.
Abstract BACKGROUND: Congenital cytomegalovirus (CMV) infection is a leading cause of sensorineural hearing loss (SNHL). The mechanisms of pathogenesis of CMV-related SNHL are still unclear. The aim is to study congenital CMV-related damage in the fetal inner ear, in order to better understand the underlying pathophysiology behind CMV-SNHL. RESULTS: We studied inner ears and brains of 20 human fetuses, all at 21 week gestational age, with a high viral load in the amniotic fluid, with and without ultrasound (US) brain abnormalities. We evaluated histological brain damage, inner ear infection, local inflammatory response and tissue viral load.Immunohistochemistry revealed that CMV was positive in 14/20 brains (70%) and in the inner ears of 9/20 fetuses (45%). In the cases with inner ear infection, the marginal cell layer of the stria vascularis was always infected, followed by infection in the Reissner's membrane. The highest tissue viral load was observed in the inner ear with infected Organ of Corti. Vestibular labyrinth showed CMV infection of sensory cells in the utricle and in the crista ampullaris.US cerebral anomalies were detected in 6 cases, and in all those cases, the inner ear was always involved. In the other 14 cases with normal brain scan, histological brain damage was present in 8 fetuses and 3 of them presented inner ear infection. CONCLUSIONS: CMV-infection of the marginal cell layer of the stria vascularis may alter potassium and ion circulation, dissipating the endocochlear potential with consequent SNHL. Although abnormal cerebral US is highly predictive of brain and inner ear damage, normal US findings cannot exclude them either.
PMID 24252374
2012
Human Cytomegalovirus Infection Dysregulates the Canonical Wnt/β-catenin Signaling Pathway
PLoS Pathog. 2012 Oct;8(10):e1002959. doi: 10.1371/journal.ppat.1002959. Epub 2012 Oct 11.
Angelova M, Zwezdaryk K, Ferris M, Shan B, Morris CA, Sullivan DE. Source Department of Microbiology and Immunology, Tulane University School of Medicine, New Orleans, Louisiana, United States of America.
Abstract
Human Cytomegalovirus (HCMV) is a ubiquitous herpesvirus that currently infects a large percentage of the world population. Although usually asymptomatic in healthy individuals, HCMV infection during pregnancy may cause spontaneous abortions, premature delivery, or permanent neurological disabilities in infants infected in utero. During infection, the virus exerts control over a multitude of host signaling pathways. Wnt/β-catenin signaling, an essential pathway involved in cell cycle control, differentiation, embryonic development, placentation and metastasis, is frequently dysregulated by viruses. How HCMV infection affects this critical pathway is not currently known. In this study, we demonstrate that HCMV dysregulates Wnt/β-catenin signaling in dermal fibroblasts and human placental extravillous trophoblasts. Infection inhibits Wnt-induced transcriptional activity of β-catenin and expression of β-catenin target genes in these cells. HCMV infection leads to β-catenin protein accumulation in a discrete juxtanuclear region. Levels of β-catenin in membrane-associated and cytosolic pools, as well as nuclear β-catenin, are reduced after infection; while transcription of the β-catenin gene is unchanged, suggesting enhanced degradation. Given the critical role of Wnt/β-catenin signaling in cellular processes, these findings represent a novel and important mechanism whereby HCMV disrupts normal cellular function.
- dysregulates the canonical Wnt/b-catenin signaling pathway in human dermal fibroblasts and placental EVTs.
- inhibits canonical Wnt signaling by causing sequestration and degradation of endogenous b-catenin, thus preventing its downstream activities.
- Since the Wnt/b-catenin pathway is an evolutionarily conserved pathway involved in a diverse range of biological functions such as cell cycle control, cell differentiation, embryonic development, placentation and metastasis, the finding that HCMV impairs this pathway becomes globally important for understanding viral pathogenesis, particularly that related to HCMV disease.
PMID 23071438
http://www.plospathogens.org/article/info%3Adoi%2F10.1371%2Fjournal.ppat.1002959
Impaired Surfactant Production by Alveolar Epithelial Cells in a SCID-hu Lung Mouse Model of Congenital Human Cytomegalovirus Infection
J Virol. 2012 Dec;86(23):12795-805. doi: 10.1128/JVI.01054-12. Epub 2012 Sep 12.
Maidji E, Kosikova G, Joshi P, Stoddart CA. Source Division of Experimental Medicine, Department of Medicine, San Francisco General Hospital, University of California, San Francisco, California, USA.
Abstract
Human cytomegalovirus (HCMV) is the leading viral cause of birth defects and life-threatening lung-associated diseases in premature infants and immunocompromised children. Although the fetal lung is a major target organ of the virus, HCMV lung pathogenesis has remained unexplored, possibly as a result of extreme host range restriction. To overcome this hurdle, we generated a SCID-hu lung mouse model that closely recapitulates the discrete stages of human lung development in utero. Human fetal lung tissue was implanted into severe combined immunodeficient (CB17-scid) mice and inoculated by direct injection with the VR1814 clinical isolate of HCMV. Virus replication in the fetal lung was assessed by the quantification of infectious virus titers and HCMV genome copies and the detection of HCMV proteins by immunohistochemistry and Western blotting. We show that HCMV efficiently replicated in the lung implants during a 2-week period, forming large viral lesions. The virus productively infected alveolar epithelial and mesenchymal cells, imitating congenital infection of the fetal lung. HCMV replication triggered apoptosis near and within the viral lesions and impaired the production of surfactant proteins in the alveolar epithelium. Our findings highlight that congenital and neonatal HCMV infection can adversely impact lung development, leading to pneumonia and acute lung injury. We have successfully developed a small-animal model that closely recapitulates fetal and neonatal lung development and provides a valuable, biologically relevant tool for an understanding of the lung pathogenesis of HCMV as well as other human respiratory viruses. Additionally, this model would greatly facilitate the development and testing of new antiviral therapies for HCMV along with select human pulmonary pathogens.
