Talk:2011 Group Project 6
Group 6: User:z3290841 | User:z3291317 | User:z3291324 | User:z3291423
Plagiarism
--Mark Hill 07:35, 30 September 2011 (EST) Currently all students originally assigned to each group are listed as equal authors/contributors to their project. If you have not contributed the content you had originally agreed to, nor participated in the group work process, then you should contact the course coordinator immediately and either discuss your contribution or request removal from the group author list. Remember that all student online contributions are recorded by date, time and the actual contributed content. A similar email reminder will be sent to all current students.
Please note the Universities Policy regarding Plagiarism
In particular this example:
- "Claiming credit for a proportion of work contributed to a group assessment item that is greater than that actually contributed;"
Academic Misconduct carries penalties. If a student is found guilty of academic misconduct, the penalties include warnings, remedial educative action, being failed in an assignment or excluded from the University for two years.
2011 Projects: Turner Syndrome | DiGeorge Syndrome | Klinefelter's Syndrome | Huntington's Disease | Fragile X Syndrome | Tetralogy of Fallot | Angelman Syndrome | Friedreich's Ataxia | Williams-Beuren Syndrome | Duchenne Muscular Dystrolphy | Cleft Palate and Lip
Group Assessment Criteria
- The key points relating to the topic that your group allocated are clearly described.
- The choice of content, headings and sub-headings, diagrams, tables, graphs show a good understanding of the topic area.
- Figures - there are some good chromosomal and heart repair student images. Historic background is covered. There were otherwise very few research figures and an over reliance on You Tube figures without any additional information.
- Tables - Were very well organised and excellent visual elements on the project page.
- Content is correctly cited and referenced.
- Figures - generally cited correctly, some were missing citation information.
- Too many Medline Plus articles in the reference list and reference 14 appears to have a typo.
- The wiki has an element of teaching at a peer level using the student's own innovative diagrams, tables or figures and/or using interesting examples or explanations.
- Evidence of significant research relating to basic and applied sciences that goes beyond the formal teaching activities.
- Genetics/Aetiology section is well researched.
- Relates the topic and content of the Wiki entry to learning aims of embryology.
- I would have liked to see some more embryology in the project page, there was almost nothing on cardiac and outflow tract development.
- Clearly reflects on editing/feedback from group peers and articulates how the Wiki could be improved (or not) based on peer comments/feedback. Demonstrates an ability to review own work when criticised in an open edited wiki format. Reflects on what was learned from the process of editing a peer's wiki.
- Final project reflects changes based upon earlier peer review comments.
- Discussion page well-summarised the peer review comments.
- Evaluates own performance and that of group peers to give a rounded summary of this wiki process in terms of group effort and achievement.
- The content of the wiki should demonstrate to the reader that your group has researched adequately on this topic and covered the key areas necessary to inform your peers in their learning.
- Develops and edits the wiki entries in accordance with the above guidelines.
Figure Assessment

Z3291324 - Figure relevant to group project. Copyright, Citation and student disclaimer included. This is an interesting figure demonstrating an infant with the disorder.

Z3291317 - Figure relevant to group project. Copyright, Citation and student disclaimer included. I am not keen on the reuse of Wellcome images here and would have liked a research or review article source. Relates to historic background. Could have included some biographical details in the legend.

Z3291317 - Figure relevant to group project. Copyright, Citation and student disclaimer included. Relates to historic background.

Z3291423 - Figure relevant to group project. The single Wikipedia image allowed in the project. Copyright, Citation and student disclaimer included. Would have liked a research or review article source.

Z3291317 - Figure relevant to group project. Copyright, Citation and student disclaimer included. This figure demonstrates anatomical feature associated with the disorder. You have not used an image of someone with the disorder and clubbing. Citation is not correctly formatted as shown below.

Z3290841 - Figure relevant to group project. Meets student drawn figure criteria. Copyright, citation and student disclaimer included. This figure is very useful for understanding chromosomal region affected. You provide further information in the figure legend, demonstrating peer teaching component.

Z3290841 - Figure relevant to group project. Meets student drawn figure criteria. Copyright, citation and student disclaimer included. This figure is very useful for understanding chromosomal region affected. You provide further information in the figure legend, demonstrating peer teaching component.

Z3290841 - Figure relevant to group project. Meets student drawn figure criteria. Copyright, citation and student disclaimer included. This figure is very useful for understanding chromosomal region affected. You provide further information in the figure legend, demonstrating peer teaching component.
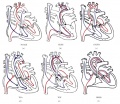
Z3291317 - Figure relevant to group project. Copyright, citation and student disclaimer included. This figure is very useful for understanding blood flow under different conditions. It does though replicate content in the project shown in other figures. You do not provide further information in the figure legend, missing the peer teaching component. The citation is not correctly formatted as required to meet this criteria, as shown below.

Z3291324 - Figure relevant to group project. Copyright, citation and student disclaimer included. This is the third TOF infant image in the project and none of them include any additional information as to what they are showing and how it relates to the associated content, lacks peer teaching. All these images have similar sources.






z3291423 - Figure relevant to group project. Meets student drawn figure criteria. Copyright, Citation and student disclaimer included. You provide further information in the figure legend, demonstrating peer teaching component. This could have been improved by labelling your drawing and perhaps you should have linked the related images together.

z3291423 - Figure relevant to group project. Meets student drawn figure criteria. Copyright, Citation and student disclaimer included. You provide further information in the figure legend, demonstrating peer teaching component. This could have been improved by labelling your drawing and perhaps you should have linked the related images together.

z3291423 - Figure relevant to group project. Meets student drawn figure criteria. Copyright, Citation and student disclaimer included. You provide further information in the figure legend, demonstrating peer teaching component. This could have been improved by labelling your drawing and perhaps you should have linked the related images together.

z3291423 - Figure relevant to group project. Meets student drawn figure criteria. Copyright, Citation and student disclaimer included. You provide further information in the figure legend, demonstrating peer teaching component. This could have been improved by labelling your drawing and perhaps you should have linked the related images together.

Z3291324 - Figure relevant to group project. Copyright, citation and student disclaimer included. This image includes no additional information as to what is shown and how it relates to the associated content, lacks peer teaching. All these images have similar sources.

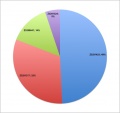
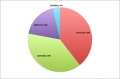
z3291423 - Figure relevant to group project. Copyright and student disclaimer included. Significantly you have not identified the source (citation) for your data in the graph. This is a major shortcoming to what would have been a good assets to the project.
















Slowly as in bit by bit, which is now done, look at it and see if you still don't understand what it's talking about. I tried to clarify some of the things that I think needs to be clarified. Also I don't know how to put a title on
what do you mean you'll slowly change it? its due in 12 hrs! (z3291324)
Ok this is going to be the new outline of the genetics part, I'll slowly change it here in the discussion so things will be added along the way, also Z3291324 the comments said table, but I'm not planning to put all my info in a table, just the gene profile, the rest will be in text form cause I don't think the information will come across better if I put all of it in a table.
Genetics/Aetiology
The genetic etiology of Tetralogy of Fallot (TOF) is still currently unknown and being researched. Even though this is the case, most of the studies done on the disorder have agreed that TOF normally occurs with other developmental disorders, like DiGeorge syndrome, and that the disorder may be caused by multiple mutations in a person’s genome. Here are some of the current suspected genetic mutations that leads to the congenital disease Tetralogy of Fallot.
| Features | 22q11.21 | 5q34 | 20p12.1 - p11.23 |
| Chromosome # | 22 [1] | 5 [2] | 20 [3] |
| Chromosome arm | q (long arm) | q (long arm) | p (short arm) |
| Position | 11.21 | 34 | 12.1 to 11.23 |
| # of base pair | 26,890 | 3,208 | 36,362 |
| Gene Affected | TBX1 | NKX2-5 | JAG1 |
22q11.21
Studies have shown 74% of patients with 22q11.2 microdeletions have Congenital Heart Defect, and out of these 22% have Tetralogy of Fallot (TOF).[4]. This is why mutation in this region of the chromosome is an important consideration for the genetic aetiology of TOF.
This region of chromosome 22 contains the gene for T-box 1 transcription factor (TBX1). As a transcription factor, it regulates the expression of genes by binding to the regulatory region of the DNA and promote/inhibit the transcription of particular genes [5]. Although the genes regulated by this particular transcription factor is still being researched, it has been discovered that mutation in the gene can lead to the development of TOF [6] [7]
The most common genetic mutation of this gene that results in TOF is a microdeletion of 3 or 1.5 Mb of 22q11.2 region on chromosome 22 [7]. The result of this microdeletion is a haploinsufficient gene. This is where there is only a single copy of the gene in one allele, which clinically leads to an abnormal functioning of the protein because a single copy of the gene is incapable of producing enough protein that will allow normal function. [8]
Although microdeletion is the most common mutation in the TBX1 gene that results to TOF, there are other mutational variants that have been observed that resulted in TOF. This variant involve a 30-bp duplication in exon 9c, a region in the TBX1 gene. This leads to the production of non-functioning TBX1 protein because the insertion of the duplicate leads to the expansion of the polyalanine tract of the gene, resulting to a non-functioning TBX1 protein. The proteins produced aggregates within the cytoplasm, leading to decrease in transcription of TBX1 gene, since this gene is dose-dependent, which means that transcription cease as soon as there is enough TBX1 protein. Since the TBX1 proteins are non-functioning transcription of genes that the TBX1 protein is responsible for is not controlled.[7]
Mutation of the TBX1 gene may also lead to other phenotype, which includes:
- DiGeorge Syndrome
- Velocardiofacial Syndrome
- Conotruncal anomaly face syndrome
5q34
Studies have shown that at least 4% of TOF patients have NKX2-5 mutation. This is why the mutation in this gene is considered in the development of TOF. [9]
This gene encodes the NK2 homeobox 5 transcription factor (NKX2-5 protein). NKX2-5 protein is essential in tissue differentiation and temporal and spatial patterns of development in cardiac tissue. [10]. This means the protein regulates the genes responsible for the formation of the chambers of the heart. This is because studies have shown that the NKX2-5 protein is involved in the development of atrial, ventricular and conotruncal septation, AV conduction and AV valve formation. [11] Atrial and ventricular septation is the formation of the walls that separate the heart into four chambers, while conotruncal septation is the formation of the two great vessels (Aorta and Pulmonary artery) that forms the outflow tracts of the heart.
There are 4 known substitution mutation of the NKX2-5 gene in TOF patients, although one of the mutations has been found to be present in non-TOF patients. [9] This includes:
- G to C substitution at base pair 21 = glutamic acid to glutamine amino acid substitution
- C to T substitution at base pair 216 = arginine to cysteine amino acid substitution
- C to T substitution at base pair 219 = alanine to valine amino acid substitution
Mutation of the NKX2-5 gene may also lead to other phenotype, which includes:
- Hypothyroidism
- Congenital non-goitrous
- Atrial septal defect with atrioventricular conduction defects
20p12.1-p11.23
The typical clinical presentation of mutation in this gene is a disease called Alagille Syndrome (AGS) that have some clinical overlap with that of TOF, which are mainly right heart abnormalities.[12] This makes mutation in this gene of special interest when it comes to TOF
The gene is about 36 kb with 26 exons, which are the coding regions of the DNA,[13] and expresses the gene Jagged-1 protein (JAG1 protein), which is a ligand of the Notch receptor [14]. This means that cells/tissues containing the JAG 1 protein are able to communicate with cells/tissues that contains the Notch receptor on its surface. JAG1 Gene is highly expressed in developing mammalian heart, thus JAG1 proteins are present on cardiac cell membranes [15]. With the Notch receptor present on adjacent cells, JAG1 protein is able to communicate with adjacent cells via intercellular signaling. This is because the bond between the JAG1 protein and the Notch receptor leads to the release of the receptor’s intracellular region from the membrane. This part is transported into the nucleus activating transcription factors, which in turn regulates the transcription of genes that will lead to cellular differentiation and morphogenesis.[14]
There is a missesnse mutation of the JAG1 gene identified at the 821st base pair. This is a G to A substitution, resulting in glycine to aspartic acid substitution. This may lead to the formation of cysteine residues that results in the formation of abnormal protein because its structure and stability has been compromised.[16] There are 2 types of proteins resulting from the mutation of the allele, a protein that functions abnormally and a protein that functions normally. The abnormal functioning protein is produced at higher temperature[17]:
- Abnormal JAG1 protein = retained intracellularly and not transported to cell surface
- Normal JAG1 protein = retains function as a ligand to Notch receptor
Mutation of the JAG1 gene may also lead to other phenotype, which includes:
- Alagille Syndrome
- Deafness
- Congenital heart defects
- Posterior embryotoxin
what does everyone think?
http://www.youtube.com/watch?v=_ErZG43lAh8&feature=related at 51 seconds (for physical examination pathophys table) --z3291324 11:24, 11 October 2011 (EST)
actually, this one is probably better http://www.youtube.com/watch?v=3bN7QltwfB0&feature=related at 5 seconds
does anyone know how to properly reference a book? i used robbins basic pathology for some of the pathophys section but im not sure how to reference it--z3291324 11:01, 11 October 2011 (EST)
hey rommel, are you putting these pics on the page? also, can you check out the feedback for your section...did other groups recommend a table for the genetics..or getting rid of the dot points? pics look good btw --z3291324 10:07, 11 October 2011 (EST)
Finally the last image for genetics. That should be it for now I'm really tired. I'll update and clear up the text on the page tomorrow, hopefully you made a comment on the timages and table by then, if not that's fine, but I won't put it in the page until I get a general consensus. --z3290841 19:50, 6 October 2011 (EST)

