Musculoskeletal System - Abnormalities
| Embryology - 19 Apr 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Introduction

There are a large number of different musculoskeletal abnormalities affecting one or a combination of bone and muscle development in the skull, trunk and limbs. This page therefore can only broadly introduce the topic and link to other resources with more specific information.
Musculoskeletal and limb disorders together form the largest group of congenital defects that occur in Australia. The three most commonly occurring are developmental dysplasia of the hip, cleft palate, cleft lip and palate.
Some defects appear as obvious malformations, such as syndactyly and limb reductions. Other muscular defects only become obvious postnatally when the muscles are required to be used, those in highest use are respiratory (diaphragm, intercostals) and anti-gravity (those that hold you upright) muscles.
International Classification Diseases - Musculoskeletal
Some Recent Findings
|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Congenital Musculoskeletal Abnormalities <pubmed limit=5>Congenital+Musculoskeletal+Abnormalities</pubmed> |
Australian Statistics

The ten most frequently reported birth defects in Victoria between 2003-2004.
- Hypospadias
- Obstructive Defects of the Renal Pelvis or Obstructive Genitourinary Defects
- Ventricular Septal Defect
- Congenital Dislocated Hip
- Trisomy 21 or Down syndrome
- Hydrocephalus
- Cleft Palate
- Trisomy 18 or Edward Syndrome - multiple abnormalities of the heart, diaphragm, lungs, kidneys, ureters and palate 86% discontinued.
- Renal Agenesis/Dysgenesis - reduction in neonatal death and stillbirth since 1993 may be due to the more severe cases being identified in utero and being represented amongst the increased proportion of terminations (approximately 31%).
- Cleft Lip and Palate - occur with another defect in 33.7% of cases.
Developmental Dysplasia of the Hip

Also called Congenital Hip Dislocation.
- Instability: 1:60 at birth; 1:240 at 1 wk: Dislocation untreated; 1:700
- congenital instability of hip, later dislocates by muscle pulls or gravity
- familial predisposition female predominance
- Growth of femoral head, acetabulum and innominate bone are delayed until the femoral head fits firmly into the acetabulum.
International Classification of Diseases
Q65 Congenital deformities of hip
- Q65.0 Congenital dislocation of hip, unilateral
- Q65.1 Congenital dislocation of hip, bilateral
- Q65.2 Congenital dislocation of hip, unspecified
- Q65.3 Congenital subluxation of hip, unilateral
- Q65.4 Congenital subluxation of hip, bilateral
- Q65.5 Congenital subluxation of hip, unspecified
- Q65.6 Unstable hip Dislocatable hip Subluxatable hip
- Q65.8 Other congenital deformities of hip Anteversion of femoral neck Congenital acetabular dysplasia Congenital coxa: valga vara
- Q65.9 Congenital deformity of hip, unspecified
Barlow test
(Barlow maneuver) A clinical term to describe a physical examination of the newborn for Developmental dysplasia of the hip (DDH). The examiner adducts the hip (bringing the thigh towards the midline) while applying light pressure on the knee, directing the force posteriorly. A positive sign is the hip being dislocatable, if the hip can be popped out of socket with this test. This test is then combined with the Ortolani test (maneuver). The test is named after Thomas Barlow (1845 – 1945) a British royal physician.
Ortolani test
(Ortolani manoeuvre) A clinical term to describe a physical examination of the newborn for developmental dysplasia of the hip (DDH). This is a test for posterior dislocation of the hip. Using the examiner's thumb, abduct the infant's leg, while using the examiner's index finger to place anterior pressure on the greater trochanter. A positive sign is a distinctive 'clunk' which can be heard and felt as the femoral head relocates anteriorly into the acetabulum, usually becomes negative after 2 months of age. This test is combined with the Barlow test (manoeuvre). Named after Marino Ortolani, the test developer in 1976.
Abduction Splints
There is variable evidence for the use of abduction splinting during onset of walking in children on the maturation of mild dysplastic hips.[4]
Scoliosis


International Classification of Diseases
Q67 Congenital musculoskeletal deformities of head, face, spine and chest - Q67.5 Congenital deformity of spine Congenital scoliosis: NOS postural Excl.: infantile idiopathic scoliosis (M41.0) scoliosis due to congenital bony malformation (Q76.3)