PMID 22973041
Low IgG avidity and ultrasound fetal abnormality predict congenital cytomegalovirus infection
J Med Virol. 2012 Dec;84(12):1928-33. doi: 10.1002/jmv.23387.
Sonoyama A, Ebina Y, Morioka I, Tanimura K, Morizane M, Tairaku S, Minematsu T, Inoue N, Yamada H. Source Department of Obstetrics and Gynecology, Kobe University Graduate School of Medicine, Kobe, Japan.
Abstract
Cytomegalovirus (CMV) causes congenital infection with high mortality and morbidity rates in affected neonates. The aim of this study was to assess whether prenatal clinical or laboratory findings in pregnant women who had high risks for primary CMV infection predicted the presence of congenital infection. Fifty pregnant women who had serum CMV IgG and positive or borderline tests for serum CMV IgM were included in this prospective study. Serum IgG avidity was measured, and PCR was conducted for CMV DNA in maternal serum, urine, and uterine cervical secretion. All neonates underwent PCR testing for CMV DNA in the urine for the presence of congenital infection. Risk factors were compared between congenital infection group and group without congenital infection. As a result, nine neonates (18%) were diagnosed as having congenital infection. The frequencies of ultrasound fetal abnormality and positive test for CMV DNA in cervical secretion, CMV IgM titer and IgM/IgG ratio in the congenital infection group were significantly higher than those in the group without congenital infection. Conversely, IgG avidity index in the congenital infection group was significantly lower than that in the group without congenital infection. By multivariate logistic regression analyses, IgG avidity index (Odds ratio 0.91, 95% CI: 0.83-0.99) and ultrasound fetal abnormality (291.22, 2.72-31125.05), were selected independently as significant signs predictive of congenital CMV infection. Among pregnant women with positive or borderline tests for CMV IgM, when they have findings of low serum CMV IgG avidity or ultrasound fetal abnormality, the probability of congenital CMV infection may increase. J. Med. Virol. 84:1928-1933, 2012. © 2012 Wiley Periodicals, Inc. Copyright © 2012 Wiley Periodicals, Inc.
PMID 23080498
A preliminary evaluation of safety and efficacy of standard intravenous immunoglobulins in pregnant women with primary Cytomegalovirus infection
Clin Vaccine Immunol. 2012 Oct 24.
Polilli E, Parruti G, D'Arcangelo F, Tracanna E, Clerico L, Savini V, D'Antonio F, Rosati M, Manzoli L, D'Antonio D, Nigro G. Source Microbiology and Virology Unit, General Hospital of Pescara, Pescara, Italy.
Abstract
Hyperimmune globulins were reported to prevent and treat fetal CMV infection during pregnancy. Here we report that infusions of standard human intravenous immunoglobulin significantly increase CMV IgG titres and avidity indexes in pregnant women, paving the way to their use for passive transfer of maternal CMV humoral immunity to foetuses. Preliminary data on perinatal outcomes of the first 67 newborns are encouraging.
http://ClinicalTrials.gov - serial number NCT01659684
PMID 23100477
http://cvi.asm.org/content/early/2012/10/18/CVI.00509-12.long
Chronic Histiocytic Intervillositis with Cytomegalovirus Placentitis in a Case of Hydrops Fetalis
Fetal Pediatr Pathol. 2012 Mar 23.
Taweevisit M, Sukpan K, Siriaunkgul S, Thorner PS. Source Department of Pathology, Chulalongkorn University, Pathumwan , Bangkok , Thailand. Abstract Chronic histiocytic intervillositis (CHI) is an infrequent inflammatory placental disorder associated with unfavorable pregnancy outcomes and a high rate of recurrence. This disorder is thought to reflect a maternal delayed hypersensitivity response to fetal antigen(s) in placental tissue. We report a case of a 20-week-gestation hydropic fetus in which the placenta showed chronic histiocytic intervillositis with cytomegalovirus placentitis. Immunophenotyping studies supported a delayed hypersensitivity response. This is the first report of these two diseases co-occurring, raising the possibility of a relationship between chronic histiocytic intervillositis and infection. Chronic histiocytic intervillositis may represent an idiosyncratic immune response, in this case to cytomegalovirus.
PMID 22443234
2011
Update on the prevention, diagnosis and management of cytomegalovirus infection during pregnancy
Clin Microbiol Infect. 2011 Apr 25. doi: 10.1111/j.1469-0691.2011.03564.x.
Lazzarotto T, Guerra B, Gabrielli L, Lanari M, Landini MP. Source Department of Haematology, Oncology and Laboratory Medicine, Operative Unit of Clinical Microbiology Department of Obstetrics and Gynaecology, St Orsola Malpighi General Hospital, University of Bologna, Bologna Operative Unit of Paediatrics and Neonatology, La Scaletta Hospital, Imola-Bologna, Italy.