Here I have another image for the next gene --z3290841 17:51, 6 October 2011 (EST)

Ok guys here you go I changed the image again, hopefully it's better if not tell me asap so I can change it --z3290841 16:36, 6 October 2011 (EST)

Hey I changed the table for genetics up tell me what you think. If it's good for you guys I'll be putting it in the page. --z3290841 16:02, 6 October 2011 (EST)
Just put up some internal links on the page. feel free to add or remove what you thin is necessary. these are th eones that i just put up Cardiovascular development abnormalities http://embryology.med.unsw.edu.au/Notes/heart2.htm#Fallot
Advanced cardiac embryology http://embryology.med.unsw.edu.au/embryology/index.php?title=Advanced_Cardiac_Embryology
Cardiovascular system development http://embryology.med.unsw.edu.au/embryology/index.php?title=Cardiovascular_System_Development
Cardiovascular development lecture http://embryology.med.unsw.edu.au/embryology/index.php?title=2009_Lecture_21 --z3291324 11:35, 6 October 2011 (EST)
Hey this is just a trial run for the table I am doing for the genetics part of our page --z3290841 11:17, 6 October 2011 (EST)
| Features | 22q11.21 | 5q34 | 20p12.1 - p11.23 |
| Chromosome # | 22 | 5 | 20 |
| Chromosome arm | q (long arm) | q (long arm) | p (short arm) |
| Position | 11.21 | 34 | 12.1 to 11.23 |
| # of base pair | 26,890 | 3,208 | 36,362 |
| Gene Affected | TBX1 | NKX2-5 | JAG1 |
Hey Rom and jaq, thanks for fixing up the table! :-{) --Z3291317 10:42, 6 October 2011 (EST)
Hey I editted the one that jaqui editted
| Race | Incidence of TOF malformation (per 10,000) |
| Whites | 2.85 |
| Hispanics | 2.31 |
| Asians | 2.83 |
| Blacks | 3.81 |
| Other | 3.80 |
Hey guys, I'm currently editing through my sections and adding new stuff, also check the image i placed in the diagnostic techniques part under MRI, i hope it fits properly! also rom the diagram looks a bit complicated, could you simplify it and explain what you are trying to show? thanks --Jasjit Walia 00:53, 6 October 2011 (EST)
test:
| Race | Incidence of TOF malformation (per 10,000) |
| Whites | 2.85 |
| Hispanics | 2.31 |
| Asians | 2.83 |
| Blacks | 3.81 |
| Other | 3.80 |
Hey People i re tweaked the table to rom's preferences, and rom you slightly jumbled the structure of the entire table, so i fixed it. Also, in your diagram, it was a bit hard trying to understand the part you try to demonstrate the zone being deleted. Speak to you about it later. Regards --Z3291317 22:50, 5 October 2011 (EST)
Hey guys I just fixed up bits and pieces of the dates on the timeline. Jaqui the table looks really good, and uhm I think I prefer the coplour of jaqui's table. The red looks a but eh to me. By the way thanks furkan for fixing the tables up now all it needs is the reference and I think we can start to get rid of some of the things in the history. Also I made a diagram for genetics so have a geez and tell me things that you like and don't like and/or hate. Also Jaqui I found a yoputube video for your MRI section of the heart I really don't understand what it's showing but I think it'll be really good if we can imbed it and keep it on loop, here's the link http://www.youtube.com/watch?v=UZk9ForCPyE --z3290841 16:30, 5 October 2011 (EST)

just testing out jaz's table too. i think i might have accidentally done this one in blue too --z3291324 21:27, 3 October 2011 (EST)
| Type of shunt | Descriptions | Reasons for it not being used |
| Pott’s shunt | This shunt is a connection that is established between the defending portion of the aorta (on the left side of chest) to the left branch of the pulmonary artery. [18] | The shunt has a tendency to increase the pulmonary blood flow, pulmonary hypertension, causes blood flow to be preferential to one of the lungs, the shunt causes kinking in the pulmonary artery and it is also very hard to close when complete repair is undertaken [19] |
| Waterston shunt | This shunt was placed between the back of the aorta, to the right branch of the pulmonary. [20] | This shunt’s use is more suited to those with pulmonary artery stenosis and also the procedure is quite difficult to perform. It causes excessive pulmonary blood flow and hypertension and congestive cardiac failure has been found in 20% of patients that have with the Waterston or Pott's shunt [21] |
| Glenn shunt | The superior vena cava is anastomosed via a shunt to the right pulmonary artery (the classic Glenn shunt). The modified glenn shunt is for, the superior vena cava to the right branch of the pulmonary artery, which is till connected to to the main pulmonary artery.[22] | This procedure is very complicated and difficult to perform, also complete repair becomes a laborious task. [23] |
for the intro, did we decide to make it like a summary of whats to come (so include a bit of epidemiology, symptoms, treatment etc)??--z3291324 21:16, 3 October 2011 (EST)
| Diagnostic technique | How the technique works | Presentation in a TOF patient | Image |
| Physical examination | TOF is often diagnosed during fetal life by echocardiography.[24]
If TOF is not detected during fetal life, certain signs and symptoms at birth may alert the need for further investigation. |
Signs and symptoms include mild to moderate cyanosis, which worsens when the baby cries, difficulty feeding and difficulty gaining weight. However, TOF often goes undiagnosed until adult life. Most adult patients will appear normal, however, some may present with cyanosis and clubbing of the fingers. The jugular venous pressure is usually normally (raised jugular venous pressure often indicates right ventricular failure). If the aorta is pushed to the right (so it is continuous with both the left and right ventricle), a lift below the right sternoclavicular joint may be noted. [25] | Insert physical examination image |
| Heart murmurs | Heart murmurs are sounds caused by the turbulent flow of blood. They are heard using a stethoscope. They are often the result of problems including valvular stenosis (narrowing of valves), valvular regurgitation (leakage of valves due to incomplete closure) or defects in the heart wall allowing blood to flow in unusual directions. | Examination of the heart of a patient with TOF may reveal a loud second heart sound (produced by the closure of the pulmonary valve). A harsh systolic ejection murmur may be heard and a palpable thrill may be felt along the left sternal border. These sounds occur because the pulmonary outflow tract is obstructed. Although this murmur is often present, sometimes it may be short or difficult to hear and is often missed on physical examination. A pansystolic (occurring throughout the whole of systole) murmur may also be heard. This type of murmur occurs due to the ventricular septal defect between the left and right ventricles. The increased pressure in the left ventricle forces blood back into the right ventricle, causing a murmur, which lasts the whole of systole (contraction phase). [26] | Insert heart murmur image |
| Electrocardiogram | Once TOF is suspected, electrocardiogram and chest radiographs are performed. Electrocardiography is used to assess the electrical activity of the heart. The electrical activity is detected by electrodes, which are placed on the skin of the patient and recorded by an external device. | The electrocardiogram is extremely important in detecting a right bundle branch block (a block in the electrical conducting system of the heart), which is common in patients with TOF. An electrocardiogram will also reveal a heart that is deviated slightly to the right and an enlarged right ventricle due to the ventricular hypertrophy.[25] | Insert electrocardiogram image here |
| align="Chest radiograph | A chest radiograph (or chest x-ray) uses ionising radiation to develop an image of the patient’s chest. It is used to diagnose many conditions including conditions of the thorax and structures within the thoracic cavity including the heart, lungs and major blood vessels entering and leaving the heart. Chest radiographs are often used to screen for certain diseases but further tests are required for a definitive diagnosis. | In a patient with TOF, a chest radiograph will demonstrate a prominent right ventricular shadow, giving the heart a boot-like appearance, which is typical of patients with TOF. The right ventricular hypertrophy causes the apex of the right ventricle to rise on top of the relatively unfilled left ventricle, giving the heart its boot-shaped appearance on examination. [27] The radiograph will also show a right-sided aorta in approximately one-quarter of patients.[25] | 
|
| Echocardiogram | An echocardiogram (also called a cardiac ultrasound) is performed to confirm the above findings. Echocardiography uses ultrasound to produce two-dimensional (and now also three-dimensional) images of the heart. It assesses cardiac tissue, valve function, the velocity of blood flow and any abnormal communications within the heart. | The echocardiogram identifies important abnormalities of the heart including obstruction of the pulmonary outflow tract, the size of the pulmonary arteries, the degree of aortic override and the size of the defect in the interventricular septum. [27] | File:Echo.jpg |
| Magnetic resonance imaging | Magnetic resonance imaging (MRI) is evolving as the most important technique for evaluating the size and functioning of the right ventricle. An MRI machine uses a magnetic field to produce a detailed image of the scanned area of the body. It is especially useful in viewing soft tissues as it provides greater contrast than techniques such as x-ray. | MRI’s are important in assessing pulmonary valve competence and the severity of regurgitation (the amount of blood that flows back into the right ventricle due to the incomplete closure of the pulmonary valves) in patients with TOF. It can measure the volume and mass of the right and left ventricles and can assess the degree of pulmonary outflow tract obstruction. Finally, MRIs are important in measuring the degree of ventricular septal defect.[25] | Insert MRI image here |
--z3291324 20:29, 3 October 2011 (EST)
Hey Jaq, here is the proposed final table without the references (will be added later). When you have the top part dark red, the reader will cognitively look at the lighter colour as red as the brain will be using the darker colour as a comparative standard (i know its a bit far fetched explanation), i think it will be alright having the colours like this... Look at the new table below, i had fixed some dates up rommel thought were together as it appeared like that in the text, so fiddled with them a bit and added some important dates i should had from before, so this new info would only be found in the table and not in the text, what you guys think?....--Z3291317 19:44, 3 October 2011 (EST)
| Year | Milestones |
| 1628 | William Harvey published his work De Motu Cordis which portrayed a groundbreaking understanding that the two criculatory systems, pulmonary and systemic, and independant of each other. |
| 1671 | Stenson anatomically described Tetralogy of Fallot |
| 1784 | William Hunter gave a precise description of the anatomy of Tetralogy of Fallot. |
| 1847 | Chevers acknowledged the absence of pulmonary valve in Tetralogy of Fallot hearts. |
| 1850s | Peacock was a pioneer in using a stethoscope to discover a cardiac murmur with a heart with pulmonary stenosis. |
| 1888 | Fallot destroyed the idea that cyanosis had always occured due to inability of the foramen ovale to close. Also, he was the one to use the term tetralogie, and furthermore acknowledged that there was no therapeutic treatments for patients of TOF during his time. |
| 1888 | Etienne-Louis Fallot specified and advanced the description of Tetralogy of Fallot’s heart anatomy and its resulting physiology |
| 1924 | Maude Abbott coined the term “Tetralogy of Fallot” |
| 1936 | Abbot demonstrated the Chest X-ray, 3-lead electrocardiogram and circulatory and auscilatory diagrams that were produced from a Tetralogy of Fallot heart. |
| 1938 | Gross and Hubbard closed off the patent dusctus arteriosus in a girl who was aged 7 |
| 1943 | Helen Taussig using fluoroscope determined that TOF patients suffer cyanosis because of decreased blood flow to the pulmonary circulation. She then proposed the benefits of an “artificial ductus” in TOF neonates, as she believed the closing of the patent ductus arteriosis lead to babies having cyanosis and cyanotic spells. |
| 1945 | Blalock and Taussig explained the ‘systemic artery-to-pulmonary artery shunt’ |
| 1950 | Beginning of the rise of open heart surgery |
| 1954 | Varco and Lilehei repaired a TOF heart whilst doing an open-heart surgery |
| 1950-70 | Realisation of variance in the anatomy of TOF. This became the period of success for intracardiac surgeries to infant. |
| mid 1970s | Advancements in Infant surgery, introduction of prostaglandin therapy and rise in electrocardiography signficantly affected the patients with Tetralogy of Fallot |
| 1990s | Dr Taussig hypothesised that congenital cardiac defects had arisen from the expression of genetic defects found in infants. |
hey furkan, thanks heaps for trying with the table. what do you guys think? maybe our colour scheme would be better as blue and grey. do you think the red looks a bit pink?? --z3291324 19:34, 3 October 2011 (EST)
Hey People i took on Jaq ideas and reformatted the table Rom made (thanks rom!). Its still a work in progress as im going to add many more dates into it so it can accompany the text in the history without having to remove the text. Man coding is annoying lol... regards --Z3291317 18:28, 3 October 2011 (EST)
| Year | Milestones |
| 1671 | Stenson anatomically described Tetralogy of Fallot |
| 1784 | William Hunter gave a precise description of the anatomy of Tetralogy of Fallot.
Etienne-Louis Fallot specified and advanced the description of Tetralogy of Fallot’s heart anatomy and its resulting physiology |
| 1924 | Maude Abbott coined the term “Tetralogy of Fallot” |
| 1938 | Gross and Hubbard closed off the patent ductus arteriosus in a girl who was aged 7 |
| 1943 | Helen Taussig using fluoroscope determined that TOF patients suffer cyanosis because of decreased blood flow to the pulmonary circulation. She then proposed the benefits of an “artificial ductus” in TOF neonates, as she believed the closing of the patent ductus arteriosis lead to babies having cyanosis and cyanotic spells. |
| 1945 | Blalock and Taussig explained the ‘systemic artery-to-pulmonary artery shunt’ |
| 1945 | Blalock and Taussig explained the ‘systemic artery-to-pulmonary artery shunt’ |
| 1950 | rise of open heart surgery |
| 1954 | Varco and Lilehei repaired a TOF heart whilst doing an open-heart surgery |
| 1950-70 | Realisation of variance in the anatomy of TOF. This became the period of success for intracardiac surgeries to infant.
Dr Taussig hypothesised that congenital cardiac defects had arisen from the expression of genetic defects found in infants. |
hey rommel! love the table! but are we going to have the table as well as the text? any chance you could make the blue a ligth red..but keep it really similar ie the darker red at the top with the light red and white in the table (so it matches the rest of the colour scheme)--z3291324 17:34, 3 October 2011 (EST)
Hey this is my attempt at making the timeline for the history section. I haven't put in any references cause I just want to check on the things that I put in it if you guys would agree. Feel free to change it, delete some of it and add some stuff in it. Also I just copied the table template from some other group so yeah :)
| Year | Milestones |
| 1671 | Stenson anatomically described Tetralogy of Fallot |
| 1784 | William Hunter gave a precise description of the anatomy of Tetralogy of Fallot.
Etienne-Louis Fallot specified and advanced the description of Tetralogy of Fallot’s heart anatomy and its resulting physiology |
| 1924 | Maude Abbott coined the term “Tetralogy of Fallot” |
| 1938 | Gross and Hubbard closed off the patent dusctus arteriosus in a girl who was aged 7 |
| 1943 | Helen Taussig using fluoroscope determined that TOF patients suffer cyanosis because of decreased blood flow to the pulmonary circulation. She then proposed the benefits of an “artificial ductus” in TOF neonates, as she believed the closing of the patent ductus arteriosis lead to babies having cyanosis and cyanotic spells. |
| 1945 | Blalock and Taussig explained the ‘systemic artery-to-pulmonary artery shunt’ |
| 1945 | Blalock and Taussig explained the ‘systemic artery-to-pulmonary artery shunt’ |
| 1950 | rise of open heart surgery |
| 1954 | Varco and Lilehei repaired a TOF heart whilst doing an open-heart surgery |
| 1950-70 | Realisation of variance in the anatomy of TOF. This became the period of success for intracardiac surgeries to infant.
Dr Taussig hypothesised that congenital cardiac defects had arisen from the expression of genetic defects found in infants. |
Summary of the Comments made on our draft project
- Intro = add picture and basically fix it up - History = put the quote in the box, add a timeline and less word, put the dates in bold - Epidemiology = more detail and work - Signs and symptoms = better ghlossary, change the size of subheadings, explain further, picture for each signs and symptoms - Genetics = explain better, i.e. the technical details, add a table - Pathophysiology = reformat - Prognosis = add a pie chart - Future Directions = add articles - Glossary - make some links
here youi go guys, sorry it's a bit late --z3290841 09:44, 3 October 2011 (EST)
hey fru, okay. maybe we should go for alternating colours then. ill try out a couple tonight. also, im just pasting the intro here on the discussion page because im going to edit it either tonight or tomorrow --z3291324 21:24, 2 October 2011 (EST) I like the grey and red border you put around the quote. maybe we can make our colour scheme gray and red. can you try and put that same colour grey into every second box of the diagnostic table. i tried to put in red and grey but for some reason it keeps turning different shades of green!--z3291324 21:46, 2 October 2011 (EST)
Tetralogy of Fallot (TOF), named after Etienne Fallot is a disease that occurs in 3 in every 10000 live births and constitutes to roughly 7%-10% of all cardiac congenital defects today.
TOF is believed to occur due to genetic mutation, which is thought to impact on the development upon the neonate heart. Furthermore, it is believed that the genetic aetiology of TOF is a mutation in one of chromosomes 5,20 and 25. These genetic mutations contribute to the four characteristic defects, in the heart of a patient having TOF:
Pulmonary stenosis
Overiding aorta
Ventricular septal defect
Right ventricular hypertrophy
TOF patients are nicknamed 'Blue babies' because the lack of oxygen being supplied to the body. Some common occurrences for TOF patients include, Infants turning blue when crying, children collapsing due to tet spells during exercise and fatigue.
Etienne Fallot, Helen Taussig and Alfred Blalock have significantly contributed to the scientific community's understanding of the cardiac anomaly and ways to treat it. Today, surgery remains the only way to treat the anomaly, however palliative care and medical treatment is available.
Due to technology advancements, doctors are able to detect TOF more accurately and treat patients quicker, allowing an increase in survival rate and a favourable long term prognosis.
Whilst a lot of knowledge is available on this disease, future directions include developing durable and efficient surgical procedures, shunts and valves.
REPLY 2: You can have the old format, ot have the red and white osscilating colours for the rows, or have both with the borders not that prominent and have the colour changes in the table. Ye i relised your pic was put down, well discuss it at next lab. hows finding other pics going?--Z3291317 10:22, 2 October 2011 (EST)
Do you think the diagnostic table would look better in paragraphs? I think the table is a bit big?--z3291324 13:31, 1 October 2011 (EST) REPLY: I reckon it will be okmto put into the table if you insert outlines into the table. If you put it into paragraphs, there is gonna be alot of writing in a section that, i think, the reader wouldnt want to read. It your call, see what the other 2 boys think --Z3291317 22:24, 1 October 2011 (EST) thanks fru, do you mean change it back to the old table format? or maybe we could put a light red background for every second row. (i tried doing that but i couldnt find a colour that was light enough and wasnt too pink). also, one of my pics got taken down so i wont upload any til the lab next thursday. --z3291324 08:40, 2 October 2011 (EST)
hey guys, ive fixed up the glossary up to treatment (but i havent done the genetics part). the terms in glossary are in bold at the moment but anyone feel free to change them to a link or anything else.--z3291324 12:48, 1 October 2011 (EST)
Page Edits 30 Sep
Project Page

