Gastrointestinal Tract Development
| Embryology - 19 Apr 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Introduction


The gastrointestinal tract (GIT) arises initially during the process of gastrulation from the endoderm of the trilaminar embryo (week 3) and extends from the buccopharyngeal membrane to the cloacal membrane. The tract and associated organs later have contributions from all the germ cell layers.
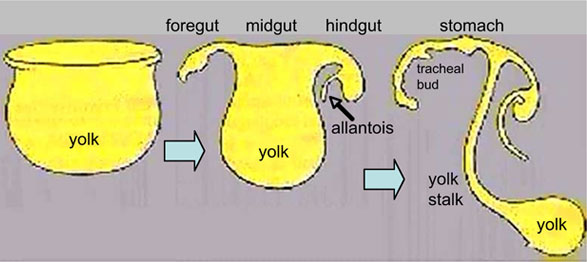
During the 4th week three distinct regions (fore-, mid- and hind-gut) extend the length of the embryo and will contribute different components of the GIT. The large mid-gut is generated by lateral embryonic folding which "pinches off" a pocket of the yolk sac, the 2 compartments continue to communicate through the vitelline duct.
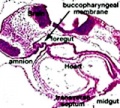
The oral cavity (mouth) is formed following breakdown of the buccopharyngeal membrane (oropharyngeal or oral membrane) and contributed to mainly by the pharynx lying within the pharyngeal arches (More? Head Development). Loss of buccopharyngeal membrane opens the tract to amniotic fluid through the remainder of development, and during the fetal period is actively swallowed.
From the oral cavity the next portion of the foregut is initially the pharynx, a single gastrointestinal (oesophagus{{) and respiratory (trachea) common tube, that lies behind the heart. Note that the respiratory tract will form from a ventral bud arising at this level (More? respiratory).
This current page provides an introductory overview, use the links below for descriptions of specific components and regions as well as developmental abnormalities.
Note that in historic texts the term entoderm is used to describe endoderm and other terminology may also differ from current descriptions.
Some Recent Findings
|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Gastrointestinal Tract Embryology | Gastrointestinal Tract Development |
| Older papers |
|---|
| These papers originally appeared in the Some Recent Findings table, but as that list grew in length have now been shuffled down to this collapsible table.
See also the Discussion Page for other references listed by year and References on this current page.
|
Textbooks
- Human Embryology Larson Chapter 9 p229-260
- The Developing Human: Clinically Oriented Embryology (6th ed.) Moore and Persaud Chapter 12 p271-302
- Before We Are Born (5th ed.) Moore and Persaud Chapter 13 p255-287
- Essentials of Human Embryology Larson Chapter 9 p123-146
- Human Embryology Fitzgerald and Fitzgerald Chapter 19,20 p119-123
More? References | Online Textbooks | Historic Textbooks
| UNSW Students | |||||||
|---|---|---|---|---|---|---|---|
|
|
You have access the following online Embryology resources and textbooks through the UNSW Library. | ||||||

|
Hill, M.A. (2020). UNSW Embryology (20th ed.) Retrieved April 19, 2024, from https://embryology.med.unsw.edu.au
| ||||||

|
Moore, K.L., Persaud, T.V.N. & Torchia, M.G. (2015). The developing human: clinically oriented embryology (10th ed.). Philadelphia: Saunders. (links only function with UNSW connection)
Chapter 11 Alimentary System
| ||||||

|
Schoenwolf, G.C., Bleyl, S.B., Brauer, P.R., Francis-West, P.H. & Philippa H. (2015). Larsen's human embryology (5th ed.). New York; Edinburgh: Churchill Livingstone.(links only function with UNSW connection)
Chapter 14 Development of the Gastrointestinal Tract
| ||||||


Objectives
- Understanding of germ layer contributions to the early gastrointestinal tract (GIT)
- Understanding of the folding of the GIT
- Understanding of three main GIT embryonic divisions
- Understanding of associated organ development (liver, pancreas, spleen)
- Brief understanding of mechanical changes (rotations) during GIT development
- Brief understanding of gastrointestinal abnormalities
Germ Layer Contributions
- Endoderm - epithelium and associated glands
- Mesoderm (splanchnic) - mesentry, connective tissues, smooth muscle, blood vessels
- Ectoderm (neural crest) - enteric nervous system (neural tube) - extrinsic innervation
Both endoderm and mesoderm will contribute to associated organs.
Gastrointestinal Tract Movies
| Gastrointestinal Tract Movies | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
| |||||||||||||||
|
|
|
|
| |||||||||||||||
|
|
|
|
| |||||||||||||||
| Stage 13 (week 5) | Stage 22 (week 8) | Stage 23 (week 8) | GIT Abnormalities Ultrasound | ||||||||||||||||