Abstract
Clin Microbiol Infect ABSTRACT: Human cytomegalovirus (CMV) is the leading cause of congenital infection, with morbidity and mortality at birth and sequelae. Each year approximately 1-7% (Rev Med Virol 2010; 20: 311) of pregnant women acquire a primary CMV infection. Of these, about 30-40% transmit infection to their fetuses. The risk of serious fetal injury is greatest when maternal infection develops in the first trimester or early in the second trimester. Between 10 and 15% of congenitally infected infants are acutely symptomatic at birth and most of the survivors have serious long-term complications. Until a few years ago, laboratory testing was not possible to precisely define the maternal immune status, the recent development of advanced serological tests (IgG avidity test, IgM immunoblot and neutralizing antibody testing) allow us to identify, among pregnant women with suspected CMV, those with primary infection who are therefore at high risk of transmitting CMV to the fetus. This is done with the use of a screening test. As most maternal infections are asymptomatic, the only way to disclose primary infection is to implement specific serological testing as early in pregnancy as possible (before week 12-16 of gestation). Given the high risk of mother-fetus transmission and fetal damage, prenatal diagnosis is recommended to women with primary CMV infection contracted in the first half of pregnancy and in case of fetal abnormalities suggestive of infection. The correct interpretation of serological and virological tests followed by appropriate counselling by an expert physician is an effective tool to reduce the number of unnecessary pregnancy terminations by over 70% (Am J Obstet Gynecol 2007; 196: 221.e1).
© 2011 The Authors. Clinical Microbiology and Infection © 2011 European Society of Clinical Microbiology and Infectious Diseases.
PMID 21631642
Inner ear lesions in congenital cytomegalovirus infection of human fetuses
Acta Neuropathol. 2011 Dec;122(6):763-74. Epub 2011 Oct 28.
Teissier N, Delezoide AL, Mas AE, Khung-Savatovsky S, Bessières B, Nardelli J, Vauloup-Fellous C, Picone O, Houhou N, Oury JF, Van Den Abbeele T, Gressens P, Adle-Biassette H. Source Pediatric ENT Department, Robert Debré Hospital, APHP, Paris, France.
Abstract
Congenital cytomegalovirus (CMV) infection is the leading cause of non-hereditary congenital sensorineural hearing loss (SNHL). The natural course and the pathophysiology of inner ear lesions during human fetal CMV infection have not yet been reported. Inner ear lesions were investigated in six CMV-infected fetuses aged 19-35 postconceptional weeks and correlated with central nervous system (CNS) lesions. All the fetuses had high viral loads in the amniotic fluid and severe visceral and CNS lesions visible by ultrasound. Diffuse lesions consisting of both cytomegalic cells containing inclusion bodies and inflammation were found within all studied structures including the inner ear, brain, other organs, and placenta, suggesting hematogenous dissemination. Cochlear infection was consistently present and predominated in the stria vascularis (5/6), whereas the supporting cells in the organ of Corti were less often involved (2/6). Vestibular infection, found in 4/6 cases, was florid; the non-sensory epithelia, including the dark cells, were extensively infected. The endolymphatic sac was infected in 1 of 3 cases. The severity of inner ear infection was correlated with the CNS lesions, confirming the neurotropism of CMV. This study documenting infection of the structures involved in endolymph secretion and potassium homeostasis in fetuses with high amniotic fluid viral loads suggests that potassium dysregulation in the endolymphatic compartment of the inner ear may lead to secondary degeneration of the sensory structures. In addition, the occurrence of SNHL depends on the intensity and duration of the viral infection and inflammation.
PMID 22033878
In vitro study on human cytomegalovirus affecting early pregnancy villous EVT's invasion function
Virol J. 2011 Mar 11;8:114.
Tao L, Suhua C, Juanjuan C, Zongzhi Y, Juan X, Dandan Z. Source Department of Obsterics and Gynecology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Abstract
BACKGROUND:
Human cytomegalovirus (HCMV) is the most common pathogen in uterus during pregnancy, which may lead to some serious results such as miscarriage, stillbirth, cerebellar malformation, fetus developmental retardation, but its pathogenesis has not been fully explained. The hypofunction of extravillous cytotrophoblast (EVT) invasion is the essential pathologic base of some complications of pregnancy. c-erbB-2 is a kind of oncogene protein and closely linked with embryogenesis, tissue repair and regeneration. Matrix metalloproteinase (MMP) is one of the key enzymes which affect EVT migration and invasion function. The expression level changes of c-erbB-2, MMP-2 and MMP-9 can reflect the changes of EVT invasion function.
RESULTS:
To explore the influence of HCMV on the invasion function of EVT, we tested the protein expression level changes of c-erbB-2, MMP-2 and MMP-9 in villous explant cultured in vitro infected by HCMV, with the use of immunohistochemistry SP method and western blot. We confirmed that HCMV can reproduce and spread in early pregnancy villus; c-erbB-2 protein mainly expressed in normal early pregnancy villous syncytiotrophoblast (ST) remote plasma membrane and EVT, especially remote EVT cell membrane in villous stem cell column, little expressed in ST proximal end cell membrane and interstitial cells; MMP-2 protein primarily expressed in early pregnancy villous EVT endochylema and rarely in villous trophoblast (VT), ST and interstitial cells; MMP-9 protein largely expressed in early pregnancy villous mesenchyme, EVT and VT endochylema. Compared with control group, the three kinds of protein expression level in early pregnancy villus of virus group significantly decreased (P < 0.05).
CONCLUSION:
HCMV can infect villus in vitro and cause the decrease of early pregnancy villous EVT's invasion function.
PMID 21392403
http://www.virologyj.com/content/8/1/114
2010
Update on the current status of cytomegalovirus vaccines
Expert Rev Vaccines. 2010 Nov;9(11):1303-14.
Sung H, Schleiss MR. Source University of Minnesota Medical School, Department of Pediatrics, Center for Infectious Diseases and Microbiology Translational Research, 2001 6th Street SE, Minneapolis, MN 55455, USA.