All Groups (1-11) Project
Discussion Page
All Groups (1-11) Discussion




{kind=link}
Test table --z3291324 19:02, 30 September 2011 (EST)
| Diagnostic technique | How it works | Presentation in a TOF patient | Image |
| Physical examination | TOF is often diagnosed during fetal life by echocardiography (Apitz, Webb, & Redington, 2009). If TOF is not detected during fetal life, certain signs and symptoms at birth may alert the need for further investigation. | Signs and symptoms include mild to moderate cyanosis, which worsens when the baby cries, difficulty feeding and difficulty gaining weight. However, TOF often goes undiagnosed until adult life. Most adult patients will appear normal, however, some may present with cyanosis and clubbing of the fingers. The jugular venous pressure is usually normally (raised jugular venous pressure often indicates right ventricular failure). If the aorta is pushed to the right (so it is continuous with both the left and right ventricle), a lift below the right sternoclavicular joint may be noted. (Somerville, 1993) | Insert physical examination image |
| Heart murmurs | Heart murmurs are sounds caused by the turbulent flow of blood. They are heard using a stethoscope. They are often the result of problems including valvular stenosis (narrowing of valves), valvular regurgitation (leakage of valves due to incomplete closure) or defects in the heart wall allowing blood to flow in unusual directions. | Examination of the heart of a patient with TOF may reveal a loud second heart sound (produced by the closure of the pulmonary valve). A harsh systolic ejection murmur may be heard and a palpable thrill may be felt along the left sternal border. These sounds occur because the pulmonary outflow tract is obstructed. Although this murmur is often present, sometimes it may be short or difficult to hear and is often missed on physical examination. A pansystolic (occurring throughout the whole of systole) murmur may also be heard. This type of murmur occurs due to the ventricular septal defect between the left and right ventricles. The increased pressure in the left ventricle forces blood back into the right ventricle, causing a murmur, which lasts the whole of systole (contraction phase). http://ccjm.org/content/77/11/821.full | Insert heart murmur image |
| Electrocardiogram | Once TOF is suspected, electrocardiogram and chest radiographs are performed. Electrocardiography is used to assess the electrical activity of the heart. The electrical activity is detected by electrodes, which are placed on the skin of the patient and recorded by an external device. | The electrocardiogram is extremely important in detecting a right bundle branch block (a block in the electrical conducting system of the heart), which is common in patients with TOF. An electrocardiogram will also reveal a heart that is deviated slightly to the right and an enlarged right ventricle due to the ventricular hypertrophy.(Somerville, 1993) | Insert electrocardiogram image here |
| Chest radiograph | A chest radiograph (or chest x-ray) uses ionising radiation to develop an image of the patient’s chest. It is used to diagnoses many conditions including the thorax and structures within the thoracic cavity including the heart, lungs and major blood vessels entering and leaving the heart. Chest radiographs are often used to screen for certain diseases but further tests are required for a definitive diagnosis. | In a patient with TOF, a chest radiograph will demonstrate a prominent right ventricular shadow, giving the heart a boot-like appearance, which is typical of patients with TOF. The right ventricular hypertrophy causes the apex of the right ventricle to rise on top of the relatively unfilled left ventricle, giving the heart its boot-shaped appearance on examination. (Bailliard & Anderson, 2009) The radiograph will also show a right-sided aorta in approximately one-quarter of patients. (Somerville, 1993) |
|
| Echocardiogram | An echocardiogram (also called a cardiac ultrasound) is performed to confirm the above findings. Echocardiography uses ultrasound to produce two-dimensional (and now also three-dimensional) images of the heart. It assesses cardiac tissue, valve function, the velocity of blood flow and any abnormal communications within the heart. | The echocardiogram identifies important abnormalities of the heart including obstruction of the pulmonary outflow tract, the size of the pulmonary arteries, the degree of aortic override and the size of the defect in the interventricular septum. (Bailliard & Anderson, 2009) | File:Echo.jpg |
| Magnetic resonance imaging | Magnetic resonance imaging (MRI) is evolving as the most important technique for evaluating the size and functioning of the right ventricle. An MRI machine uses a magnetic field to produce a detailed image of the scanned area of the body. It is especially useful in viewing soft tissues as it provides greater contrast than techniques such as x-ray. | MRI’s are important in assessing pulmonary valve competence and the severity of regurgitation (the amount of blood that flows back into the right ventricle due to the incomplete closure of the pulmonary valves) in patients with TOF. It can measure the volume and mass of the right and left ventricles and can assess the degree of pulmonary outflow tract obstruction. Finally, MRIs are important in measuring the degree of ventricular septal defect. (Somerville, 1993) | Insert MRI image here |
Test: <object width="480" height="360"><param name="movie" value="http://www.youtube.com/v/PRxN6migkW8?version=3&hl=en_US"></param><param name="allowFullScreen" value="true"></param><param name="allowscriptaccess" value="always"></param><embed src="http://www.youtube.com/v/PRxN6migkW8?version=3&hl=en_US" type="application/x-shockwave-flash" width="480" height="360" allowscriptaccess="always" allowfullscreen="true"></embed></object>
Peer Review
Group 6: Nice introduction. The length is right. Perhaps what is missing is general image to make it less wordy. History seems to be well researched but if you can make into a timeline would be great. Nice layout in the Signs and symptoms Genetics/Aetiology. You may want to consider more images since the section are quite big. Also, add a description, copyright and reference for the images in the genetics and aetiology. Well done in the table of diagnostic Tests. Do not forget to add the images. In the Treatment and management, you may need to add some shading in the table because the lines of the table are not obvious and Prognosis needs more referencing. In the future Directions, you may consider deleting the in text referencing. Finally, some of references need to re-format.
Well Done. --z3284061 11:53, 29 September 2011 (EST)
Group 6
- The intro needs some referencing
- An image might be good in the introduction
- Histroy section is good. A timeline might be helpful
- Epidemiology section needs more information
- Good table in Diagnostic Tests, however, images are missing
- An image would be good in either Prognosis or Future directions to break up the text
- Good flow to the project
- Good student drawn picture
- Glossary needs to be completed
- Double referencing needs to be fixed
--z3292953 11:08, 29 September 2011 (EST)
Tetralogy of Fallot (Group 6) Peer Review:
Introduction: Good content, however possibly revise grammar and structure of some sentences. Also, it would engage the reader more if they could visualize what you are saying through an image.
History: This section has the relevant information, however try using a different format to represent your ideas, such as a timeline or a table? Fallot image lacks a student template and images need to have the correct referencing format. Maybe too wordy for history? Try to make it a bit more succinct.
Epidemiology: Slightly short. Can you elaborate?
Signs and Symptoms: Good use of links to redirect the reader to more information. Image is good, however I think you could maybe put more images in this section to break up the text. Try revising some of the sentence structure. Otherwise, the information in this section is good.
Genetics/ Aetiology: This section is good, however some things need to be further explained. Example: “Gene affected = NKX2-5” – could you elaborate on this? Images are good and relevant.
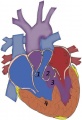
Pathophysiology and Abnormalities: This section is impressive! Images are excellent and help the reader understand what you are describing in words. The fetal blood flow image lacks a student template. This section needs to be referenced.
Diagnostic tests: Obviously a lot of information here. I am sure I do not need to tell you that this section is incomplete. Images need to be added. I am slightly confused as to why there is a reference directly below the table? Couldn’t this be added to the reference list with the other references?
Treatment/ Management: This section is good. Image needs a student template, but otherwise well done.
Prognosis: Good information. However, surely you did not gather all of this information from the one reference? Also, maybe a picture would help to break up the information.
Future Directions: Good idea. This section is good.
Glossary: Could be expanded.
Overall, the page is coming along well. Nice work and good luck with the editing process! --z3290808 10:44, 29 September 2011 (EST)
Tetralogy of Fallot – Group 6
- Introduction is rather disjunct. No images here also. Also no referencing.
- History looks well detailed, however other groups have used a timeline or table to summarize this information. I think this would help it flow better and be more succinct.
- Epidemiology needs some work. No images and the text does not really explain the epidemiology well.
- Signs and symptoms looks well written, however maybe some more images here could be useful. Also a table might better summarize this information. The image used could be better explained also.
- Other sections look well structured and highly detailed. Looks like a lot of work and research has been put in. Images are well explained and correctly referenced.
- The future directions heading could also include some more detail current research projects as well as some comment on the overall direction that this future direction is taking.
- Glossary needs a lot of work to be complete.
--Z3288196 10:44, 29 September 2011 (EST)
Peer Review The first striking feature is the long block of text from the start. You need to break this up with more tables. Your Genetics/Aetiology section could be laid out more simply. A table with columns for the Gene, gene profile and then description. In Pathophysiology, you already have the numbered list. Don't put the numbers next description and format this so that each of the following:
Pulmonary stenosis Overriding aorta Ventricular septal defect Right ventricular hypertrophy
are a subheading in your contents.
In treatment and managment, I would suggest that you colour each row of the table differently. I agree that tables without borders look better. However, if is hard to see which bit of information is associated with Pott's shunt, Watersons shunt etc.
Lastly: only 41 references? I would have expected a lot more. The average number for the other groups is in the 125-150 region. You might want to do a bit more research.
--Ziggy Harrison-Tikisci 10:41, 29 September 2011 (EST)
--Ziggy Harrison-Tikisci 10:41, 29 September 2011 (EST)
--Ziggy Harrison-Tikisci 10:41, 29 September 2011 (EST)
--Ziggy Harrison-Tikisci 10:41, 29 September 2011 (EST)
--Ziggy Harrison-Tikisci 10:41, 29 September 2011 (EST)
Group 6:
Great intro, brief but covers everything. Good amount of references for the information provided Genetics part was covered well.
The reference under diagnostic techniques should be with the other references and hopefully, by the end of semester there will be images where it says “insert images”
Good use of tables.
Maybe a few more pictures and the page will be perfect.
Evidently there’s been good work put in and the information has been researched well.
9-13 are all the one link so it should be one link not 5 separate links.
Clear and concise
z3332178 =]
Peer Review
- Introduction: the layout is a bit messy. Maybe get rid of the double spacing. It might also be a good idea to include an image e.g. maybe of a heart. Needs to include more references in this section.
- History section was well written. I suggest putting the quote in a blue box or highlighting it in some way to make it stand out. Try including a table or timeline to summarise the key events and findings.
- Signs and symptoms; Good layout and presentation of information. Easy to follow and understand.
- Genetics: shows it has been thoroughly researched. Like the use of images to compliment the text. Try and put the information in a table. The section is too lengthy in comparison with the other sections. Needs to hyperlink certain technical words to the glossary.
- Pathophysiology: well written. The information is concise and easy to understand. Good use of student drawn images.
- Great idea summarizing the information on 'diagnostic tests' in a table. Get rid of the in text referencing in the table.
- Add a border around the table in the treatment/management section.
- Other sections; good information. The referencing need to be fixed, it's not consistent. Try and include more images or tables in the prognosis, future directions sections to break up the heavy text. These sections seem a bit mundane compared with the rest. Prognosis section required more referencing.
- Glossary; need to be expanded.
--Z3291622 10:06, 29 September 2011 (EST)
‘’’Peer Review’’’
Some places for improvement.
- Double spacing of paragraphs looks awkward.
- Introduction does not flow very well. Sentences are very choppy.
- History section would benefit from a timeline rather than paragraphs as it is a bit hard to follow.
- In the epidemiology and symptoms sections need some more content. Seems very minimal. Also images?
- Diagnostic section needs the rest of the information added to its table. “Insert text here”. Also use of bolding or different font sizes would benefit this table.
- Glossary could be expanded, very minimal.
- References need to be fixed. There are many that are just a web address. Full citation is needed.
--z3217043 09:19, 29 September 2011 (EST)
Group 6 Peer Review
- Majority of page is in a logical and organised manner however maybe switch aetiology and signs and symptoms to make it flow better?
- History section had good, clear subheadings
- Epidemiology seems brief relative to other sections-perhaps merge with a section or expand on this if possible
- Table in Diagnostic tests-great however an image would help break up the text
- Glossary could be extended further
- Referencing inconsistent
- Image/text ratio is good however layout could be improved
- Overall, a very informative and interesting page. Visual appeal could be worked on but once a few things are adjusted, it will finish it nicely
--Fleur McGregor 09:10, 29 September 2011 (EST)
Group 6
- Introduction is good and very clear, except there are no references, easily fixed but (Y)
- History could be incorporated into a table, or at least, the dates could be bolded or highlighted to establish progress through time.
- Good use of subheadings under ‘Signs and Symptoms’, might be beneficial to include more images as examples of each symptom, but just enough to provide a balance between text and images
- Genetics – well organised information, incorporation of images is excellent, many of the terms mentioned here could be defined in the glossary
- ’Pathophysiology and Abnormalities’ – this section definitely needs to be referenced, but good info.
- ’Treatment/Management’ – this table needs borders, i was easily confused as to which paragraph i was reading, but great info.
- Glossary could have a lot more terms included.
--z3331469 07:02, 29 September 2011 (EST)
Group 6 Peer Review
• Nice and simple sub-heading structure. I like the consistency of two images throughout the page. However I feel like you have lots of text with fewer images.