Gastrointestinal Tract Divisions

During the 4th week the 3 distinct divisions (foregut, Midgut and hindgut) extend the length of the embryo from oral membrane to cloacal membrane and will contribute different components of the GIT. These 3 divisions are also later anatomically defined by the vascular (artery) supply to each of theses divisions.
The large mid-gut is generated by lateral embryonic folding which "pinches off" a pocket of the yolk sac, the 2 compartments continue to communicate through the vitelline duct.
The oral cavity (mouth) is formed following breakdown of the buccopharyngeal membrane (oropharyngeal, oral membrane) and contributed to mainly by the pharynx lying within the pharyngeal arches. The opening of the GIT means that it contains amniotic fluid, which is also swallowed later in development.
Foregut

First embryonic division of gastrointestinal tract, extending from the oral (buccopharyngeal) membrane and contributing oesophagus, stomach, duodenum (to bile duct opening), liver, biliary apparatus (hepatic ducts, gallbladder, and bile duct), and pancreas. The forgut blood supply is the celiac artery (trunk) excluding the pharynx, lower respiratory tract, and most of the oesophagus.
From the oral cavity the next portion of the foregut is initially a single gastrointestinal (oesophagus) and respiratory (trachea) common tube, the pharynx which lies behind the heart. Note that the respiratory tract will form from a ventral bud arising at this level.
- Oral cavity
- Pharynx (esophagus, trachea)
- Respiratory tract
- Stomach
Midgut

The middle embryonic division of gastrointestinal tract contributing the small intestine (including duodenum beneath distal bile duct opening), cecum, appendix, ascending colon, and part of the transverse colon (right half to two thirds). The midgut blood supply is the superior mesenteric artery.
Much of the midgut is herniated at the umbilicus external to the abdomen through development. A key step in development is the rotation of this midgut that must occur to place the GIT in the correct abdominal position with its associated mesentry. The GIT itself differentiates to form significantly different structures along its length: oesophagus, stomach, duodenum, jejunum, ilium (small intestine), colon (large intestine).
The mesenteries of the GIT are generated from the common dorsal mesentery, with the ventral mesentry contributing to the lesser omentum and falciform ligament.
Note the duodenum is commonly divided into 4 anatomical sequential parts (superior, descending, horizontal, ascending).
Hindgut
The final embryonic division of gastrointestinal tract consisting initially of the cloaca snd extending to the cloacal membrane. The hindgut contributes part of the transverse colon (left half to one third), descending colon, sigmoid colon, rectum, part of anal canal (superior), urinary epithelium (bladder and most urethra).
The initial cloaca space will later become partitioned by a septum into a dorsal gastrointestinal component (rectum) and ventral urogenital sinus (renal/genital component).
Development Overview
GIT shown in green anchored by dosal and ventral mesogastrium. The space ouside this will be the peritoneal cavity.
Red ring - neural tube with neural crest Blue ring - notocord Orange - somites
Differentiation of associated organs at the level of the forming stomach occurs both dorsally (spleen) and ventrally (liver).
Large blue ring - dorsal aorta Dark green ring - liver
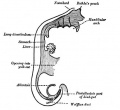
Continued growth of the GIT and the organs leads to organ movements and bending of tract.
Carnegie stage 13 Embryo Overview
Below is an overview of the sections starting at the level of pharynx compressed dorsoventrally, following the GIT through to the rectum. The most obvious feature is that of a continuous tube initially, attached by dorsoventral mesentry. Outside this tube and mesentry (at the levels below the lung buds) is the intraembryonic coelom that will form the peritoneal cavity. The hepatic diverticulum (liver bud) lies under the septum transversum is the earliest associated GIT organ that has differentiated, and now occupies a substantial region of the abdomen. Clicking on sections below will open the original images.