- frequency of congenital scoliosis is approximately 0.5, or 1 in 1,000 births.
- assymetric growth impairment of vertebral bodies
- lateral deviation of spine (Lateral flexion, Forward flexion, Rotation of vertebral column on long axis)
- compensated by movement of vertebral column above and below affected region (producing a primary and two secondary curves)
- progresses rapidly in adolescence and becomes fixed once bone growth is completed.
- both genetic and environmental terartogens implicated.
- a large number of chromosomal deletions relating to regions 2p13 – 15, 6q13 and 15q12 have been identified.
Chêneau's Brace

Dr. Chêneau fabricated the original "Chêneau Brace" in 1979 and is commonly used for the treatment of scoliosis and thoracic hypokyphosis in some European countries, though not commonly in either North America or the United Kingdom. The brace corrects by a system of multipoint pressure zones and expansion chambers.
Harrington Rod
Dr Paul Harrington, a USA orthopaedic surgeon, in 1953 designed the "Harrington implant", the first modern spinal instrumentation system that produced both correction and immobilization. This historic system has now been replaced by more modern systems.
- Links: Axial Skeleton Development
Muscle Development
There can be abnormalities associated directly with muscle differentiation and function as well as those mediated indirectly by abnormalities of innervation or skeletal development and other associated systems.
Duchenne Muscular Dystrophy
The most common occuring in Boys and in Duchenne Muscular Dystrophy (DMD). This cause of the disease was discovered in 1988 as a mutation in dystrophin, a protein that lies under the muscle fiber membrane and maintains the cell's integrity. As skeletal muscles have little prenatal load or use it is not until postnatally that muscle wasting occurs, usually in the anti-gravity muscles first. This is a progressive disease usually detected between 3-5 years old.
- X-linked dystrophy
- large gene encoding cytoskeletal protein - Dystrophin
- progressive wasting of muscle, die late teens
Becker Muscular Dystrophy
A milder adult (30-40 years old) onset form of the disease Becker's Muscular Dystrophy (BMD) that involves mutations in the same dystrophin gene.
Autosomal Recessive Muscular Dystrophy
Dystroglycan, a protein that associates with both dystrophin and membrane molecules, is a candidate gene for the site of the mutation in autosomal recessive muscular dystrophies. A knockout mouse has been generated that has early developmental abnormalities.
Myotonic Dystrophy
An inherited disorder in which the muscles contract but have decreasing power to relax. With this condition, the muscles also become weak and waste away. The myotonic dystrophy gene, found on chromosome 19, codes for a protein kinase that is found in skeletal muscle, where it likely plays a regulatory role. The disease is "amplified" through generations probably by a similar GC expansion associated with Huntington disease.
Facioscapulohumeral Muscular Dystrophy
(FSHD) This form of muscular dystrophy is an autosomal dominant genetic disorder characterized by progressive muscle weakness and wasting that typically begins in the face, shoulder-girdle and upper arm. Currently thought to relate to an impaired muscle regeneration process.
- Links: skeletal muscle
Spinal Muscular Atrophy
ICD-11 8B61 Spinal muscular atrophy (ICD-10-CM Diagnosis Code G12.9)
Spinal muscular atrophy (SMA) is a rare neural genetic condition that leads to a loss of motor neurons and then progressive muscle wasting. The disease exists in several different forms: Type 1, Type 2, and Type 3a SMA. A new drug treatment using nusinersen (trade name Spinraza®) has led to the inclusion of SMA in the newborn heel-prick test (Guthrie test).
- Links: spinal cord
Limb Abnormalities
Genetic

- Human Gene Mutations - mutation of any of the patterning genes will result in limb abnormalities (Will put Table on Web page mutations and terminology)
Type II syndactyly- HoxD13
Maternal
- thalidomide Phocomelia
- short ill-formed upper or lower limbs
- hyperthermia
Syndactyly

Fusion of fingers or toes which may be single or multiple and may affect: skin only, skin and soft tissues or skin, soft tissues and bone.
The condition is unimportant in toes but disabling in fingers and requires operative separation and is frequently inherited as an autosomal dominant.
The presence of this additional "webbing" reflects preservation of the developmental tissues that in normal development are removed by programmed cell death (apotosis).
Polydactyly

Presence of additional toes or fingers also called polydactylia or polydactylism. The condition is often treated surgically in the infant.
Ernest Hemingway in the 1930's had a six-toed cat (Snowball) showing a form of polydactyly and cats with a similar condition are now called "Hemingway cats".
(More? Limb Development Abnormalities - Polydactyly)
Polysyndactyly
Developmental abnormality where there is a combination of polydactyly with syndactyly is known as polysyndactyly.
Triphalangeal Thumb (TPT)
|
Developmental abnormality with three phalanges instead of two, forming a long, finger-like thumb. Usually inherited as an autosomal dominant trait, gene locus chromosome region 7q36. |