• Introduction is clear and to the point, however where are you references? And an image in this section is always good to give a representation of the abnormality from the start.
• History is really good! Clearly researched very well and good images! Interesting to read. However, the use of a timeline or ‘bolding’ all the dates would make it an easier read.
• Epidemiology is good, however I think you could elaborate more and possibly add a table/graph.
• I personally think that your signs and symptoms would look better displayed in a table. Definitely need more images here, possibly one for each sign/symptom.
• Why are signs and symptoms before the aetiology and pathogenesis of the disease? For me, it’s more logical to explain the cause and how the disease comes about before the signs and symptoms.
• Pathophysiology and abnormalities is a really good descriptive section. Well explained! And good use of images. But where are all the references?
• Diagnostics test has interesting information. Inconsistent referencing system to the entire page, also desperately in need of images to break up all that text.
• Future directions is well summarised, with relevant headings.
• Not really sure what’s going on with your referencing, but you need to have a consistent system throughout the entire page with no doubling up of articles.
--z3289829 02:44, 29 September 2011 (EST)
- Intro: Best not to start off the introduction with stats, people will quickly lose interest. I like how you’ve given a very brief idea of each subheading. This section would benefit from a picture , something to grab your attention.
- History: A timeline would be best, as this section isn’t as significant as the others so it doesn’t need to be in extensive detail.
- Epidemiology: “ It makes up around 7%-10% of cardiac congenital defects. Moreover, epidemiological studies show that it occurs in 3 out of 10000 live births that are delivered” repetitive. Best if not mentioned in introduction, as it is useful fact in this segment. Needs a little more detail, quite short in comparison to other sections.
- Signs and Symptoms: Good use of subheadings, need more images. Loved the audio! Very interesting. This section needs to come in after aetiology though.
- Genetics/Aetiology: Quite extensive, very detailed and understandable, but a lot longer than the other sections, it could do with a bit of trimming. Also the one type of image being used 3 times is not appealing, perhaps hand draw it in different colours or get a different style of drawing representing it.
- Pathophysiology: Like the subheadings and it’s easy to follow the information.The first image is great, the 2nd image could be broken down and hand drawn to compare the normal blood flow with TOF blood flow individually, instead of having the other conditions included. This would make it more clear.
- Diagnostic Test: Table is clearly incomplete. Add images, and add colour. The text is also not referenced. Why is there one reference at the bottom of the table?
- Treatment: Quite detailed and informative. There are many sections missing references above the table.
- Glossary: INCOMPLETE. There’s many more words you can add here.
- References: Links to other pages don’t count as references- that needs to be fixed.
- Overall: Great job. You’re image:text ratio is little unbalanced, as you need more interesting pictures. Needs a few changes here and there as I’ve mentioned above but it’s looking good so far.
--z3290270 02:29, 29 September 2011 (EST)
Peer Review
- Introduction needs more/any references.
- Use of a quote in History is interesting.
- History sections seems to be too focused on certain specific procedures rather than their significance for the disease itself and the patients.
- Some grammatical errors in various sections.
- Epidemiology seems a bit short...if no other details can be found for it, consider merging it with another section?
- Signs and Symptoms can use more references, but the subheadings used are very fitting and set out the information well.
- The subheadings in Genetics/Aetiology mean nothing to me. Explanations? On that note, the glossary can be more filled out.
- The layout of Genetics/Aetiology can probably be tweaked a bit.
- Pathophysiology is set out very nicely, but it needs references.
- The table in Diagnostic Tests is very succinct, but the section needs some text, if only to introduce/explain the table. Also, there is a random reference at the bottom.
- Treatment/Management needs more references. The table therein is strange, but the information is very well presented.
- The inclusion of a Prognosis section is interesting, but maybe consider putting it within Treatment/Management?
- Inclusion of Future Directions is very good but the references need to be cleaned up.
--z3290689 01:15, 29 September 2011 (EST)
Group 6
- Introduction: well summarised, but paragraphs don’t flow. This section needs referencing and a few terms could be defined in the glossary.
- History: good use of images to break up text. Maybe consider a timeline just to summarise the section since there is a lot of information here to digest.
- Signs & Symtoms: I like the use of subheadings – clearly indicates topics discussed. Maybe consider un-bolding the list of mumurs since they are not headings, just to keep the formatting consistent.
- Genetics: I like the images which are consistent throughout and the use of gene profiles – nice touch.
- Pathophysiology and abnormalities: well written & formatted section. Referencing?
- Treatment/Management: The only thing I would suggest is to add borders to the table so that the rows are clearly separated. I like the external links.
- Perhaps the page needs just a few more images/tables to break up the heavy text. And the glossary should be expanded.
--Lisa Xiao 00:48, 29 September 2011 (EST)
Group 6 Hey, nice progress with your page, all sections have similar amount of content which were interesting
- The key points relating to the topic that your group allocated are clearly described.
- Introduction: Referencing needs to be improved here
- History: content is good but too wordy. I think a summary or a simple timeline would be good
- Epidemiology: Where's the reference for 3/10000 live births?
- Signs: ok section, but could do with more images here
- Genetics: If using abbreviations, such as TBX1 gene, you should explain what it is, ie. TBX1 gene (T-box 1). Also need to work on referencing here as well. How about organising all the content in a table? have in columns: gene, gene profile, frequency, etc.
- Pathogenesis: I'm not quite sure about this, but do you need permission to adapt an image from an article? (I'm referring to the '4 defects' image)
- Diagnosis: I'm sorry, but this section is a bit bland, though the content is very informative. I think some images here would be good
- Treatment: Referencing! Also, personally, that green is too bright, maybe find a more neutral, soothing colour?
- The choice of content, headings and sub-headings, diagrams, tables, graphs show a good understanding of the topic area.
- Need to find more images, I feel some of the information could be more effectively presented in table formate rather than lengthy text
- Content is correctly cited and referenced.
- VERY poor referencing, which makes me question the reliability of the content in some sections
- The wiki has an element of teaching at a peer level using the student's own innovative diagrams, tables or figures and/or using interesting examples or explanations.
- needs a lot more images
- Evidence of significant research relating to basic and applied sciences that goes beyond the formal teaching activities.
- research done is evident, just need to reference
- Relates the topic and content of the Wiki entry to learning aims of embryology.
- Clearly reflects on editing/feedback from group peers and articulates how the Wiki could be improved (or not) based on peer comments/feedback. Demonstrates an ability to review own work when criticised in an open edited wiki format. Reflects on what was learned from the process of editing a peer's wiki.
- Evaluates own performance and that of group peers to give a rounded summary of this wiki process in terms of group effort and achievement.
- The content of the wiki should demonstrate to the reader that your group has researched adequately on this topic and covered the key areas necessary to inform your peers in their learning.
- Develops and edits the wiki entries in accordance with the above guidelines
"What would improve this project...."
- glossary is very lacking in terminology
- need more images
- REFERENCING!
--z3291643 23:25, 28 September 2011 (EST)
GROUP 6:Tetralogy of Fallot
- Info in the intro is succinct and informative but sentence structuring and punctuation lets this down e.g. "These genetic mutations contribute to the four characteristic defects, in the heart of a patient having TOF" - comma is misplaced here
- "disease that occurs in 3 in every 10000 live births" -consider rephrasing this
- Intro needs an image to draw attention of reader
- While I appreciate the sectioning of the history section, i think that a chronological timeline may be more comprehensive for the reader, I feel that some of the dates are all over the place, also the history of this disease seams to stop at 1950s, could you maybe find more recent findings or contributions
- History images are good but need to be properly referenced and student template is missing from the first image
- I feel epidemiology section is a little underdeveloped, could you possibly find some more stats and compare incidence in several countries?
- Signs and symptoms has good info, but i feel that some sections could be expanded more
- signs and symptoms could use more images to accompany info
- I like the audio links to the heart signs
- Genetics/Aetiology section looks like it has been thoroughly researched, i like the structure of how each gene is dealt with, however, this info could be better formatted in a table and summarised a little more (if you are going to include all this technical info make sure it's explained in glossary maybe), also images in this section need better descriptions in the legends
- Pathophysiology and Abnormalities (I'm not sure if this is the best heading, could maybe be associated conditions or associated abnormalities or even just Cardiac abnormalities), info here is good but could be expanded a little more seeing as cardiac abnormalities seem to be a major manifestation of this anomaly
- Diagnostic tests section could be better placed further up? appears to have some info missing, and in some parts too much text, maybe could be summarised a little. Images could help break up the text, use of a table here is suitable but colour for the side headings could make it stand out a bit more. Referencing really needs to be fixed for this section
- Treatment and management is well researched, however Palliative Procedures could use more referencing esp. at the beginning. Table included is good but could be improved with colour and sectioning
- Prognosis has good inf but lacks referencing
Overall:
- More images are needed to balance out text
- Reference list needs work, don't think it's sufficient to just provide links to websites
- proof reading is needed to fix spelling mistakes, grammar issues and general sentence structure
- Glossary needs finishing, consider linking glossary words to the text and adding any acronyms used
- referencing of some images need to be fixed and student templates are missing in some
--z3331556 22:12, 28 September 2011 (EST)
Group 6
- The introduction is good but it would be better if there was some referencing.
- The history seemed abit chunky ? maybe a summarised version in a form of a timeline would be good. But overall the use of images is good, it breaks up the heavy text more.
- Epidemiology was abit too short, maybe expanding on why it is this pattern and etc would be a good idea.
- Signs and Symptoms had a nice summary of information. Maybe more pictures would make it more easy on the eyes because this section is quite big on the info. But the audio is a interesting idea!
- Genetics - Firstly, maybe get rid of mark's post. Secondly the layout of information is not that appealing, maybe you could underline the headings to make it more definite. Lastly, the use of images is good! it is very consistent for all genes.
- Diagnostic Tests section was not referenced! If it was then this section would be a winner, if it was completed!
- Overall, it looks like you guys have done alot of research. Good job!
--z3330313 00:01, 29 September 2011 (EST)
Group 6:
•Very text heavy, perhaps an image in the introduction could be added to grab the attention of the reader and create a better balance between text and images.
•Also, there are no references in the introduction. The source of this information needs to be references properly.
•The history section is worded well, though it may be more visually appealing and better formatted in a timeline. Also it seems to stop at the 1950s period. Is there no other recent research or developments made that could be added to bring the timeline up to date?
•The epidemiology section is quite short
•Good description of the signs and symptoms and good use of external links in this section for further information
•I like the diagnostic tests table, although it is incomplete at the moment, when the images and other information is added then this section will be very well done. Just make sure that it is referenced properly though, because it seems to be lacking referencing at the moment.
•Glossary needs to be completed and a number of the references are repeated
•Good work overall, some sections just need to be fixed up and completed and some more images added, but the overall formatting seems fine.
--z3332183 21:30, 28 September 2011 (EST)
Group 6
*The key points relating to the topic that your group allocated are clearly described. All main sections are there. History is well done, perhaps a time-line could be used?
*The choice of content, headings and sub-headings, diagrams, tables, graphs show a good understanding of the topic area. Good use of headings, subheadings in history was well used.
*Content is correctly cited and referenced. File:Finger-Clubbing.jpg, File:TBX1.jpeg, File:NKX2-5.jpeg, File:JAG1.jpeg and File:Normal fetal blood flow and Tetralogy of Fallot.jpg should be referenced properly.
*The wiki has an element of teaching at a peer level using the student's own innovative diagrams, tables or figures and/or using interesting examples or explanations. Well done student image with good explanation. More images would be good. Include more terms in glossary. Table in diagnostic tests has too much text. Table should be used to summarise, put main block of text outside of the table.
*Evidence of significant research relating to basic and applied sciences that goes beyond the formal teaching activities. Prognosis needs more referencing.
*Relates the topic and content of the Wiki entry to learning aims of embryology. Good information in genetics, but maybe relate the symptoms to problems? (eg: what does Conotruncal anomaly face syndrome mean for the person/fetus?)
*Develops and edits the wiki entries in accordance with the above guidelines. Has developed wiki according to guidelines but some changes could be good.
--z3329495 21:18, 28 September 2011 (EST)
Peer Assessment Group 6-Tetralogy of Fallot
- An image in 'Introduction' will make the beginning of the page more lucrative
- History might work better as a timeline, with bullet points and bold the dates so it is easier to follow.
- Surgical history and Contemporary History has a lot of information, some of it overlaps.The whole section could be replaced by a 'easy to follow' timeline. Good pictures in history.
- Are you going to expand on 'Epidemiology',? Maybe talk more about the actual pattern of occurrence rather than just a couple of observations from epidemiological studies?
- Are you also adding a description for Aortic Insufficency Murmur? The other three heart murmur types have an explanation except for this one.
- There are too many gaps in between the lines, makes the page look a bit sparse.
- Genetics looks quite full on. You may want to add more distinct subheadings to make it easier to follow and keep the reader's attention