| |||
| Bifurcation of the pharynx into anterior respiratory and posterior oesophagous. | The stomach forming beneath the lung buds and adjacent to the developing liver. | Below the stomach the GIT has a large dorsal mesogastrium and finer ventral mesogastrium. Associated with the tract is the large portal blood vessel derived from the vitelline circulation. | At the bottom curvature of the embryo the mesentry association with the GIT shows extensive vitelline vessels running out through the umbilicus. The hindgut can then be seen, ending at the common urogenital sinus, the cloaca. |
Innervation

The gastrointestinal tract has both intrinsic and extrinsic innervation. (see the recent review[6])
- The intrinsic innervation, the enteric plexus, is derived from neural crest cells migrating into and along the wall of the gastrointestinal tract.
- mainly vagal region neural crest - generating both neurons and glia.
- some sacral neural crest - in chicken.[7]
- The extrinsic innervation occurs by efferent and afferent nerves, from the vagus and sympathetic chain and pelvic nerves.
- Vagus - sensory and motor fibers project from oesophagus to small intestine.
- Sympathetic and parasympathetic - lower oesophagus to large intestine.
- Pelvic nerves - large intestine, rectum.
| Myenteric plexus | Submucosal plexus |
|---|---|
| Auerbach's plexus | Meissner's plexus |
| Leopold Auerbach (1828–1897) a German anatomist and neuropathologist. | Georg Meissner (1829–1905) a German anatomist and physiologist. |
|
|
| Links: enteric nervous system | intestine | neural crest | PMID 25428846 |
Neural History
- 1857 Meissner was the first to describe a nerve plexus in the submucosa of the bowel wall.
- 1864 Auerbach described the myenteric plexus between the longitudinal and circular muscle layers.
- 1981 LeDouarin describes neural crest contribution to both plexuses.
Myenteric Plexus
- Peristalsis
- Coordinated waves of descending inhibition followed by waves of descending excitation
+ Extrinsic parasympathetic cholinergic nerves (vagal and sacral) excite peristalsis and stimulate
- Sympathetic noradrenergic nerves inhibit the transit of gut contents
Submucosal Plexus
- epithelial movements
- secretion and absorption
- Links: neural crest
Associated Organs

The early tract develops as a simple tube, then a number of endodermal outgrowths from this tube at different levels and contribute to a range of additional organs and tissues. The gastrointestinal associated organs liver, gall bladder and pancreas. Development of these organs is described on separate pages.
There are also a number of additional non-gastrointestinal structures including the respiratory tract and development within the mesentery such as the spleen.
Gastrointestinal Tract Abnormalities
Only a brief description is given on this current page, for more details see Gastrointestinal Tract - Abnormalities.
Lumen Abnormalities
There are several types of abnormalities that impact upon the continuity of the gastrointestinal tract lumen.
- Atresia - interuption of the lumen (esophageal atresia, duodenal atresia, extrahepatic biliary atresia, anorectal atresia)
- Stenosis - narrowing of the lumen (duodenal stenosis, pyloric stenosis).
- Duplication - incomplete recanalization resulting in parallel lumens, this is really a specialized form of stenosis.
Meckel's Diverticulum
This GIT abnormality is a very common and results from improper closure and absorption of the omphalomesenteric duct (vitelline duct) in development. This transient developmental duct connects the yolk to the primitive GIT.
Intestinal Malrotation