Abstract
Human cytomegalovirus (HCMV) is ubiquitous in all populations, and is the most commonly recognized cause of congenital viral infection in developed countries. On the basis of the economic costs saved and the improvement in quality of life that could potentially be conferred by a successful vaccine for prevention of congenital HCMV infection, the Institute of Medicine has identified HCMV vaccine development as a major public health priority. An effective vaccine could potentially also be beneficial in preventing or ameliorating HCMV disease in immunocompromised individuals. Although there are no licensed HCMV vaccines currently available, enormous progress has been made in the last decade, as evidenced by the recently reported results of a Phase II trial of a glycoprotein B vaccine for the prevention of HCMV infection in seronegative women of childbearing age. HCMV vaccines currently in clinical trials include: glycoprotein B subunit vaccines; alphavirus replicon particle vaccines; DNA vaccines; and live-attenuated vaccines. A variety of vaccine strategies are also being examined in preclinical systems and animal models of infection. These include: recombinant vesicular stomatitis virus vaccines; recombinant modified vaccinia virus Ankara; replication-deficient adenovirus-vectored vaccines; and recombinant live-attenuated virus vaccines generated by mutagenesis of cloned rodent CMV genomes maintained as bacterial artificial chromosomes in Escherichia coli. In this article, we provide an overview of the current state of clinical trials and preclinical development of vaccines against HCMV, with an emphasis on studies that have been conducted in the past 5 years. We also summarize a number of recent advances in the study of the biology of HCMV, particularly with respect to epithelial and endothelial cell entry of the virus, which have implications for future vaccine design.
PMID 21087108
Dried blood spot real-time polymerase chain reaction assays to screen newborns for congenital cytomegalovirus infection
JAMA. 2010 Apr 14;303(14):1375-82.
Boppana SB, Ross SA, Novak Z, Shimamura M, Tolan RW Jr, Palmer AL, Ahmed A, Michaels MG, Sánchez PJ, Bernstein DI, Britt WJ, Fowler KB; National Institute on Deafness and Other Communication Disorders CMV and Hearing Multicenter Screening (CHIMES) Study. Collaborators (58)
Source UAB Department of Pediatrics, CHB 114, 1600 Sixth Ave S, Birmingham, AL 35233, USA. sboppana@peds.uab.edu Abstract CONTEXT: Reliable methods to screen newborns for congenital cytomegalovirus (CMV) infection are needed for identification of infants at increased risk of hearing loss. Since dried blood spots (DBS) are routinely collected for metabolic screening from all newborns in the United States, there has been interest in using DBS polymerase chain reaction (PCR)-based methods for newborn CMV screening. OBJECTIVE: To determine the diagnostic accuracy of DBS real-time PCR assays for newborn CMV screening. DESIGN, SETTING, AND PARTICIPANTS: Between March 2007 and May 2008, infants born at 7 US medical centers had saliva specimens tested by rapid culture for early antigen fluorescent foci. Results of saliva rapid culture were compared with a single-primer (March 2007-December 2007) and a 2-primer DBS real-time PCR (January 2008-May 2008). Infants whose specimens screened positive on rapid culture or PCR had congenital infection confirmed by the reference standard method with rapid culture testing on saliva or urine. MAIN OUTCOME MEASURES: Sensitivity, specificity, and positive and negative likelihood ratios (LRs) of single-primer and 2-primer DBS real-time PCR assays for identifying infants with confirmed congenital CMV infection. RESULTS: Congenital CMV infection was confirmed in 92 of 20,448 (0.45%; 95% confidence interval [CI], 0.36%-0.55%) infants. Ninety-one of 92 infants had positive results on saliva rapid culture. Of the 11,422 infants screened using the single-primer DBS PCR, 17 of 60 (28%) infants had positive results with this assay, whereas, among the 9026 infants screened using the 2-primer DBS PCR, 11 of 32 (34%) screened positive. The single-primer DBS PCR identified congenital CMV infection with a sensitivity of 28.3% (95% CI, 17.4%-41.4%), specificity of 99.9% (95% CI, 99.9%-100%), positive LR of 803.7 (95% CI, 278.7-2317.9), and negative LR of 0.7 (95% CI, 0.6-0.8). The positive and negative predictive values of the single-primer DBS PCR were 80.9% (95% CI, 58.1%-94.5%) and 99.6% (95% CI, 99.5%-99.7%), respectively. The 2-primer DBS PCR assay identified infants with congenital CMV infection with a sensitivity of 34.4% (95% CI, 18.6%-53.2%), specificity of 99.9% (95% CI, 99.9%-100.0%), positive LR of 3088.9 (95% CI, 410.8-23 226.7), and negative LR of 0.7 (95% CI, 0.5-0.8). The positive and negative predictive values of the 2-primer DBS PCR were 91.7% (95% CI, 61.5%-99.8%) and 99.8% (95% CI, 99.6%-99.9%), respectively. CONCLUSION: Among newborns, CMV testing with DBS real-time PCR compared with saliva rapid culture had low sensitivity, limiting its value as a screening test. Comment in JAMA. 2010 Jul 28;304(4):407; author reply 408. JAMA. 2010 Jul 28;304(4):407-8; author reply 408. JAMA. 2010 Apr 14;303(14):1425-6.
PMID 20388893
Neurodevelopmental outcome following congenital cytomegalovirus infection in preterm infants with twin-to-twin transfusion syndrome: a case report
Klin Padiatr. 2010 Sep;222(5):312-4. Epub 2010 Aug 30.
Griesmaier E, Neubauer V, Blum S, Trawöger R, Keller M, Kiechl-Kohlendorfer U. Source Innsbruck Medical University, Department of Pediatrics IV, Innsbruck, Austria. Elke.Griesmaier@i-med.ac.at
Abstract
Twin-to-twin transfusion syndrome and conital cytomegalovirus infection bear the risk of brain damage. In the 27th week of gestation of a twin pregnancy a Caesarean section was performed because of pathological cardiotocogram and Doppler ultrasonography of the second twin (recipient). Both infants presented with severe, persistent thrombocytopenia, elevated liver enzymes and direct hyperbilirubinemia. Primary congenital CMV infection was diagnosed. Both twins showed severe neuropathological symptoms, pathological aEEG with seizure activity and severe neurodevelopmental delay at corrected age of 12 months. The severity of brain pathology, the complex etiology, its consequence for neurotion with extreme prematurity make this case of special interest. Georg Thieme Verlag KG Stuttgart, New York.