- 'Abnormalities' looks great however you might want to change the italics to just bolded headings, makes the page look more consistent. Also make the numbers bold if you are going to have the text following the number bold.
- Though in number 4 under 'abnormalities' can you give a quick definition on what hypertrophy actually is?
- Even though the table is coming along make sure you take the reference off from the bottom of the table and add pictures. It looks like a work in progress. Also the referencing style is different to the rest of the page
- The student drawn pictures under treatment is nice.
- The table is also quite succinct
- 'Future directions' doesn't sound great as a heading. Use something more appropriate to the context
--Tahmina Lata 19:21, 28 September 2011 (EST)
Peer Assessment Gr 6
- History – what has been done in the last 50yrs? It seems to stop around 1950.
- Signs and symptoms- needs to be edited so it flows better, avoid long wordy sentences – just break them up into 2 (e.g abnormal growth part). Do you have a pic of a blue baby?
- Genetics- need a bit more space between each gene section, just to make it really clear (e.g. between the end of 5q34 and 20p12.1)
- Diagnostic tests table is good (but incomplete), perhaps consider using colours like other groups has? But the bright green of the shunt table is too bright, it hurts my eyes haha.
- References under the reference table needs to be fixed – do you want them to be in the table, or a list of them or what? Same for the references in the future directions section.
- Very well researched and thorough explanations
- Maybe expand the glossary?
- Reference section has some that double up (one after another) – there is a way to fix this and condense it.
- Do you have some photos of real hearts that have been affected by this disorder?
--z3332824 17:46, 28 September 2011 (EST)
Group 6: Peer Assessment
- It would be good to see more images
- The introduction would be more engaging if it had an image
- The history section is informative however would be nicer in a chronologic fashion. May be a table?
- The extra surgical history makes it clear that surgery plays an important role. Good
- Signs and Symptoms and genetic abnormalities are good overall. Many of the terms need to be added to the glossary though and it might be better to put aetiology first.
- It's a quite big and text heavy table in your diagnostic section. May be you can make it shorter, put pictures in
- I found quite a few words that should be in the glossary
- There is no title for your reference section and it looks like you should have more references for the amount of text that you have written
- Overall your page is very informative, good content. You need more images, appropriate referencing and a more complex glossary. --z3279511 17:11, 28 September 2011 (EST)
Group 6 Peer Review
- Good introduction, although an image straight up would be nice!
- History is presented well, although a table format at the end that summarises everything you have said would be nice. Also, does the history stop around the 1950's? It seems like there has been nothing done on it until 1970/1980? Hence, the table format would be nice if it appears that I've missed information.
- Epidemiology section is really quite short. Is there nothing more that can be said on it? Does it have preference to specific race?
- Signs and symptoms - from the way that the page is formatted it appears that you've gone down onto the level 4 headings with 4 ='s paraphrasing each heading. Try to use 3 or so just to make sur e the headings are larger and each subsection can be identified.
- The genetics/aetiology section should be explained better; whilst this is aimed at academics, it is almost impossible to understand the information pertaining to the genetics section.
- The pathophysiology and abnormalities section is well explained, and the diagram is excellent to show exactly where the problem lies. A well done section, and a well-selected image for the blood flow patterns.
- Diagnostic tests: Still need to insert those images on the right hand side column! Also, ensure that the referencing is done in the correct format - this section still needs work.
- Treatment/Management section is done well, with a good balance between text and table.
- Current and Future research: Perhaps more dates? The formatting here also needs to be fixed up, and try to have dates on the papers that you are quoting from (although I understand it's difficult without the references in place)
- The glossary section needs more terms added to it! Especially from the genetics/aetiology section which is already terribly difficult to understand.
- Referencing section is quite short - but understandably the whole project feels like the referencing just needs to be finished.
- Overall a nice-looking project with a lot of promise. The spacing and format of the project makes it easy to read - perhaps more images and the use of some tables might also assist in the presentation of this project.
--Leonard Tiong 10:49, 28 September 2011 (EST)
Group 6
- My first impression is that this project is lacking images. There is way too much text in comparison to images.
- An image would nicely complement the introduction
- I feel that history would work better in a timeline
- Epidemiology needs a table/graph
- Good links in signs/symptoms although another image would be nice
- Genetics needs to be explained a little better
- Student drawn images were great- obviously a lot of effort has been put into these
- Diagnostic test table needs an image and needs to be referenced properly
- Again, an image is needed for prognosis
- Glossary needs to be extended
- Overall a good project but you need to fix a few things
Group 6
- Introduction: the contend is ok, but the structure could be clearer
- History: too text heavy, a timeline would be nice
- Epidemiology: more content would be good
- Symptoms: the picture could be more general
- Genetics/ Aetiology: the structure could be better, maybe use some more subheadings, and put the gene profile in tables
- Pathophysiology: you need references
- Diagnostic tests: why does it say “insert images”, that should be fixed
- Treatment/ management: looks like there are some references missing? Deleate “Want to learn about more surgery and treatment methods?”, the contend is good, types of shunt would look better as a table
- Prognosis: references missing? good use of subheadings,
- Glossary: incomplete
--Z3387190 21:52, 27 September 2011 (EST)
Group 6 peer assessment
- Introduction is clear though lack images where a image of example of a blue baby would suffice
- History begins clearly though becomes about surgical history instead of the disease, where time line is not even present of how understanding of this disease improved.
- Epidemiology should be expanded either the genetics of the disease, in general have more information of the causes, incidence and distribution of the disease.
- Signs and symptoms poorly structured and requires more images also doesn’t have an introduction to the signs and symptoms. Although the extra links to comparison of the heart is useful and nicely used.
- Pathophysiology should add supplementary information to back up all the information.
- Diagnosis please add the images, while there is the content though no image following also first box has “insert text” very confusing.
- Treatment/management indicate the separation of surgery and other treatment types in the introduction which is lacking otherwise all is A ok
- Glossary needs to be referenced to other sections of the web page also expanded as most language used is unknown without a dictionary.
- Referencing needs to be fixed as links is not proper referencing also the repeats need to be removed
z3332250 23:53, 26 September 2011 (EST)
Comments on Group Project 6
Strengths:
- The flow between sections and sub-sections is good with appropriate placements of headings and sub-headings.
- Some of the references have good use of multiple referencing so as to avoid duplication.
- The external links under signs and symptoms is very apt and will interest readers.
Weaknesses:
- Almost half of the references are not properly formatted.
- Some of the words that should be in the glossary are not under that section e.g. Velocardiofacial, Conotruncal, Hypothyroidism, nengoitrous, embryotoxon.
- Punctuation in some sections can be better.
Specific corrections:
- ”muattional” under 22q11.21 sub-heading is spelt incorrectly.
- ”cyamnosis” under signs and symptoms is spelt incorrectly.
- ”enlargenemt" under clubbing is spelt incorrectly.
- Insert a timeline under history to provide a summary.
- It might be better to have genetics section before signs and symptoms.
- Under Treatment/Management, it will be good to put “medical therapy”, “palliative procedures” and “surgery” as sub-headings.
--Z3389806 08:03, 26 September 2011 (EST)
Group 6 Critique
- • Introduction is ok, however it needs to be structured a lot better than what it is
- • History is interesting
- • Epidemiology needs a lot more detail. A few lines is not good enough
- • Signs and Symptoms is ok
- • Genetics needs to be explained a lot more clearly than what it is
- • Abnormalities is ok
- • Diagnostic tests table is impressive
- • Treatment/management section is very good
- • Prognosis and future directions section is great
- • Glossary is incomplete. Check the first term and fix this
--Robert Klein 19:05, 24 September 2011 (EST)
Tetralogy of Fallot
- An image in the 'Introduction' to introduce the topic would not go astray
- "...Infants turning blue when crying..." middle of sentence, no capital is required. What is tet spells?
- History might work better as a timeline, otherwise at least bold the dates so I know whats going on
- Surgical history has been covered through most of 'Contemporary History', there's not a whole lot of point having two subheadings here
- The 'Epidemiology' is a bit sparce? Are there no other stats to add to this section?
- There is a lot of good in information in 'Genetics', but I think you need something to break it up, you've got the images of the chromosomes (which are very good), but can you find other images? Maybe put some of the information into a table?
- The 'Abnormalities' section looks really good. The information is clear, succinct, with good illustrative images
- Though in number 4 under 'abnormalities' can you give a quick definition on what hypertrophy actually is?
- Diagnosis is poor, it isn't referenced and clearly isn't finished ("insert text here"). This does not flow on from the rest of the page at all. It looks a bit dry with no colour or images
- There are minimal references in 'Treatment', surely you didn't all that information out of only a few papers?
- I like the table in 'Treatment'
- Can you make the subheadings in 'Treatment' as actually subheadings as opposed to just bold?
- It's coming along, but you need more images! It starts off well, but there aren't many toward the end.
- Make sure you finish the project off!
Group 6-
- No way near enough images. As I scrolled through there was HEAPS of text and only a few images, all of which are on the right hand side. It would be better if they were scattered around
- An image in the introduction would be helpful
- What are ‘tet spells’? mentioned in the introduction (described later but when seen in the introduction it looks like a typo)
- History would work better as a list of dates rather than paragraphs. I do like the section at the top with the quote though
- Epidemiology needs an image- perhaps a table or a graph.
- Signs and symptoms could do with another image to visualise the clinical manifestations
- I really liked the audio clips but the first one didn’t work on my computer? I couldn’t hear anything. Not sure if it was just me
- I think you can come up with a better way of formatting the genetics section. Maybe a table? The information is good it just looks a bit funny
- The pathogenesis doesn’t actually say HOW is happens in infants. Is this a condition formed during embryonic development or after?
- The diagnosis section is far from complete. This needs to be corrected
- Diagnosis section is also not referenced properly
- Why is there a reference at the bottom of the diagnosis section?
- As funny as this was: ‘Want to learn about more surgery and treatment methods? Check here!’…. maybe not appropriate sorry. It should be a little more formal. If you want the reader’s attention- try colour.
- Prognosis- image needed please. Maybe a graph?
- The glossary also needs to be extended
- The references need to be tidied up- there are also not many?
- You need to reference your images properly. ‘normal fetal blood flow and tetralogy of fallot’ is an example. You have but the copyright but not the reference. The web address is not a reference
- You are clearly on your way with the project but more work is required. You need to FINISH the content and format it a little better with more images.
Group 6 Assessment'
- First, I’d like to note good job on using a reference more than once in the correct way instead of referencing the same thing multiple times. At least this is done in the first few sections. First time I’ve seen this done correctly!
- The introduction, however, has no references whatsoever. Where did this information come from?
- It might also be good to add a simple picture in the introduction section so it looks more appealing.
- Good information included in the history section. It might look better if this were laid out in a bullet format though.
- The epidemiology section looks rather bland. Not only is there not a picture, but there also isn’t very much information included. Think about what else you could include here or what you could go into depth about.
- The signs and symptoms section has good information, but it might be a good idea to represent this information in a better format, possibly in a chart, with pictures of each symptom included in the chart.
- Finger-clubbing.jpg also needs a detailed description still.
- Good organization and format under the Genetics section.
- Under the pathyphysiology and Abnormalities section there are no references made. Where did this information come from? Diagnostic Tests and Treatment also needs more referencing.
- Pictures still haven’t been inserted into the Diagnostic Tests chart.
- More referencing is needed for the Prognosis section. Also, does the glossary terms need to be referenced?
- It would be a good idea also to have the glossary terms linked with the words in the wiki page, so that the reader can easily get access to the word in the glossary. References 7-14 are the same reference. Fix these so they are under one single reference number.
- For the references given throughout the wiki, there isn’t any consistency in how the [#] is given. The [#] is sometimes right after the sentence, sometimes a space is given between the sentence and citation number, and the end of the sentence (period or comma) is sometimes before or after the reference #...
- Overall, there is a substantial amount of information given within this page, which is good. I like the basic format of everything and most of the pictures which are included. Just work on weaving everything together better and referencing things correctly. Good job!
--Z3391078 15:32, 27 September 2011 (EST)
Group 6
- Nice overall structure and good use of headings and subheading. It gives the page a nice flow.
- INtroduction is nice and straight to the point and gives the reader a good overview of your topic.
- I like the historical section with interesting subheadings used, maybe you could add a timeline just to simplify the info.
- Signs and symptoms nicely arranged. could you add some more pictures here?
- Pathophysiology and Abnormalities section need to have the references accompanying the information. Just so the read can identify where all the info is from.
- The diagnostic tests table would be nice with some colour and when the images are it will look complete. It's a little text heavy for a table maybe try bullet points. also the referencing system has changed in this table? and a little unsure of the reference at the bottom of the section?