- Links: Intestinal Malrotation
Intestinal Aganglionosis
(intestinal aganglionosis, Hirschsprung's disease, aganglionic colon, megacolon, congenital aganglionic megacolon, congenital megacolon) A condition caused by the lack of enteric nervous system (neural ganglia) in the intestinal tract responsible for gastric motility (peristalsis).
Gastroschisis
Gastroschisis (omphalocele, paraomphalocele, laparoschisis, abdominoschisis, abdominal hernia) is a congenital abdominal wall defect which results in herniation of fetal abdominal viscera (intestines and/or organs) into the amniotic cavity. Incidence of gastroschisis has been reported at 1.66/10,000, occuring more frequently in young mothers (less than 20 years old).
By definition, it is a body wall musculoskeletal defect, not a gastrointestinal tract defect, which in turn impacts upon GIT development.
Molecular
The endoderm of the developing gastrointestinal tract is a source for patterning signals for both within the tract and also for the surrounding organs and tissues.
- Sox2 - expressed in the anterior part of the primitive gut[8]
- Cdx2 - expressed in the posterior part of the primitive gut[8]
- GDNF - regulate migration of enteric neural crest cells[9]
- endothelin - regulate migration of enteric neural crest cells[9]
References
- ↑ Niu X, Liu L, Wang T, Chuan X, Yu Q, Du M, Gu Y & Wang L. (2020). Mapping of extrinsic innervation of the gastrointestinal tract in the mouse embryo. J. Neurosci. , , . PMID: 32690615 DOI.
- ↑ Davis A, Amin NM, Johnson C, Bagley K, Ghashghaei HT & Nascone-Yoder N. (2017). Stomach curvature is generated by left-right asymmetric gut morphogenesis. Development , 144, 1477-1483. PMID: 28242610 DOI.
- ↑ Ueno S, Yamada S, Uwabe C, Männer J, Shiraki N & Takakuwa T. (2016). The Digestive Tract and Derived Primordia Differentiate by Following a Precise Timeline in Human Embryos Between Carnegie Stages 11 and 13. Anat Rec (Hoboken) , 299, 439-49. PMID: 26995337 DOI.
- ↑ Vestentoft PS, Jelnes P, Hopkinson BM, Vainer B, Møllgård K, Quistorff B & Bisgaard HC. (2011). Three-dimensional reconstructions of intrahepatic bile duct tubulogenesis in human liver. BMC Dev. Biol. , 11, 56. PMID: 21943389 DOI.
- ↑ Dames P, Puff R, Weise M, Parhofer KG, Göke B, Götz M, Graw J, Favor J & Lechner A. (2010). Relative roles of the different Pax6 domains for pancreatic alpha cell development. BMC Dev. Biol. , 10, 39. PMID: 20377917 DOI.
- ↑ Uesaka T, Young HM, Pachnis V & Enomoto H. (2016). Development of the intrinsic and extrinsic innervation of the gut. Dev. Biol. , 417, 158-67. PMID: 27112528 DOI.
- ↑ Burns AJ, Champeval D & Le Douarin NM. (2000). Sacral neural crest cells colonise aganglionic hindgut in vivo but fail to compensate for lack of enteric ganglia. Dev. Biol. , 219, 30-43. PMID: 10677253 DOI.
- ↑ 8.0 8.1 Raghoebir L, Bakker ER, Mills JC, Swagemakers S, Kempen MB, Munck AB, Driegen S, Meijer D, Grosveld F, Tibboel D, Smits R & Rottier RJ. (2012). SOX2 redirects the developmental fate of the intestinal epithelium toward a premature gastric phenotype. J Mol Cell Biol , 4, 377-85. PMID: 22679103 DOI.
- ↑ 9.0 9.1 Goto A, Sumiyama K, Kamioka Y, Nakasyo E, Ito K, Iwasaki M, Enomoto H & Matsuda M. (2013). GDNF and endothelin 3 regulate migration of enteric neural crest-derived cells via protein kinase A and Rac1. J. Neurosci. , 33, 4901-12. PMID: 23486961 DOI.
Online Textbooks
- Developmental Biology (6th ed) Gilbert, Scott F. Sunderland (MA): Sinauer Associates, Inc.; c2000. The Digestive Tube and Its Derivatives | Endodermal development of a human embryo
- The Gastrointestinal Circulation Peter R. Kvietys. San Rafael (CA): Morgan & Claypool Publishers; 2010. Table of Contents
- Motor Function of the Pharynx, Esophagus, and its Sphincters. Mittal RK. San Rafael (CA): Morgan & Claypool Life Sciences; 2011. Table of Contents
- Search NLM Online Textbooks "gastrointestinal tract" : Developmental Biology | Endocrinology | Molecular Biology of the Cell | The Cell- A molecular Approach
Historic Textbooks
- The Elements of Embryology by Foster, M., Balfour, F. M., Sedgwick, A., & Heape, W. (1883) The Alimentary Canal and its Appendages
