Gastrointestinal Tract - Liver Development: Difference between revisions
mNo edit summary |
mNo edit summary |
||
| Line 375: | Line 375: | ||
Mall FP. [[Paper - A Study of the Structural Unit of the Liver|A Study of the Structural Unit of the Liver]] (1906) Amer. J. of Anat. 5:227-308. | Mall FP. [[Paper - A Study of the Structural Unit of the Liver|A Study of the Structural Unit of the Liver]] (1906) Amer. J. of Anat. 5:227-308. | ||
<gallery> | <gallery> | ||
File:Mall1906-fig06.jpg|Fig 6 | File:Mall1906-fig06.jpg|Fig 6 human embryo 2.1 mm | ||
File:Mall1906-fig07.jpg|Fig 7 | File:Mall1906-fig07.jpg|Fig 7 human embryo 4.3 mm | ||
File:Mall1906-fig08.jpg|Fig 8 | File:Mall1906-fig08.jpg|Fig 8 human embryo 4.3 mm | ||
File:Mall1906-fig09.jpg|Fig 9 | File:Mall1906-fig09.jpg|Fig 9 human embryo 4.5 mm | ||
File:Mall1906-fig10.jpg|Fig 10 | File:Mall1906-fig10.jpg|Fig 10 human embryo 4.5 mm | ||
File:Mall1906-fig11.jpg|Fig 11 | File:Mall1906-fig11.jpg|Fig 11 human embryo 4 mm | ||
File:Mall1906-fig12.jpg|Fig 12 | File:Mall1906-fig12.jpg|Fig 12 human embryo 6.6 mm | ||
File:Mall1906-fig13.jpg|Fig 13 | File:Mall1906-fig13.jpg|Fig 13 human embryo 5 mm | ||
File:Mall1906-fig14.jpg|Fig 14 | File:Mall1906-fig14.jpg|Fig 14 human embryo 5 mm | ||
File:Mall1906-fig15.jpg|Fig 15 | File:Mall1906-fig15.jpg|Fig 15 human embryo 7 mm | ||
File:Mall1906-fig16.jpg|Fig 16 | File:Mall1906-fig16.jpg|Fig 16 human embryo 7 mm | ||
File:Mall1906-fig17.jpg|Fig 17 | File:Mall1906-fig17.jpg|Fig 17 human embryo 7 mm | ||
File:Mall1906-fig18.jpg|Fig 18 | File:Mall1906-fig18.jpg|Fig 18 human embryo 9 mm | ||
File:Mall1906-fig19.jpg|Fig 19 | File:Mall1906-fig19.jpg|Fig 19 human embryo 9 mm | ||
File:Mall1906-fig20.jpg|Fig 20 | File:Mall1906-fig20.jpg|Fig 20 human embryo 9 mm | ||
File:Mall1906-fig21.jpg|Fig 21 | File:Mall1906-fig21.jpg|Fig 21 human embryo 11 mm | ||
File:Mall1906-fig22.jpg|Fig 22 | File:Mall1906-fig22.jpg|Fig 22 human embryo 11 mm | ||
File:Mall1906-fig23.jpg|Fig 23 | File:Mall1906-fig23.jpg|Fig 23 human embryo 11 mm | ||
File:Mall1906-fig24.jpg|Fig 24 | File:Mall1906-fig24.jpg|Fig 24 human embryo 11 mm | ||
File:Mall1906-fig25.jpg|Fig 25 | File:Mall1906-fig25.jpg|Fig 25 human embryo 11 mm | ||
File:Mall1906-fig26.jpg|Fig 26 | File:Mall1906-fig26.jpg|Fig 26 human embryo 20 mm | ||
File:Mall1906-fig27.jpg|Fig 27 | File:Mall1906-fig27.jpg|Fig 27 human embryo 20 mm | ||
File:Mall1906-fig28.jpg|Fig 28 | File:Mall1906-fig28.jpg|Fig 28 human embryo 24 mm | ||
File:Mall1906-fig29.jpg|Fig 29 | File:Mall1906-fig29.jpg|Fig 29 model human embryo 24 mm | ||
File:Mall1906-fig30.jpg|Fig 30 | File:Mall1906-fig30.jpg|Fig 30 model human embryo 24 mm | ||
</gallery> | </gallery> | ||
Revision as of 12:38, 21 September 2015
| Embryology - 16 Apr 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
Introduction