Calcaneovalgus
- Occurs in about 5% of all newborns.
- Females are affected more often than males.
- Deformity can be unilateral or bilateral.
- external rotation of the calcaneus.
- an overstretched Achilles tendon.
- tight anterior leg musculature.
See the review "The Newborn Foot" (2004).[7]
Gastroschisis
By definition, it is a body wall musculoskeletal defect, not a gastrointestinal tract defect, which in turn impacts upon GIT development.
| Gastroschisis (paraomphalocele, laparoschisis, abdominoschisis, abdominal hernia) is an abdominal wall defect associated with evisceration of the intestine (2.5 cases/10,000 births), occuring more frequently in young mothers (less than 20 years old). There have been reports that this abnormality is increasing in incidence.
The abnormality is usually situated to the right of the umbilicus and abdominal contents, mainly gastrointestinal, are found outside the anterior body wall. International Classification of Diseases, 9th Revision diagnosis (756.79) and procedure (54.71) code for gastroschisis (2003 to 2008). |

|
| Can occur in isolation and also in association with other gastrointestinal anomalies (intestinal atresia, perforation, necrosis or volvulus). Defects in other organ systems have been reported in up to 35% of children. There are several theories as to the cause of this abdominal wall defect, including recently failure of the yolk sac and related vitelline structures to be incorporated into the umbilical stalk.[8]
The condition can often be detected by ultrasound scan. Reported as a high mortality defect, only 60% of children survive until the end of the first year of age. |
|
Gastroschisis patients are commonly small for gestational age (SGA, birth weight < 10th centile). Frequency line graphs of the birth weight distribution, Kolmogorov-Smirnov test confirmed that this difference was significant (p < 0.001).[9]
|

|
Gastroschisis Classification
There has been a recent attempt to classify gastroschisis in order to measure clinical outcomes.[10]
- Simple gastroschisis - intact continuous bowel that is not compromised or breached at delivery or presentation
- Complex gastroschisis - presence of one or more of intestinal atresia, perforation or intestinal necrosis at delivery or presentation, or missed atresia
- Links: Gastrointestinal Tract - Gastroschisis | Ultrasound movie - Gastroschisis | UCSF Childrens Hospital - Gastroschisis | Brown University Image Bank- Abdominal Wall Defects
Inguinal Hernia
Inguinal hernias are more common in males and associated with the fetal/neonatal developmental descent of the testis through the abdominal wall. The following graphs are from a study of Danish data on postnatal hernia repairs[11]. In contrast, femoral hernia repairs occur mainly in adults in both sexes and increases with age.