PMID 20806166
Transmission of cytomegalovirus via breast milk to the prematurely born infant: a systematic review
Clin Microbiol Infect. 2010 Aug;16(8):1172-8.
Kurath S, Halwachs-Baumann G, Müller W, Resch B. Source Paediatric Department, Division of Neonatology, Research Unit for Neonatal Infectious Diseases and Epidemiology, Medical University of Graz, Graz, Austria.
Abstract
To analyse current data on transmission of human cytomegalovirus (HCMV) via breast milk with subsequent symptomatic HCMV infection of the preterm infant and to report on long-term follow-up, a systematic literature review was performed using EMBASE, MEDLINE and CINAHL (January 1966 to December 2008) Studies were included for analysis if congenital HCMV infection was excluded and transmission via breast milk was either confirmed or strongly suspected. Twenty-six studies were included for analysis. Maternal HCMV-IgG-positivity was reported to be in the range 51.6-100% (median 81.6%), HCMV-IgG detection in breast milk in the range 67-97.2% (median 80%) and HCMV-positivity of the infants in the range 5.7-58.6%. Symptomatic HCMV disease occurred in 0-34.5% (median 3.7%) and severe sepsis-like syndrome in 0-13.8% (median 0.7%). Data on long-term outcome of preterm infants with symptomatic HCMV infection revealed a low risk for mild neurological and cognitive sequelae, without hearing impairment. Recommendations for high-risk preterm infants diverged markedly. The current data report low rates of symptomatic disease after transmission of HCMV via breast milk to the preterm infant without evidence of certain long-term sequelae. The results of our review do not support a general approach, either by avoidance or pasteurization of breast milk, in high-risk preterm infants.
PMID 20670291
2009
Histological findings in foetuses congenitally infected by cytomegalovirus
J Clin Virol. 2009 Dec;46 Suppl 4:S16-21. Epub 2009 Oct 30.
Gabrielli L, Bonasoni MP, Lazzarotto T, Lega S, Santini D, Foschini MP, Guerra B, Baccolini F, Piccirilli G, Chiereghin A, Petrisli E, Gardini G, Lanari M, Landini MP. Source St. Orsola Malpighi GH, University of Bologna, Italy. liliana.gabrielli@aosp.bo.it Abstract BACKGROUND: Congenital cytomegalovirus (CMV) infection is a major cause of central nervous system damage leading to sensorineural hearing loss, mental retardation and cerebral palsy. OBJECTIVES: Identify the type of organ involvement and understand the histopathogenesis of damage in foetuses of women with a CMV-highly positive amniotic fluid. STUDY DESIGN: 34 foetuses with congenital CMV infection documented by prenatal diagnosis were studied. Three foetuses died in utero. The remaining pregnancies were electively terminated at 20-21 weeks gestation. RESULTS: Foetal organs positive for CMV antigens were: placenta (100%), pancreas (100%), lung (87%), kidney (87%), liver (71%), brain (55%) and heart (44%). Inflammatory infiltrate was almost always present in CMV-infected foetal organs and the severity of the inflammatory response was correlated with the organ damage. Brain damage with necrosis was observed in 33% (9/27) and a mild telencephalic leukoencephalopathy in 22% (6/27) of foetuses studied. CONCLUSIONS: Focal necrosis was observed very frequently in organs such as pancreases, livers, hearts and kidneys. However the damage in these organs is likely to be resolved by parenchymal regeneration. Brain damage, which seems to be the results of a combined effect of viral infection, inflammatory infiltration and hypoxia due to severe placentitis, is less likely to be resolved because of the low regeneration ability of this organ.
PMID 19879801
2008
Cytomegalovirus induces abnormal chondrogenesis and osteogenesis during embryonic mandibular development
BMC Dev Biol. 2008 Mar 27;8:33.
Jaskoll T, Abichaker G, Sedghizadeh PP, Bringas P Jr, Melnick M.
Laboratory for Developmental Genetics, USC, Los Angeles, CA, USA. tjaskoll@usc.edu
Abstract
BACKGROUND: Human clinical studies and mouse models clearly demonstrate that cytomegalovirus (CMV) disrupts normal organ and tissue development. Although CMV is one of the most common causes of major birth defects in humans, little is presently known about the mechanism(s) underlying CMV-induced congenital malformations. Our prior studies have demonstrated that CMV infection of first branchial arch derivatives (salivary glands and teeth) induced severely abnormal phenotypes and that CMV has a particular tropism for neural crest-derived mesenchyme (NCM). Since early embryos are barely susceptible to CMV infection, and the extant evidence suggests that the differentiation program needs to be well underway for embryonic tissues to be susceptible to viral infection and viral-induced pathology, the aim of this study was to determine if first branchial arch NCM cells are susceptible to mCMV infection prior to differentiation of NCM derivatives. RESULTS: E11 mouse mandibular processes (MANs) were infected with mouse CMV (mCMV) for up to 16 days in vitro. mCMV infection of undifferentiated embryonic mouse MANs induced micrognathia consequent to decreased Meckel's cartilage chondrogenesis and mandibular osteogenesis. Specifically, mCMV infection resulted in aberrant stromal cellularity, a smaller, misshapen Meckel's cartilage, and mandibular bone and condylar dysmorphogenesis. Analysis of viral distribution indicates that mCMV primarily infects NCM cells and derivatives. Initial localization studies indicate that mCMV infection changed the cell-specific expression of FN, NF-kappaB2, RelA, RelB, and Shh and Smad7 proteins. CONCLUSION: Our results indicate that mCMV dysregulation of key signaling pathways in primarily NCM cells and their derivatives severely disrupts mandibular morphogenesis and skeletogenesis. The pathogenesis appears to be centered around the canonical and noncanonical NF-kappaB pathways, and there is unusual juxtaposition of abnormal stromal cells and surrounding matrix. Moreover, since it is critically important that signaling molecules are expressed in appropriate cell populations during development, the aberrant localization of components of relevant signaling pathways may reveal the pathogenic mechanism underlying mandibular malformations.