- Treatment/Management section is nicely arranged.. could you add another picture here just to compensate for the amount of text. the table really brightens up the page!
- Future directions section is nicely summarised and I like the tone of voice used here. just make sure the referencing is correct as it is a little confusing and interrupts the flow of the section.
- Maybe the use of similar tables and colour scheme will increase the continuity of the page.
- Make sure your references are not doubled in the list.
- Ensure all of your pictures are correctly referenced.
- Make sure all acronyms and scientific wording is in the glossary.
- Intro: What's a tet spell?
- History: Very good in general. Not sure it makes sense to split it into 2 parts, with surgical being separate? I think it would work just as well combining the two.
- Edidemiology: Looks fine
- Signs and Symptoms: Otherwise good, but considering you have a whole subsection entitled clubbing, I'd suggest explaining what it is right there, and not just in the glossary.
- Genetics/Aetiology: Love the detail and depth, though the more technical terms should be explained in the glossary. Tiny comment: "there is only a single copy of the gene in one allele" - I know what you're trying to say, only one allele is functioning, but saying it like this kinda means, this allele only has one copy of the gene, whereas usually there are multiple copies of a gene in one allele, which is, as far as I know, not the case (that would just be contradictory, as an allele is a copy/varient of a gene).
- Pathophysiology and Abnormalities: Very good, nice use of figures.
- Diagnostic Tests: Not sure I like the table. It is just a hell of a lot of text... in a table. It doesn't really help give an overview, maybe just have subheadings, with (once you have an image) a picture on the side? Also, referencing needs fixing.
- Treatment/Management: Very good, nice amount of detail. Again not sure a table is required. Also, the colour is a bit in your face, but that might just be me. I like the links at the end.
- Prognosis: Content seems fine. A bit odd there's only one reference?
- Future directions: Otherwise seems fine, though referencing needs fixing.
- Glossary: A bit poor. More technical terms need to be explained.
- General: The last few sections lack some figures, it is just a lot of text. The content in general (as in of the whole project) was really good, so well done!
Peer Assessment: Group Project 6
- The introduction and the section on pathophysiology and abnormalities have no references. This needs to be rectified.
- The introduction and some of the history section have short paragraphs that are only one sentence long and would be improved, both for formatting and information purposes, by incorporating them into the rest of the information.
- Inserting a small timeline in the history section would make the sequence of events more accessible to the reader.
- Some sentences are too long such as, 'Children with TOF don’t grow at the rate of normal children as whilst breastfeeding in infancy, the babies would get tired quicker and during the growth of the infant, normal functionability of the heart and oxygen saturated blood is needed for proper growth'. This sentence could be broken up and also improved by a greater explanation of why the process of growth is abnormal in TOF.
- Maybe explain more about what 'clubbing' is.
- In the diagnostic tests section the images need to be inserted and needs to be properly referenced. The information is good but as noted one section is totally void of text.
- The section on prognoses needs proper referencing.
- The section on future directions is well written, however the referencing needs to be adapted to the wiki format.
- Under the information in some of the images you have uploaded such as in the portait of A. Fallot, you still need to add {{Template:2011 Student Image}}.
- The project is informative, however formatting and referencing are issues that need to be addressed.
--z3217345 22:23, 27 September 2011 (EST)
Group 6:
- Introduction: Maybe briefly explain the symptoms and the physiological implications of a tet spell and what palliative care is, alternatively hyperlink these words to the signs and symptoms and treatment sections. There are also a few mistakes such as no space after commas “chromosomes 5,20 and 25.” and an incorrect capital letter after a comma “TOF patients include, Infants turning blue”, just make sure to correct these little mistakes by re-reading this section. An image here would also be good.
- History: The history you do have is very comprehensive and easy to read, however the dates get lost in amongst the text. If you bold the dates or include a brief table after the text it will help the reader to track the history better.
- Epidemiology: Very short, could you maybe elaborate to why TOF affects slightly more males than females?
- Signs and symptoms; the information here is very good, it could be improved with the use of more images. I’m not sure if it’s just me or not but I couldn’t hear anything in the normal heart video but the TOF heart video was fine?
- Genetics: This section genuinely scared me, it is a lot of text and a lot of scientific text at that. I found it difficult to read and ended up skipping over this section. Maybe try explaining the genes in your own words. The images do help though so maybe make them bigger. I did find a little typo “gene taht results to TOF” so make sure you proof read once you’ve edited again.
- Pathophysiology and abnormalities is done really well with great visual aids (second image needs to include “{{Template:2011 Student Image}}”). Only suggestion is to leave the sub-headings just bold - no need for italics.
- Diagnosis is obviously unfinished but once the images have been added, the blank text has been filled and some colour is added to the table, I think it will be a great section.
- Treatment and management: The image here is also missing the student template. Spelling mistakes found so proof reading is required “oxygen & intravenous morphine to provides more blood flow”. The table here could be coloured to liven up the page.
- Prognosis is done well but maybe a pie graph could be inserted to show the major causes of death in surgically untreated patients as a visual.
- Future directions is also very good – the referencing just needs to be fixed.
--z3290815 20:31, 28 September 2011 (EST)
Peer Review
- really well done
- format and structure of the wikipage was consistent throughout
--z3060621 21:36, 28 September 2011 (EST)
Test:
| Diagnosis |
--z3291423 11:57, 22 September 2011 (EST)
Hey Jaz, thanks for letting me know...my english can fail me at times.....lol...fixed it up... regards--Z3291317 18:49, 18 September 2011 (EST)
Hey guys! i just realised that the caption of helen taussig and ballot say portraight....not PORTRAIT!?!! i tried to change it but it don't really know how..anyone have any ideas to this?! :S thanks --z3291423 00:06, 17 September 2011 (EST)
Table Test! --z3291423 22:16, 16 September 2011 (EST)
| Type of Shunt | Description | Reasons for it not being used | Image |
| Pott’s Shunt | This shunt is a connection that is established between the lower part of the Aorta (on the left side of chest) to the left branch of the Pulmonary artery. | The shunt has a tendency to increase the pulmonary blood flow and it is also very hard to close when complete repair is undertaken | Insert image |
| Waterston Shunt | This shunt was placed between the back of the Aorta, to the right branch of the pulmonary. | This shunt’s use is more suited to those with pulmonary artery stenosis and also the procedure is quite difficult to perform. | Insert Image |
| Glenn Shunt | The Super Vena Cava is anastomosed via a shunt to the right pulmonary artery. | This procedure is very complicated and difficult to perform, also complete repair becomes a laborious task. | Insert image |
Table test (fingers crossed!) --Jacqueline Ellero 10:49, 15 September 2011 (EST)
TOF diagnostic techniques
| Diagnostic technique | How the procedure works | Presentation in TOF patient | Image |
|---|---|---|---|
| Physical examination | TOF is often diagnosed during fetal life by echocardiography (Apitz, Webb, & Redington, 2009). If TOF is not detected during fetal life, certain signs and symptoms at birth may alert the need for further investigation. These signs and symptoms include mild to moderate cyanosis, which worsens when the baby cries, difficulty feeding and difficulty gaining weight. However, TOF often goes undiagnosed until adult life. Most adult patients will appear normal, however, some may present with cyanosis and clubbing of the fingers. The jugular venous pressure is usually normally (raised jugular venous pressure often indicates right ventricular failure). If the aorta is pushed to the right (so it is continuous with both the left and right ventricle), a lift below the right sternoclavicular joint may be noted. (Somerville, 1993) | Insert text here | Insert physical examination image |
| Heart murmurs | Heart murmurs are sounds caused by the turbulent flow of blood. They are heard using a stethoscope. They are often the result of problems including valvular stenosis (narrowing of valves), valvular regurgitation (leakage of valves due to incomplete closure) or defects in the heart wall allowing blood to flow in unusual directions. | Examination of the heart of a patient with TOF may reveal a loud second heart sound (produced by the closure of the pulmonary valve). A harsh systolic ejection murmur may be heard and a palpable thrill may be felt along the left sternal border. These sounds occur because the pulmonary outflow tract is obstructed. Although this murmur is often present, sometimes it may be short or difficult to hear and is often missed on physical examination. A pansystolic (occurring throughout the whole of systole) murmur may also be heard. This type of murmur occurs due to the ventricular septal defect between the left and right ventricles. The increased pressure in the left ventricle forces blood back into the right ventricle, causing a murmur, which lasts the whole of systole (contraction phase). http://ccjm.org/content/77/11/821.full | Insert heart murmur image |
| Electrocardiogram | Once TOF is suspected, electrocardiogram and chest radiographs are performed. Electrocardiography is used to assess the electrical activity of the heart. The electrical activity is detected by electrodes, which are placed on the skin of the patient and recorded by an external device. | The electrocardiogram is extremely important in detecting a right bundle branch block (a block in the electrical conducting system of the heart), which is common in patients with TOF. An electrocardiogram will also reveal a heart that is deviated slightly to the right and an enlarged right ventricle due to the ventricular hypertrophy.(Somerville, 1993) | Insert electrocardiogram image here |
| Chest radiograph | A chest radiograph (or chest x-ray) uses ionising radiation to develop an image of the patient’s chest. It is used to diagnoses many conditions including the thorax and structures within the thoracic cavity including the heart, lungs and major blood vessels entering and leaving the heart. Chest radiographs are often used to screen for certain diseases but further tests are required for a definitive diagnosis. | In a patient with TOF, a chest radiograph will demonstrate a prominent right ventricular shadow, giving the heart a boot-like appearance, which is typical of patients with TOF. The right ventricular hypertrophy causes the apex of the right ventricle to rise on top of the relatively unfilled left ventricle, giving the heart its boot-shaped appearance on examination. (Bailliard & Anderson, 2009) The radiograph will also show a right-sided aorta in approximately one-quarter of patients. (Somerville, 1993) | Insert CXR image here |
| Echocardiogram | An echocardiogram (also called a cardiac ultrasound) is performed to confirm the above findings. Echocardiography uses ultrasound to produce two-dimensional (and now also three-dimensional) images of the heart. It assesses cardiac tissue, valve function, the velocity of blood flow and any abnormal communications within the heart. | The echocardiogram identifies important abnormalities of the heart including obstruction of the pulmonary outflow tract, the size of the pulmonary arteries, the degree of aortic override and the size of the defect in the interventricular septum. (Bailliard & Anderson, 2009) | Insert echo image here |
| Magnetic resonance imaging | Magnetic resonance imaging (MRI) is evolving as the most important technique for evaluating the size and functioning of the right ventricle. An MRI machine uses a magnetic field to produce a detailed image of the scanned area of the body. It is especially useful in viewing soft tissues as it provides greater contrast than techniques such as x-ray. | MRI’s are important in assessing pulmonary valve competence and the severity of regurgitation (the amount of blood that flows back into the right ventricle due to the incomplete closure of the pulmonary valves) in patients with TOF. It can measure the volume and mass of the right and left ventricles and can assess the degree of pulmonary outflow tract obstruction. Finally, MRIs are important in measuring the degree of ventricular septal defect. (Somerville, 1993) | Insert MRI image here |
Hey peeps just put a intro just as a draft...tell me what you guys think of it. Edit it as you may wish.... And Jaq, if you describe briefly how each test works it would be good, regards --Z3291317 23:16, 14 September 2011 (EST)
hey jaz, ive fixed up the diagnosis, but feel free to add anything! or let me know if you think i should add anything. --z3291324 10:06, 14 September 2011 (EST) should i describe each diagnostic test!!??--z3291324 10:07, 14 September 2011 (EST)
Hey Guys! just added a very few changes, links etc to treatment. I've begun to add make a bit of notes on diagnosis that could just add a bit of detail to the diagnosis section. just wondered if any of you guys know what particular section of the ECG indicates...Left Ventricular Hypertrophy etc maybe ill call up a cardiologist :P nonetheless ill add references and some things to diagnosis tmrw night. regards, --z3291423 00:15, 14 September 2011 (EST)
Hey jaq. no particular order, the referencing system in the wiki automatically arranges it according to the order it is found in the text. In text referencing is NEEDED, lol. Type in the text title into Pubmed and when the article is found, the pmid code will be found at the bottom of the abstract for that article. if you cant figure out how to reference, put in the pubmed ids as intext citations then ill fix it for you...Make pathophys a bit more simpler, but do not compromise the anatomical words, i.e. write the anatomical word, then write in brackets what it means, eg. ...anterolaterally (at the top away from the midline) is just an example (a crap one to lol). Also did you find any new info for diagnostic tests? and Rom, why did you remove info from the 22q section???? regards --Z3291317 22:02, 13 September 2011 (EST)
hey guys, quick question about the referencing. are they in any particular order? or should i just add mine to the end of the list? and do we need to do in-text referencing?? and how do you find the pmid code? also, any suggestions on how i should improve pathophys? ie make it more anatomical based or reword it so its simpler? thanks --z3291324 21:30, 13 September 2011 (EST)
Hey Rom, looking good thus far. if you need help with referencing even after trying so much i can help you during the 1 hour we have afta the lecture tomorrow to go through and help you fix em up... its a bit tricky but can get a handle of it... --Z3291317 20:37, 12 September 2011 (EST)
Hey guys sorry for the delay, but I'm slowly uploading all my stuff up. I'm just a bit confused about how I do the reference tag thing, as you can see there is a massive red thing on our reference list. I tried copying how you guys did it but I failed at it. I'll be posting some more in the next couple of hours, I just need to get a hang of this coding thing gah! --z3290841 19:36, 12 September 2011 (EST)