|

|
| Inguinal hernia repair | Femoral hernia repair |
- Links: genital abnormalities
References
- ↑ Osborn DPS. etal; Mutations in INPP5K cause a form of congenital muscular dystrophy overlapping Marinesco-Sjögren syndrome and dystroglycanopathy. (2017) The American Journal of Human Genetics http://www.cell.com/ajhg/fulltext/S0002-9297(17)30019-8 Published online: February 9, 2017
- ↑ Chotigavanichaya C, Leurmsumran P, Eamsobhana P, Sanpakit S & Kaewpornsawan K. (2012). The incidence of common orthopaedic problems in newborn at Siriraj Hospital. J Med Assoc Thai , 95 Suppl 9, S54-61. PMID: 23326983
- ↑ Pannier S, Mugniery E, Jonquoy A, Benoist-Lasselin C, Odent T, Jais JP, Munnich A & Legeai-Mallet L. (2010). Delayed bone age due to a dual effect of FGFR3 mutation in Achondroplasia. Bone , 47, 905-15. PMID: 20673820 DOI.
- ↑ 4.0 4.1 Windhagen H, Thorey F, Kronewid H, Pressel T, Herold D & Stukenborg-Colsman C. (2005). The effect of functional splinting on mild dysplastic hips after walking onset. BMC Pediatr , 5, 17. PMID: 15958160 DOI.
- ↑ Postema SG, van der Sluis CK, Waldenlöv K & Norling Hermansson LM. (2012). Body structures and physical complaints in upper limb reduction deficiency: a 24-year follow-up study. PLoS ONE , 7, e49727. PMID: 23226218 DOI.
- ↑ Zaborowska-Sapeta K, Kowalski IM, Kotwicki T, Protasiewicz-Fałdowska H & Kiebzak W. (2011). Effectiveness of Chêneau brace treatment for idiopathic scoliosis: prospective study in 79 patients followed to skeletal maturity. Scoliosis , 6, 2. PMID: 21266084 DOI.
- ↑ Gore AI & Spencer JP. (2004). The newborn foot. Am Fam Physician , 69, 865-72. PMID: 14989573
- ↑ Stevenson RE, Rogers RC, Chandler JC, Gauderer MW & Hunter AG. (2009). Escape of the yolk sac: a hypothesis to explain the embryogenesis of gastroschisis. Clin. Genet. , 75, 326-33. PMID: 19419415 DOI.
- ↑ Payne NR, Simonton SC, Olsen S, Arnesen MA & Pfleghaar KM. (2011). Growth restriction in gastroschisis: quantification of its severity and exploration of a placental cause. BMC Pediatr , 11, 90. PMID: 22004141 DOI.
- ↑ Molik KA, Gingalewski CA, West KW, Rescorla FJ, Scherer LR, Engum SA & Grosfeld JL. (2001). Gastroschisis: a plea for risk categorization. J. Pediatr. Surg. , 36, 51-5. PMID: 11150437 DOI.
- ↑ Burcharth J, Pedersen M, Bisgaard T, Pedersen C, Rosenberg J Nationwide Prevalence of Groin Hernia Repair PLoS ONE 8(1): e54367. doi:10.1371/journal.pone.0054367 (2013) PLoS ONE
Journals
- Scoliosis - the official journal of the Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) and affiliated with the International Research Society of Spinal Deformities (IRSSD), is ready to receive manuscripts on all aspects of the prevention, control, and treatment of scoliosis and other spinal deformities.
- BMC Musculoskeletal Disorders is an open access journal publishing original peer-reviewed research articles in all aspects of the prevention, diagnosis and management of musculoskeletal and associated disorders, as well as related molecular genetics, pathophysiology, and epidemiology.
Reviews
Perronnet C & Vaillend C. (2010). Dystrophins, utrophins, and associated scaffolding complexes: role in mammalian brain and implications for therapeutic strategies. J. Biomed. Biotechnol. , 2010, 849426. PMID: 20625423 DOI.
Le Rumeur E, Winder SJ & Hubert JF. (2010). Dystrophin: more than just the sum of its parts. Biochim. Biophys. Acta , 1804, 1713-22. PMID: 20472103 DOI.
Lapidos KA, Kakkar R & McNally EM. (2004). The dystrophin glycoprotein complex: signaling strength and integrity for the sarcolemma. Circ. Res. , 94, 1023-31. PMID: 15117830 DOI.
Gore AI & Spencer JP. (2004). The newborn foot. Am Fam Physician , 69, 865-72. PMID: 14989573
Articles
Singh SM, Kongari N, Cabello-Villegas J & Mallela KM. (2010). Missense mutations in dystrophin that trigger muscular dystrophy decrease protein stability and lead to cross-beta aggregates. Proc. Natl. Acad. Sci. U.S.A. , 107, 15069-74. PMID: 20696926 DOI.
Norwood FL, Sutherland-Smith AJ, Keep NH & Kendrick-Jones J. (2000). The structure of the N-terminal actin-binding domain of human dystrophin and how mutations in this domain may cause Duchenne or Becker muscular dystrophy. Structure , 8, 481-91. PMID: 10801490
Search PubMed
Search April 2010
- Musculoskeletal System Development - All (44637) Review (5065) Free Full Text (6601)
- Musculoskeletal Development - All (44637) Review (5065) Free Full Text (6601)
Search Pubmed: musculoskeletal system abnormalities
Additional Images

Adult axial skeleton
Adult appendicular skeleton

Bone structure
Developing vertebra

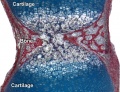
Endochondral bone

Fetal head lateral (12 weeks)
Fetal head medial (12 weeks)

Fetal head section (12 weeks)








External Links
External Links Notice - The dynamic nature of the internet may mean that some of these listed links may no longer function. If the link no longer works search the web with the link text or name. Links to any external commercial sites are provided for information purposes only and should never be considered an endorsement. UNSW Embryology is provided as an educational resource with no clinical information or commercial affiliation.
- Scoliosis - the official journal of the Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) and affiliated with the International Research Society of Spinal Deformities (IRSSD).
- Young Women's Health - scoliosis
- Scoliosis Australia
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, April 19) Embryology Musculoskeletal System - Abnormalities. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Musculoskeletal_System_-_Abnormalities
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G