PMID 18371224
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2330031/
2007
Translational mini-review series on infectious disease: congenital cytomegalovirus infection: 50 years on
Clin Exp Immunol. 2007 Aug;149(2):205-10. Hassan J, Connell J. Source National Virus Reference Laboratory and Centre for Research into Infectious Disease, University College Dublin, Dublin, Ireland. jaythoon.hassan@ucd.ie
Abstract
Cytomegalovirus (CMV) is the leading cause of congenital viral infection, with an incidence of 0.5-3% of live births worldwide. Clinical evidence has shown hearing and vision loss, mental retardation and sometimes death in affected newborns. Primary maternal CMV infection during gestation poses a 40% risk of intrauterine transmission in contrast to recurrent infection. European laboratories have made significant progress in the last decade in solving diagnostic problems linked to infection in pregnancy. With the advances in CMV serology, such as detection of anti-CMV IgM by enzyme immunoassays (EIA), confirmed by Western blot, together with seroconversion and anti-CMV IgG avidity evaluation in pregnant mothers, can help to identify recent infection. Preventative measures such as screening for CMV in the routine serological work-up of pregnant women have been introduced in countries such as Spain and Italy. The development of specific T cell-mediated immune responses in mothers, fetus and neonates is now emerging with regard to antigen-specific CD4 and CD8 T cells, differentiation status, proliferative and cytokine responses. A protective vaccine against CMV is a major public health priority and the study of vaccines in animal model systems has identified potential strategies for interrupting transmission and preventing disease in newborns. Congenital CMV infection has a variable outcome and therefore novel diagnostic methods are required to identify those at risk and therapeutic interventions are needed to improve the long-term prognosis of those infected. CMV was first isolated in 1957. We are now 50 years on, so procrastination is not an option.
PMID 17635529
Cytomegalovirus-induced mirror syndrome associated with elevated levels of circulating antiangiogenic factors
Obstet Gynecol. 2007 Feb;109(2 Pt2):549-52.
Rana S, Venkatesha S, DePaepe M, Chien EK, Paglia M, Karumanchi SA. Source Maternal Fetal Medicine Division, Department of Obstetrics and Gynecology, Women and Infants Hospital, Brown University, Providence, Rhode Island 02905, USA. saroshrana@gmail.com Erratum in Obstet Gynecol. 2007 May;109(5):1207. Abstract BACKGROUND: We describe a case where Mirror syndrome was characterized by altered levels of antiangiogenic proteins (soluble fms-like tyrosine kinase 1 [sFlt1] and soluble endoglin). CASE: We describe a pregnant patient with severe fetal and placental edema induced by congenital cytomegalovirus (CMV) infection that was associated with preeclampsia. Fetal CMV was confirmed histologically, whereas antiangiogenic factors were demonstrated to be elevated in maternal but not fetal blood. The levels of sFlt1 and soluble endoglin in our patient's serum before delivery were 116.5 ng/mL (normal pregnancy 19.3 ng/mL and preeclampsia 66.0 ng/mL, representing mean values before delivery) and 107.4 ng/mL (normal pregnancy 18.7 ng/mL and preeclampsia 52.6 ng/mL, representing mean values before delivery), respectively. In contrast, the values of sFlt1 and soluble endoglin in the cord blood were relatively low at 2.1 ng/mL and 8.2 ng/mL, respectively. CONCLUSION: If this observation is confirmed, CMV infection may be cited as a cause of Mirror syndrome and preeclampsia phenotypes associated with this disorder may be related to increased circulating antiangiogenic factors. Comment in Obstet Gynecol. 2007 May;109(5):1205-6; author reply 1206.
PMID 17267891
2001
Epidemiology of transmission of cytomegalovirus from mother to preterm infant by breastfeeding
Lancet. 2001 Feb 17;357(9255):513-8.
Hamprecht K, Maschmann J, Vochem M, Dietz K, Speer CP, Jahn G. Source Institute of Medical Virology and Epidemiology of Viral Diseases, University Hospital of Tübingen, Germany. kshampre@med.uni-tuebingen.de
Abstract
BACKGROUND: Breastfeeding practices strongly influence the epidemiology of human cytomegalovirus infection. By contrast with term neonates, few data are available on transmission of infection from mothers to preterm infants during breastfeeding.
METHODS: 151 mothers and their 176 preterm infants (gestational age at birth <32 weeks or birthweight <1500 g) were prospectively screened for cytomegalovirus infection by serology, virus culture, and PCR. The roles of cell-free and cell-associated cytomegalovirus excretion during lactation were analysed longitudinally in relation to transmission, by maximum-likelihood estimates.
FINDINGS: Of the 69 seronegative breastfeeding control mothers, none had detectable cytomegalovirus DNA in breastmilk and none of their 80 infants shed the virus in urine. The proportion of cytomegalovirus reactivation in seropositive breastfeeding mothers was 96% (73 of 76). The early appearance of viral DNA in milk whey (median 3.5 days post partum in transmitters; 8 days in non-transmitters; p=0.025) and infectious virus in milk whey (10 days and 16 days, respectively; p=0.005) were risk factors for transmission. The cumulative rate of transmission was 37% (27 of 73 mothers; 33 infants). The infection of the neonates had a mean incubation time of 42 days (95% CI 28-69). About 50% of the infected infants had no symptoms, but four had sepsis-like symptoms.