This section of notes gives an overview of how the liver develops. The transverse septum (septum transversum) arises at an embryonic junctional site. The junctional region externally is where the ectoderm of the amnion meets the endoderm of the yolk sac. The junctional region internally is where the foregut meets the midgut. The mesenchymal structure of the transverse septum provides a support within which both blood vessels and the liver begin to form. Arises at embryonic junction (septum transversum): externally is where ectoderm of amnion meets endoderm of yolk sac and internally is where the foregut meets the midgut. Mesenchymal structure of transverse septum provides a support within which both blood vessels and liver begin to form in the underlying splanchnic mesoderm.
In the early embryo, the liver and heart grow rapidly forming obvious external swellings on the ventral embryo surface. The liver's initial embryonic function is mainly cardiovascular. Firstly, as a vascular connection between the developing placental vessels to the heart. Secondly, as a haemopoietic tissue where blood stem cells reside before bone marrow development.
See also Liver Histology showing both developmental and adult histology.
Some Recent Findings
|
| More recent papers |
|---|
 This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References Search term: Liver Embryology <pubmed limit=5>Liver Embryology</pubmed> |
Movies
|
|
Liver Development Stages

| Feature | |
| hepatic diverticulum development | |
| cell differentiation
septum transversum forming liver stroma hepatic diverticulum forming hepatic trabeculae | |
| epithelial cord proliferation enmeshing stromal capillaries | |
| hepatic gland and its vascular channels enlarge
hematopoietic function appeared | |
| obturation due to epithelial proliferation
bile ducts became reorganized (continuity between liver cells and gut) | |
| biliary ductules developed in periportal connective tissue
produces ductal plates that receive biliary capillaries | |
| Human data from Godlewski G, etal,[5] see also liver development in the rat during the embryonic period (Carnegie stages 15-23).[6] (More? Timeline human development) | |
| Carnegie Stage | Age (days) | CRL (mm) | Biliary system | Vascular | Hepatic parenchyma |
|---|---|---|---|---|---|
| 14 | 33 | 7 |
|
|
|
| 18 | 46 | 15 |
|
|
|
| 21 | 53 | 22.5 | Bile duct morphology as earlier stage. Common bile duct empties at the level of the proximal duodenum. |
|
Hepatic parenchyma a large rounded mass. |
| 23 | 58 | 27 | Bile duct morphology as earlier stage. |
|
|
| Data from a recent human study[7] Links: liver | Carnegie stage 14 | 18 | 21 | 23 | simple embryonic timeline | Timeline human development | |||||
Liver Buds
- Differentiates to form the hepatic diverticulum and hepatic primordium, generates the gall bladder then divides into right and left hepatic (liver) buds.
- Three connecting stalks (cystic duct, hepatic ducts) which fuse to form bile duct.
Left Hepatic Bud
- left lobe, quadrate, caudate (both q and c anatomically Left)
- caudate lobe of human liver consists of 3 anatomical parts: Spiegel's lobe, caudate process, and paracaval portion.
Right Hepatic Bud
- right lobe
Liver Structural Origins
- Hepatic Buds - form hepatocytes, produce bile from week 13 (forms meconium of newborn)
- Vitelline Veins - form sinusoids
- Mesenchyme - form connective tissue and Kupffer cells
Function - Haemopoiesis
Embryonic liver also involved in blood formation, after the yolk sac and blood islands acting as a primary site.
Components of Liver Formation

Primitive Endoderm
|
|
|
Data from mouse [9]
Hepatoblasts - endoderm-derived cells can differentiate into either:
- hepatocytes - populate the bulk of the liver parenchyma.
- cholangiocytes - line the intrahepatic bile ducts.
- Links: Endoderm | Mouse Development
Development
Stage 13

The images below link to larger cross-sections of the mid-embryonic period (end week 4) stage 13 embryo starting just above the level of the liver and then in sequence through the liver to the level of the stomach. Note the relative position of the liver with respect to the abdominal cavity, the gall bladder and the heart.
The transverse septum differentiates to form the hepatic diverticulum and the hepatic primordium, these two structures together will go on to form different components of the mature liver and gall bladder. At this stage large vascular channels can be seen coursing through the liver primordium.
|
|

|

|

|

|

|
| D3L | D4L | D5L | D6L | D7L | E1L |

|

| ||||
| G6L | G7L |
- Links: Carnegie stage 13 - serial sections | Embryo Serial Sections | Embryo Carnegie stage 13 Movies
Stage 22
| Virtual Slide Features - Stage 22 Liver | |||||||
|---|---|---|---|---|---|---|---|