- Text-Book of the Embryology of Man and Mammals by Dr Oscar Hertwig (1892) The Organs of the Inner Germ-Layer The Alimentary Tube with its Appended Organs
- Atlas of the Development of Man Volume 2 by Julius Kollmann (1907) Gastrointestinal
- Text-Book of Embryology by Bailey, F.R. and Miller, A.M. (1921) Alimentary tube and organs
| Historic Disclaimer - information about historic embryology pages |
|---|
|
Reviews
Le Guen L, Marchal S, Faure S & de Santa Barbara P. (2015). Mesenchymal-epithelial interactions during digestive tract development and epithelial stem cell regeneration. Cell. Mol. Life Sci. , 72, 3883-96. PMID: 26126787 DOI.
Browning KN & Travagli RA. (2014). Central nervous system control of gastrointestinal motility and secretion and modulation of gastrointestinal functions. Compr Physiol , 4, 1339-68. PMID: 25428846 DOI.
Hao MM, Bornstein JC, Vanden Berghe P, Lomax AE, Young HM & Foong JP. (2013). The emergence of neural activity and its role in the development of the enteric nervous system. Dev. Biol. , 382, 365-74. PMID: 23261929 DOI.
Burns AJ, Roberts RR, Bornstein JC & Young HM. (2009). Development of the enteric nervous system and its role in intestinal motility during fetal and early postnatal stages. Semin. Pediatr. Surg. , 18, 196-205. PMID: 19782301 DOI.
Burn SF & Hill RE. (2009). Left-right asymmetry in gut development: what happens next?. Bioessays , 31, 1026-37. PMID: 19708022 DOI.
McLin VA, Henning SJ & Jamrich M. (2009). The role of the visceral mesoderm in the development of the gastrointestinal tract. Gastroenterology , 136, 2074-91. PMID: 19303014 DOI.
Young HM. (2008). On the outside looking in: longitudinal muscle development in the gut. Neurogastroenterol. Motil. , 20, 431-3. PMID: 18416699 DOI.
Rubin DC. (2007). Intestinal morphogenesis. Curr. Opin. Gastroenterol. , 23, 111-4. PMID: 17268237 DOI.
Neu J. (2007). Gastrointestinal development and meeting the nutritional needs of premature infants. Am. J. Clin. Nutr. , 85, 629S-634S. PMID: 17284768
Anderson RB, Newgreen DF & Young HM. (2006). Neural crest and the development of the enteric nervous system. Adv. Exp. Med. Biol. , 589, 181-96. PMID: 17076282 DOI.
Costa RH, Kalinichenko VV, Holterman AX & Wang X. (2003). Transcription factors in liver development, differentiation, and regeneration. Hepatology , 38, 1331-47. PMID: 14647040 DOI.
de Santa Barbara P, van den Brink GR & Roberts DJ. (2003). Development and differentiation of the intestinal epithelium. Cell. Mol. Life Sci. , 60, 1322-32. PMID: 12943221 DOI.
Johnson LR. (1985). Functional development of the stomach. Annu. Rev. Physiol. , 47, 199-215. PMID: 3922287 DOI.
Articles
Ueno S, Yamada S, Uwabe C, Männer J, Shiraki N & Takakuwa T. (2016). The Digestive Tract and Derived Primordia Differentiate by Following a Precise Timeline in Human Embryos Between Carnegie Stages 11 and 13. Anat Rec (Hoboken) , 299, 439-49. PMID: 26995337 DOI.
Wilm B, Ipenberg A, Hastie ND, Burch JB & Bader DM. (2005). The serosal mesothelium is a major source of smooth muscle cells of the gut vasculature. Development , 132, 5317-28. PMID: 16284122 DOI.
Search PubMed
| Year | Total articles | Reviews | Free fun text |
|---|---|---|---|
| Mar 2007 | 29,361 | 3,494 | |
| Apr 2010 | 35980 | 4707 | 8086 |
| Dec 2018 | 58103 | 9188 | 44728 |
Search Pubmed: Gastrointestinal Tract Development
Additional Images
buccopharyngeal membrane

serial sections stage 13
Historic
| Historic Disclaimer - information about historic embryology pages |
|---|
|




Historic image showing midgut herniation

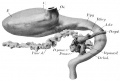
1914 Thyng

1914 Thyng Plate 2






Terms
| Gastrointestinal Tract Terms | ||
|---|---|---|
| ||
|
| System Links: Introduction | Cardiovascular | Coelomic Cavity | Endocrine | Gastrointestinal Tract | Genital | Head | Immune | Integumentary | Musculoskeletal | Neural | Neural Crest | Placenta | Renal | Respiratory | Sensory | Birth |
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, April 19) Embryology Gastrointestinal Tract Development. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Gastrointestinal_Tract_Development
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G