Oocyte Development: Difference between revisions
| Line 22: | Line 22: | ||
[[Image:oocytenumber.jpg|500px]] | [[Image:oocytenumber.jpg|500px]] | ||
Graph based on data from Hassold, etal., 1996<ref><pubmed>8908177</pubmed></ref> | Graph based on data from Hassold, etal., 1996.<ref><pubmed>8908177</pubmed></ref> Some recent studies suggest that the number of follicles at birth maybe much lower, about 2.5 million, than the original data suggested.<ref><pubmed>20111701</pubmed></ref> | ||
==Meiosis == | ==Meiosis == | ||
Revision as of 16:10, 17 May 2011

Introduction

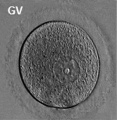
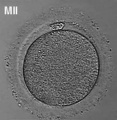
Prior to release from the ovary oocytes (eggs, ova) are arrested at an early stage of the first meiotic division as a primary oocyte (primordial follicle). Following purberty, during each menstrual cycle, pituitary gonadotrophin stimulates completion of meiosis 1 the day before ovulation. Early oocytes are also classified as immature (germinal vesicle (GV) or metaphase I (MI) stage). The breakdown of the germinal vesicle indicates a resumption of meiosis and the extrusion of the first polar body (1 PB) indicates completion of the first meiotic division in human oocytes.
In an adult human female the development of a primordial follicle containing an oocyte to a preovulatory follicle takes in excess of 120 days.
| Menstrual Cycle | In Vitro Fertilization
Oogenesis
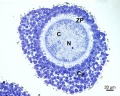
A human infant ovary histology, showing the large number of oocytes occupying the ovary cortical region. Compare this with a mature ovary and note the absence of any follicle development in the infant. These early oocytes remain at the diplotene stage of the meiosis I during development from fetal life and postnatal childhood, until puberty when the lutenizing hormone (LH) surges stimulate the resumption of meiosis.

The graph below shows the changes in human germ cell numbers in the ovary with age, peaking at about 7 million (occuring in early fetal development) and then decreasing by apopotic cell death. At puberty there remain only about 400,000 and only about 10% of these will be released through reproductive life. (More? Menstrual Cycle)

Graph based on data from Hassold, etal., 1996.[1] Some recent studies suggest that the number of follicles at birth maybe much lower, about 2.5 million, than the original data suggested.[2]
Meiosis

In females, the total number of eggs ever to be produced are present in the newborn female initially arrested at the diplotene stage of the meiosis I from fetal life through childhood until puberty, when the lutenizing hormone (LH) surges stimulate the resumption of meiosis.
- All eggs are arrested at an early stage (prophase I) of the first meiotic division as a primary oocyte (primordial follicle). Following purberty, during each menstrual cycle, pituitary gonadotrophin stimulates completion of meiosis 1 the day before ovulation.
- In meiosis 1, a diploid cell becomes 2 haploid (23 chromosomes) daughter cells, each chromosome has two chromatids. One cell becomes the secondary oocyte the other cell forms the first polar body.
- The secondary oocyte then commences meiosis 2 which arrests at metaphase and will not continue without fertilization.
- At fertilization meiosis 2 completes, forming a second polar body. Note that the first polar body may also undergo this process forming a third polar body.

- Links: Cell Division - Meiosis
Polar Body

The breakdown of the germinal vesicle indicates a resumption of meiosis and the extrusion of the first polar body (1 PB) indicates completion of the first meiotic division in human oocytes. The polar body is a small cytoplasmic exclusion body formed to enclose the excess DNA formed during the oocyte (egg) meiosis and following sperm fertilization. There are 2-3 polar bodies derived from the oocyte present in the zygote, the number is dependent upon whether polar body 1 (the first polar body formed during meiosis 1) divides during meiosis 2. This exclusion body contains the excess DNA from the reductive division (the second and third polar bodies are formed from meiosis 2 at fertilization). These polar bodies do not contribute to the future genetic complement of the zygote, embryo or fetus.
Recent research in some species suggest that the space formed by the peripheral polar body (between the oocyte and the zona pellucia) can influence the site of spermatozoa fertilization.
Assisted reproductive techniques involving intracytoplasmic sperm injection (ICSI) have looked at the "quality" of the polar body and found that the morphology is related to mature oocyte viability and has the potential to predict oocyte fertilization rates and pregnancy achievement.[3][4]
Abnormalities

Meiotic non-disjunction resulting in aneuploidy, most are embryonic lethal and not seen. The potential for genetic abnormalities increase with maternal age.
- Autosomal chromosome aneuploidy
- trisomy 21 - Down syndrome
- trisomy 18 - Edwards syndrome
- trisomy 13 - Patau syndrome
- Sex chromosome aneuploidy
- monosomy X - Turner's Syndrome
- trisomy X - Triple-X syndrome
- 47 XXY - Klinefelter's Syndrome
Oocyte-Follicle cell Interaction
The oocyte and the surrounding granulosa cells have a complex paracrine interactions during follicle growth and development. Oocyte maturation has been shown to depend on secretory products of both the granulosa and cumulus cells.
Oocyte Factors
- promotes granulosa cell proliferation in preantral and antral follicles (GDF-9, BMP15)
- cumulus expansion and granulosa cell differentiation are dependent upon oocyte-derived factors
- BMP15 inhibits FSH-stimulated progesterone production
Oocyte Protein Expression


The table above shows the pattern of protein expression (as percentages of total) in the mouse germinal vesicle and MII oocyte according to 14 molecular function categories.[5]
- Links: Germinal vesicle oocyte protein expression | MII oocyte protein expression | Zygote Protein Expression | Mouse Development | Oocyte Development | Zygote
Additional Images
Human oocyte

Human oocyte metaphase I
Human oocyte metaphase II

Historic drawing human

Historic photo human
- Monkey-ovary x20he.jpg
Monkey

Mouse

Mouse
Canine (dog)

Canine (dog)
Salamander







{kind=link}
References
Search
- NCBI Bookshelf oocyte | oogenesis | oocyte development
- Pubmed oocyte | oogenesis | oocyte development
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, April 16) Embryology Oocyte Development. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Oocyte_Development
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G