INTERPRETATION: The proportion of cytomegalovirus reactivation during lactation almost equals maternal seroprevalence. Breastfeeding as a source of postnatal cytomegalovirus infection in preterm infants has been underestimated and may be associated with a symptomatic infection.
Comment in Lancet. 2001 Jun 2;357(9270):1800. Lancet. 2001 Jun 2;357(9270):1799-800. PMID 11229670
1993
Cell types infected in human cytomegalovirus placentitis identified by immunohistochemical double staining
Virchows Arch A Pathol Anat Histopathol. 1993;423(4):249-56.
Sinzger C, Müntefering H, Löning T, Stöss H, Plachter B, Jahn G. Source Institut für Klinische und Molekulare Virologie, Universität Erlangen-Nürnberg, Germany.
Abstract
Chronic villitis is almost always present in intrauterine infection with human cytomegalovirus (HCMV). The inflammatory response to this virus has been described in detail. However, little is known about the types of placental cells that may be infected by HCMV and six cases of HCMV placentitis were thus investigated to identify the vulnerable cell types. Immunohistochemical double staining analyses were performed using antibodies to HCMV immediate early antigens and to specific cellular marker proteins. Fixed connective tissue cells could be demonstrated to be the predominantly infected cell type in each placental tissue. Endothelial cells and macrophages were also found to be infected in all six cases, whereas evidence of trophoblast infection was obtained in four cases. It is concluded that release of infectious virus by connective tissue cells, macrophages and endothelial cells may play a critical role in transplacental transmission of HCMV. The findings further suggest that the cytopathic effect of HCMV infection on these cells might be involved in the pathogenesis of intrauterine HCMV disease.
PMID 8236822
CDC Images
http://phil.cdc.gov/phil_images/20030425/14/PHIL_3646_lores.jpg
{kind=link}
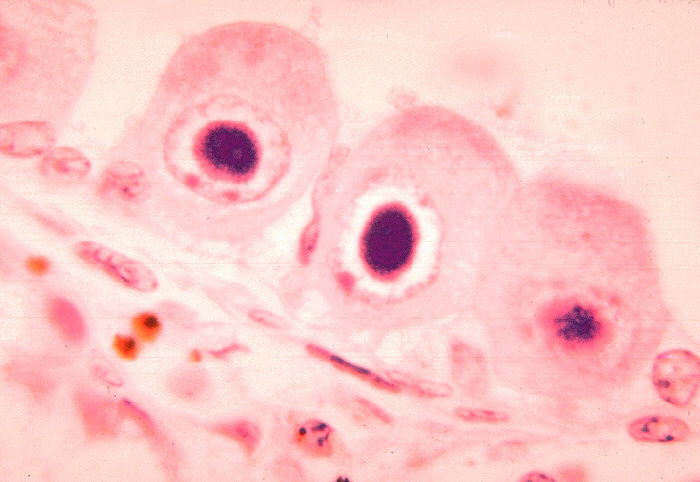
Histopathology of cytomegalovirus infection of brain
http://phil.cdc.gov/PHIL_Images/06011999/00021/09G0041_lores.jpg
{kind=link}
ID#:1160 Description: Histopathology of cytomegalovirus infection of brain.
Histopathology of cytomegalovirus infection of brain capillary endothelial cell.
High Resolution: High resolution download is not available for this image
Content Providers(s):CDC/ Dr. HarasztiCreation Date:1964
Copyright Restrictions:None - This image is in the public domain and thus free of any copyright restrictions. As a matter of courtesy we request that the content provider be credited and notified in any public or private usage of this image.
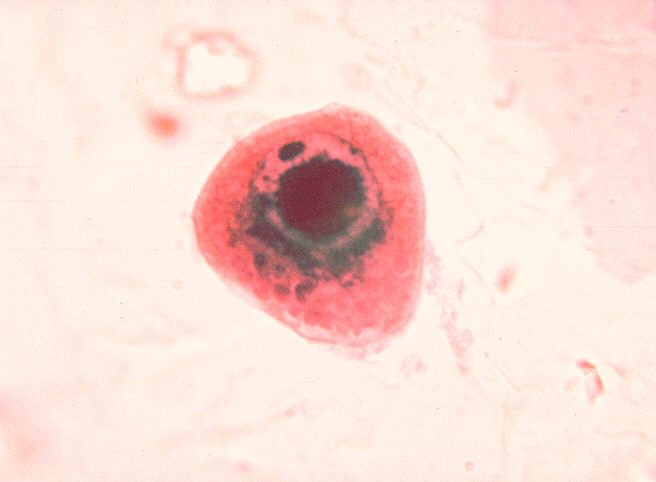
Cytomegalovirus infection of cell in urine
http://phil.cdc.gov/PHIL_Images/06011999/00018/09G0038_lores.jpg
{kind=link}
High Resolution: High resolution download is not available for this image
Content Providers(s):CDC/ Dr. HarasztiCreation Date:1964
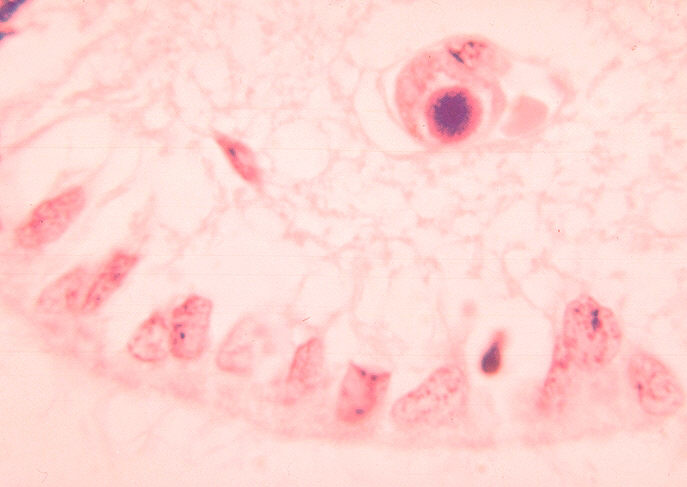
Histopathology of cytomegalovirus infection of kidney
http://phil.cdc.gov/PHIL_Images/06011999/00016/09G0036_lores.jpg
{kind=link}
Description: Histopathology of cytomegalovirus infection of kidney.