hey rommel, we really need to see your part of the project and get your suggestions on parts we have done because its due on thursday --z3291324 19:16, 12 September 2011 (EST)
Hey Peeps, Just reconstucted the referencing so they are done exactly as it should be... Also just uploaded a pic of Mr fallot Himself without any copyright restrictions ( aha ow ye ow ye, took me long before i found it lol). I left the intext references jac and jaz put in their sections for future reference. Thats about it for now... Jaz i hope u liked the pics i showed you, and i hope rom is going well in his section... See yous soon... Regards --Z3291317 17:36, 11 September 2011 (EST)
update: uploaded the drawn images, took ages but its finally done :) and I've just finished the future directions :) so it should be fine to edit and look over in the next couple of days! regards --z3291423 13:16, 11 September 2011 (EST)
looking good jaz. thanks for the articles fru. ive had a quick look at them but will need to fix it up after work this arvo! --z3291324 11:59, 11 September 2011 (EST)
Hey Jac, ive got 2 articles that i will send to your email, both talk about Cardiac Magnetic Resonance, one some detail about electrocardiography. Also, Jaz i have an article that has a section based on 'Future Innovations' for TOF, have a read and i reckon it will help out with the future directions part... i will send these articles to your emails so look at them when yous can... and rom, you breathing my friend?... regards --Z3291317 01:29, 11 September 2011 (EST)
hey guys, just reworded diagnosis so it makes sense. can anyone suggest any good articles to read for diagnosis? im having trouble accessing a lot of articles (they keep asking for passwords) and a lot of the articles dont discuss diagnosis in much detail at all. help is much appreciated!! thanks :) --z3291324 21:12, 10 September 2011 (EST)
hey rom, this might be helpful for genetics. not sure what youve got already though http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2747103/ --z3291324 20:50, 10 September 2011 (EST)
also what should i do about the symptoms-pathophys overlap. should i alter the pathophys so its more anatomical like in the below article??--z3291324 20:10, 10 September 2011 (EST)
On to it now fru. thanks for the article. should i reword pathophys too so its easier to read/understand?--z3291324 20:08, 10 September 2011 (EST)
Hey Fru: in regards to the below comments, im working on future directions now :) also i read through the history section and it seems a lot more better :) just one mistake is the "durng such operations there need". Ill have my edited prognosis and futures up by tonight! :) ohh and the heart! regards --z3291423 11:03, 10 September 2011 (EST)
Hey Jac i was reading the article: Review - Tetralogy of Fallot by Frederique Bailliard and Robert H Anderson ( im sure you have this one) and theres a section absed on " Anatomical variants of Tetralogy of Fallot, and associated anomalies". i believe if you could also include this section into the Pathophysiology section it would be great! Furthermore would you please do the things Mark said in regards to your sections it would be good, especially the diagnostic tests part :). Also to everyone we need to get Future Directions and especially Genetics up ASAP! thus respective people have them completed asap. --Z3291317 22:49, 9 September 2011 (EST)
Hey jaz, the prognosis sounds pretty good. maybe expand/explain how the hypoxic spells, brain abscesses etc cause death. i think in general we could expand upon most sections. off to work now guys but ill fix up my couple of sections tonight/tomorrow morn! --z3291324 08:30, 9 September 2011 (EST)
Thanks Fru! I will definitely crack onto those suggestions, I'm going to first email the owner of the children's hospital video on youtube to get permission for using the video, and then ill put it up in my section.
ALSO, I've nearly done the picture! I've got an outline and as your reading this, i should have it coloured, labelled and ready for upload! :D
have a great weekend guys!
Reagards --z3291423 23:29, 8 September 2011 (EST)
Hey jaz just read your prognosis section. You made it well, however,i picked up 2 things you could do and it woould be good if you do them: 1. The causes of death after no surgery has done; if you can explain how these 'causes of death' occur due to TOF, it will portray the role TOF has in these problems. 2. You should talk about any complications that could arise in both patients that dont have corrected TOF and the ones who do have the surgery (i.e. any conditions that could develop after having the surgery or not, not just the death of the patient if they dont correct their heart). Other than that great work! :) --Z3291317 23:17, 8 September 2011 (EST)
Ye Jaz, thanks for the pic. Aswell ive attached a reviewed file of the treatment section on an email i sent to you. Maybe the youtube cideo based on the TOF fix up can now be put under this section as an embedded video... --Z3291317 22:19, 8 September 2011 (EST)
hey jaz, the treatment section is much better, much easier to read. thanks for the heart pic! im pretty sure my section is he one that is too "verbose" so anyone feel free to fix it up--z3291324 19:47, 8 September 2011 (EST)
Hey Guys! sorry prognosis took me a bit longer to do, but It will be up by tonight :) and ill upload the heart pic as well :) which took forever to make! regards --z3291423 16:05, 8 September 2011 (EST)
hey guys just put up some diagnosis, let me know if you want me to add anything to it. furkan, glossary looks good! rommel, how are you going with the genetics do you need any help? and jaz are you able to post up the prognosis? once they are all up we should go through and edit them all together and fix up the wording. --z3291324 15:50, 8 September 2011 (EST)
Hey peoples...im going to start constucting the glossary wordbank as i read the entire document. Please add words yous think i missed out on... Also i found a pic of Mr Fallot but i think theres copyright rights on it. i think i gotta clear it somehow...--Z3291317 19:19, 7 September 2011 (EST)
hey jaz, i think the treamtment section is alright. maybe reword the first bit into sentences (i think it was the bit on how severe the cyanosis is) so its a bit clearer. but otherwise good :) what do you think about pathophys?--z3291324 12:40, 7 September 2011 (EST)
hey guys, i cant tell if this pic has copyright or not. can someone please have a look for me? http://www.nhlbi.nih.gov/health/health-topics/topics/tof/ thanks!--z3291324 09:49, 6 September 2011 (EST)
--> REPLY: I looked at the pic and looks great. however, i couldnt see if it was copyright or not. HOWEVER, it is found on a public government website, and from what i remember Mark said we can use these materials. To make sure just please check it with him aswell. Also, im going to format your pathophysioligy section now so it looks prettier :)--Z3291317 19:19, 7 September 2011 (EST)
Hey guys, i Just finished the Treatment part, I've got palliative in this heading to still complete but Its very brief so i thought id get cracking on getting that drawing done and also the prognosis will be up by tomorrow! also check this out! http://www.nemours.org/content/dam/nemours/www/filebox/service/medical/cardiology/defect/tof.swf --z3291423 23:57, 5 September 2011 (EST) -->REPLY: Cool animation. Would we use an external link to this animation due to copyright restrictions?--Z3291317 19:19, 7 September 2011 (EST)
Hey Peepz
I just finished the sections of History, Signs and symptoms and Epidemiology
just please check these sections, especially the epidemiology one, do yous want it more detailed or is it enough?
z3291324 your section seems alright so far, show us your edited version so we can fully critic it then.
p.s. the post below my one i dont really understand itl who is speking to who and what are yous refering to? lol
Regards --Z3291317 23:44, 4 September 2011 (EST)
j: the article on future treatment directions sounds good. i might add some of the info in to the pathophysiology section because it links in well with the pulmonary stenosis and right ventricular hypertrophy. --z3291324 13:47, 2 September 2011 (EST)
I think this article makes some good points which could be added into the treatment section (eg discuss treatment/surgery after birth and also follow up treatments in adulthood- pulmonary valve replacement etc due to valvular incompetence and regurgitation because of the growing heart)
pathophysiology
hey guys. ive written some basic notes (UNEDITED) for pathophysiology. Just want to get an idea of how much detail i should go into before i start adding links to journal articles etc. can someone please have a quick look through and give me an idea of how much more detail is needed. thanks :)
The four features of tetralogy of fallot are pulmonary stenosis, overriding aorta, ventricular spetal defect and right ventricular hypertrophy. These features result from the anterosuperior displacement of the infundibular septum. The severity of symtpoms is determined by the extent of right ventricular outflow obstruction.
Pulmonary stenosis
(Symptoms include cyanosis, right ventricular hypertrophy, hepatomegaly and peripheral oedema (of the legs). More mild symptoms include sudden fainting and dizziness from exercise. )
Valvular or infundibular stenosis (narrowing of the outflow tract of the right ventricle). Obstructs the outflow of blood from the right ventricle reducing pulmonary flow. If the pulmonary stenosis is mild, a left to right shunt (with no cyanosis) will form, due to the higher pressure in the left ventricle. However, significant pulmonary stenosis can raise right ventricular pressure above the left ventricular pressure and cause a right to left shunt (cyanosis etc). The pathophysiology of pulmonary stenosis usually worsens with age because the pulmonary orifice stays the same size despite an increase in the size of the heart.
Overriding aorta
The aortic valve has a biventricular connection. Instead of being positioned over the left ventricle, the aortic valve is located above the interventricular spetal defect allowing blood from both the right and left ventricles to pass through the aortic valve. The degree to which the overriding aorta is continuous with the right ventricle determines the severity of symptoms. Because the right ventricle receieves deoxygenated blood from the systemic circulation, the percent oxygenation of bloood entering the aorta and hence back into the systemic circulation is decreased.
Ventricular septal defect
The interventricular septum dividing the left and right ventricles is incomplete at its superior, membranous end. During ventricular contraction, blood from the left ventricle passes into the right ventricle and then re-enters the pulmonary circulation. Leakage of blood from the left to right ventricle raises the right ventricular volume and pressure resulting in pulmonary hypertension. (Shortness of breath, dizziness and fainting) If the right ventricular pressure exceeds that of the left, the left to right shunt is reversed and the patient will experience cyanosis and deoxygenated blood is by-passing the lungs and entring the systemic circulation. (also breathlessness, poor feeding and failure to thrive in infancy.)
Rigth ventricular hypertrophy
Compensatory response to pulmonary stenosis ...to be contined.
--z3291324 13:38, 2 September 2011 (EST)
link to pathology textbook
hey guys, this is the link to tetralogy of fallot in robbins pathology --z3291324 13:05, 2 September 2011 (EST)
More genetics and Surgery
Hey Peeps, i forund another article in regards to Genetics as it does an genotype-phenotype anaylis os TOF Patients. Have a read and see if it can help in the assignment subsection. if you cant get the full article tell me and ill give you the pdf of it.
Article: PMID: 19948535
And Regards to surgery and its prognosis post-operation i found these articles that may be helpful for 3291423. Again if yous cant find the pdf tell me and i'll send yous the pdf articles of these.
Articles: PMID: 20091166 ; PMID: 21769263 ; PMID: 21566339 (hey 3291423 this is the article i showed you in the lab and you wanted it from me)
Anyways peeps i hope all the assignments are coming along well
Regards --Z3291317 19:03, 1 September 2011 (EST)
REPLY: Thanks z3291317, I had a look through the files and am using them now for summarising :) also, can you send through the picture of what you want the abnormal TOF heart to look like and ill get cracking on it to produce/draw it :)
regards --z3291423 22:15, 1 September 2011 (EST)
Genetics
Hey guys, found some articles relating to genetics and the deletion of the 22q11 gene. take a look :) --z3291423 21:09, 27 August 2011 (EST)
AS Bassett, EWC Chow and J Husted et al., Clinical features of 78 adults with 22q11 deletion syndrome, Am J Med Genet 138 (2005), pp. 307–313. http://pediatrics.aappublications.org.wwwproxy0.library.unsw.edu.au/content/112/1/101
http://pediatrics.aappublications.org.wwwproxy0.library.unsw.edu.au/content/112/1/101
=Treatment and
Hey guys, found this really amazing article about treatments and their repercussions http://www.ccjm.org/content/77/11/821.long#abstract-3 future directions info/readings= --z3291423 21:09, 27 August 2011 (EST)
Online lab 4 info
I my friends , colleagues and countrymen am going to be undertaking the research of the subsection Genetics/Aetiology in the topics that have been discussed. --z3290841 10:18, 25 August 2011 (EST)
Im going to be researching Treatment/Management, Prognosis & Future directions. - z3291423
regards, --z3291423 23:30, 24 August 2011 (EST)
Thanks for typing them up. I'm going to research Pathophysiology and abnormalities and diagnostic tests.
--z3291324 15:40, 24 August 2011 (EST)
Hey Group 6
From the Meeting on Tuesday after the Embryo lecture, we had concluded that we are going to divide the group project of TOF into the following sub-sections (if i am not mistaken):
- Introduction
- History
- Epidemiology
- Signs and Symptoms
- Genetics/Aetiology
- Pathopgysiology and Abnormalities
- Diagnostic Tests
- Treatment/Management
- Prognosis
- Future Directions
- Glossary
- References
From these subsections, I (z3291317) will research the History, Epidemiology and Signs & Symptoms subsections of the group Project.
Just wanted to put forward my part for the group project :)
Regards --Z3291317 15:01, 24 August 2011 (EST)
Resources
Hey Group 6
When i was looking around for info in regards to TOF, i found some videos on youtube made by an american hospital which we could use on our page in the "more info" section. Check them out and tell me what yous think...
- http://www.youtube.com/watch?v=ACRfFkxow7w - http://www.youtube.com/watch?v=jgLC2QABcxo
So what you guys think? --Z3291317 22:54, 21 August 2011 (EST)
COMMENT: great stuff! that really is a great tool, maybe we can incorporate that in as a link, or something to really explain it! without all the mumbo jumbo :) --z3291423 22:22, 22 August 2011 (EST)
Articles
Found really good article detailing some clinical aspects http://journals.cambridge.org.wwwproxy0.library.unsw.edu.au/action/displayAbstract?fromPage=online&aid=331031 its called: The clinical anatomy of tetralogy of Fallot, http://www.sciencedirect.com.wwwproxy0.library.unsw.edu.au/science/article/pii/S0140673609606577 - Tetraology of ballot by christian apitz, just google scholar it via unsw or use the link I've given you :) --z3291423 19:10, 20 August 2011 (EST)
Images
Hey guys, this is an image of tetralogy of fallot with pulmonary atresia
 --z3291324 22:07, 17 August 2011 (EST)
--z3291324 22:07, 17 August 2011 (EST)
Hey guys, just found this still frame showing large ventricular septal defect, aortic override, and right ventricular hypertrophy which are all very common to patients with ToF
 --z3291423 21:43, 17 August 2011 (EST)
--z3291423 21:43, 17 August 2011 (EST)
Hey guys this is my image of our disease, it is just outlining some of the basic changes that happens to the heart, mainly the right ventricle.