High Resolution:High resolution download is not available for this image
Content Providers(s):CDC/ Dr. Haraszti
Creation Date:1964
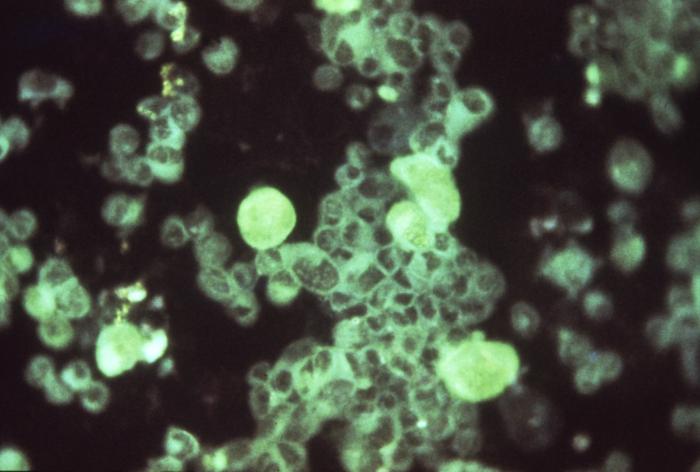
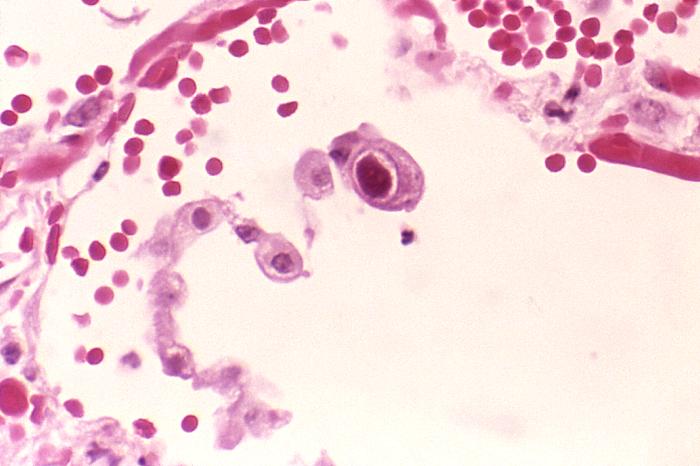
Active cytomegalovirus infection of lung in AIDS
http://phil.cdc.gov/PHIL_Images/958/958_lores.jpg
{kind=link}
Description:Active cytomegalovirus infection of lung in AIDS.
Histopathology of lung shows cytomegalic pneumocyte containing characteristic intranuclear inclusion.
High Resolution:Right click here and select "Save Target As..." for hi-resolution image (6.52 MB)Content Providers(s):CDC/ Dr. Edwin P. Ewing, Jr.Creation Date:1982Copyright Restrictions:None - This image is in the public domain and thus free of any copyright restrictions. As a matter of courtesy we request that the content provider be credited and notified in any public or private usage of this image.
ICD - P35.1 Congenital cytomegalovirus infection
OMIM
LRP6 OMIM 603507
- Structure an extracellular domain that contains LDLR binding repeats and EGF repeats with associated spacer domains containing the YWTD motif; a single transmembrane-spanning domain; and a C-terminal cytoplasmic domain that generally contains at least 1 copy of the NPXY motif
- LRP6 and LRP5 proteins are structurally similar; compared to known LDLR family members, they display a unique pattern of EGF and LDLR repeats in the extracellular domain and have proline-rich motifs but no NPXY motif in the cytoplasmic domain. Northern blot analysis detected a 10-kb human LRP6 transcript in a variety of tissues.
Cyclin D1 OMIM 168461
- regulatory subunit of a holoenzyme that phosphorylates and inactivates the RB protein (RB1; 614041)
- promotes progression through the G1-S phase of the cell cycle in a manner dependent on cyclin-dependent kinases, or CDKs (see CDK2; 116953).
- Hinds et al. (1994) presented evidence that the cyclin D1 gene can function as an oncogene. In cultured cells, a cDNA clone of the CCND1 gene contributed to cell transformation by complementing a defective adenovirus E1A oncogene.
- D-cyclins were critically required for expansion of hematopoietic stem cells.
- cyclin D-deficient fibroblasts proliferated nearly normally, but showed increased requirement for mitogenic stimulation in cell cycle reentry.
PitX2 OMIM 601542
- belongs to the bicoid class of homeodomain transcription factors.
- Kioussi et al. (2002) reported that the transcription factor PITX2 is rapidly induced by the WNT (164820)/DVL (601365)/beta-catenin (116806) pathway and is required for effective cell type-specific proliferation by directly activating specific growth-regulating genes.
- PITX2 then serves as a competence factor required for the temporally ordered and growth factor-dependent recruitment of a series of specific coactivator complexes necessary for cyclin D2 (123833) gene induction.
AXIN1 http://omim.org/entry/603816 AXIS INHIBITOR 1;