--z3290841 13:42, 17 August 2011 (EST)
Hey Group 6, its z3291317
I just wanted to make it clear that we add all new entries into our discussion page at the top of the page and not at the bottom of it. Thats how we are told to edit this discussion page.
Anyways this is my Image for Lab 3 Question 2:

I hope it would be beneficial for our page...
--Z3291317 12:05, 17 August 2011 (EST)
--Z3291317 17:00, 7 August 2011 (EST) Hey Group 6
i just done some research on a possible group project subject. It is quite detailed and interesting (to me) disease to write on.What do you guys think? Here is the review and research article for it:
The Disease:Tetralogy of Fallot
Review Article:
Orphanet J Rare Dis. 2009 Jan 13;4:2.
Tetralogy of Fallot.
Bailliard F, Anderson RH.
North Carolina Children's Heart Center, Department of Pediatrics, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA. frederique_bailliard@med.unc.edu
Link: [28]
Description: This paper gives an overview about the disease, how it happens, and clinical manifestations.
Research Article:
J Med Genet. 2010 May;47(5):321-31. Epub 2009 Nov 30.
Comprehensive genotype-phenotype analysis in 230 patients with tetralogy of Fallot.
Rauch R, Hofbeck M, Zweier C, Koch A, Zink S, Trautmann U, Hoyer J, Kaulitz R, Singer H, Rauch A.
Institute of Medical Genetics, Schorenstrasse 16, CH-8603 Zurich-Schwerzenbach, Switzerland. anita.rauch@medgen.uzh.ch
Link: [29]
Description: A study was done to see the prevalent phenotype for Tetralogy of fallot, and it was found that the 22q11.2 deletion was the most common type in Tetralogy of Fallot.
References:
- ↑ http://ghr.nlm.nih.gov/gene/TBX1
- ↑ http://ghr.nlm.nih.gov/gene/NKX2-5
- ↑ http://ghr.nlm.nih.gov/gene/JAG1
- ↑ <pubmed>11339373</pubmed>
- ↑ <pubmed>9570129</pubmed>
- ↑ <pubmed>20937753</pubmed>
- ↑ 7.0 7.1 7.2 <pubmed>19948535</pubmed>
- ↑ http://ghr.nlm.nih.gov/glossary=haploinsufficiency
- ↑ 9.0 9.1 <pubmed>1714651</pubmed>
- ↑ <pubmed>7665173</pubmed>
- ↑ <pubmed>10587520</pubmed>
- ↑ <pubmed>12427653</pubmed>
- ↑ <pubmed>9268641</pubmed>
- ↑ 14.0 14.1 <pubmed>11869892</pubmed>
- ↑ <pubmed>10556292</pubmed>
- ↑ <pubmed>11152664</pubmed>
- ↑ <pubmed>12649809</pubmed>
- ↑ http://www.chdinfo.com/aa/aa112397.htm
- ↑ http://emedicine.medscape.com/article/2035949-treatment#a1156
- ↑ http://www.chdinfo.com/aa/aa112397.htm
- ↑ <pubmed>4813185</pubmed>
- ↑ http://www.chdinfo.com/aa/aa112397.htm
- ↑ http://emedicine.medscape.com/article/2035949-treatment#a1156
- ↑ <pubmed>19683809</pubmed>
- ↑ 25.0 25.1 25.2 25.3 <pubmed>8272784</pubmed>
- ↑ Cite error: Invalid
<ref>tag; no text was provided for refs namedPMID21048055 - ↑ 27.0 27.1 <pubmed>19144126</pubmed>
- ↑ <pubmed>19144126</pubmed>
- ↑ <pubmed>19948535</pubmed>
--Z3291317 17:00, 7 August 2011 (EST)
--z3290841 09:36, 8 August 2011 (EST)
Hey Guys,
I did research on Cystic fibrosis and these are the 2 articles that I found that explains a lot about the disease, and the genetic research on it.
Review Article:
Cystic Fibrosis: Seminar
Description: This is basically outlining the pathophysiology of the disease, disease manifestation,current treatments diagnostic tool.
Ratjen F & Doring G.(2003).Cystic Fibrosis: Seminar.The Lancet, 361, 681-9. Retrieved from http://www.sciencedirect.com/science/article/pii/S0140673603125676
Research Article:
Gene expression profile study in CFTR mutated bronchial cell lines
Description: This article provides information about the severity of gene expression in relation of the extent or type of mutation.
Gambardella S, Biancolella M, D'Apice M, Amati F, Sangiuolo F, Farcomenti A, Chillemi G, Bueno S, Desideri A & Novelli G.(2006).Gene expression profile study in CFTR mutated bronchial cell lines.Clinical and Experimental Medicine , 6, 157-65. Retrieved from http://proquest.umi.com/pqdlink?Ver=1&Exp=08-05-2016&FMT=7&DID=1187181501&RQT=309&cfc=1
--z3290841 09:36, 8 August 2011 (EST)
--z3291324 20:48, 10 August 2011 (EST)
Hey guys, I like the disease that Furkan found (tetralogy of fallot)! What does everyone think?
These are the two articles I found. The review article gives a pretty good description of the disease, symptoms, treatment and complications etc. The research article looks at some of the genetic causes.
Goldmuntz, E., Geiger, E., & Benson, D. W. (2001). NKX2.5 mutations in patients with tetralogy of fallot. Circulation, 104(21), 2565-2568.
Apitz, C., Webb, G. D., & Redington, A. N. (2009). Tetralogy of Fallot. Lancet, 374(9699), 1462-1471.
Hey kiddes just done some research! check it out, its about Hypoplastic left heart syndrome
Review article:
2001 May-Jun;21(3):705-17. Hypoplastic left heart syndrome. Bardo DM, Frankel DG, Applegate KE, Murphy DJ, Saneto RP.
Link: [1]
Research:
2011 Aug 1;108(3):421-7. Epub 2011 May 31. Prenatal diagnosis of hypoplastic left heart syndrome in current era. Kipps AK, Feuille C, Azakie A, Hoffman JI, Tabbutt S, Brook MM, Moon-Grady AJ. Link: [2]
References
1. Bardo DM, Frankel DG, Applegate KE, Murphy DJ, Saneto RP ""Hypoplastic left heart syndrome.""Radiographics. 2001 May-Jun;21(3):705-17 [1]
2. Kipps AK, Feuille C, Azakie A, Hoffman JI, Tabbutt S, Brook MM, Moon-Grady AJ ""Prenatal diagnosis of hypoplastic left heart syndrome in current era."" Am J Cardiol. 2011 Aug 1;108(3):421-7. Epub 2011 May 31 [2]
Peer Assessments
- I would suggest placing the history section into a timeline or table format just so that significant dates are more clear and emphasised.
- The gene profile section was great. It was in detail, it was coherent and the inclusion of gene images enhanced my understanding of this particular section.
- Maybe for the “how the procedure works” section of the diagnostics table could have been summarised into a flow diagram or through images, rather than having a chunk of text. This could make it more straight forward to the reader.
- Your website was generally well-written and to the point. You varied your formatting regularly which made your page entertaining.
- My last suggestion would to only use the image of the shunt once and finding a different image as the repetitiveness of this is slightly disengaging
--z3332629 15:26, 22 September 2011 (EST)