|
Virtual Slide - Stage 22 Liver and Ductus Venosus All Virtual Slides
The links shown in the table below are to specific features shown on the Human embryo (stage 22) Liver and Ductus Venosus virtual slide. See also notes on Liver Development Clicking the text will open the slide at a detailed view with the structure generally located in the centre of the view. The slide then can also be zoomed out from the set magnification using the controls in the upper left or the mouse. Use your browser back button to return to this table. |
You can also make your own selected feature view.
See also Permalink help | |||||
| Cardiovascular | Liver | Endocrine | Musculoskeletal | Neural | Gastrointestinal | ||
The images below link to larger cross-sections of the end of the embryonic period (week 8) stage 22 embryo starting just above the level of the liver and then in sequence through the entire liver. (Note the sections are viewed from below, LR axis is reversed)
The rapidly developing liver also forms a visible surface bulge on the embryo directly under the heart bulge. The liver now occupies the entire ventral body cavity with parts of the gastrointestinal tract and urinary system "embedded" within its structure. Note in this image the large central ductus venosus.

|

|

|

|

|
| E3L | E4L | E5L | E6L | E7L |

|

|

|

|

|
| F1L | F2L | F3L | F4L | F5L |
- Links: Carnegie stage 22 - serial sections | Embryo Serial Sections | Embryo Carnegie stage 22 Movies
Selected Stage 22 Images

|
E3 Overview of liver region for selected high power views shown below. Note the position and size of the developing liver spanning the entire abdomen and within the liver the large central ductus venosus. |

|
E4 Central veins of liver. Radiating appearance of hepatic sinusoids. unlabeled version |

|
E5 Central vein with endothelial lining, containing nucleated erythrocytes, fetal red blood cells. The fetal liver has an important haemopoietic role. unlabeled version |
Week 9

Paraffin-embedded sections of human embryonic liver at 9 weeks (GA 11 weeks).[10] |
|
Ductal Plate
The ductal plate is a primitive biliary epithelium which develops in mesenchyme adjacent to portal vein branches (periportal hepatoblasts). During liver development it is extensively reorganised (ductal plate remodelling) within the developing liver to form the intrahepatic bile ducts (IHBD). If remodelling does not occur, leading to excess of embryonic bile duct structures in the portal tract, these developmental abnormalities are described as "ductal plate malformation" (DPM).
Ductal Plate Malformations
- Interlobular bile ducts - autosomal recessive polycystic kidney disease
- Smaller interlobular ducts - von Meyenburg complexes
- Larger intrahepatic bile ducts - Caroli's disease
Bile Secretion
The epithelial cells that line the bile ducts are called cholangiocytes.
The pathway below describes the production and passage of bile for final excretion into the duodenum:
- hepatocytes produce bile
- secreted into bile canaliculi
- connected to intrahepatic bile ducts
- intrahepatic bile ducts connect to the hepatic duct
- then the cystic duct for storage in the gallbladder
- then the common bile duct into the duodenum
The term extrahepatic bile ducts (EHBDs) is used to describe the hepatic, cystic, and common bile ducts.
The developing bile ducts express VEGF while hepatoblasts express angiopoietin-1, these two signals are thought to regulate arterial vasculogenesis and remodeling of the hepatic artery respectively.[11]
Liver Blood Flow

Dual blood supply of the liver merges upon entry into the liver lobule at the portal field.
- branches of the portal vein
- branches of the hepatic artery
The blood flows along the sinusoid and exits at the central vein.
Hepatocytes

These are the adult functional cells forming the majority of the liver (80% of the cells).
Many different functions including:
- Storage of substances including glucose (as glycogen), vitamin A (possibly in specialized adipocytes), vitamin B12, folic acid and iron.
- Lipid Turnover synthesis of plasmalipoproteins
- Plasma Protein Synthesis albumin, alpha and beta globulins, prothrombin, fibrinogen
- Metabolism fat soluble compounds (drugs, insecticides), steroid hormones turnover
- Secretion bile (about 1 litre/day)
Kupffer Cells
Kupffer Cells are a population of tissue macrophages found in the lumen of hepatic sinusoids, their role is endocytic against blood-borne materials entering the liver.
Primordial (primitive) macrophages arise in the yolk sac and then differentiate into fetal macrophages, either of these enter the blood and migrate into the developing liver.[12]
Kupffer Cells image
- Search PubMed: Kupffer cell development
Liver Associated Vessels

Liver ventral surface and associated veins (human embryo, 24-25 days, after His.) |
|
Adult Liver Transplants
- About 6,000 liver transplant operations are performed in the United States (http://www.liverfoundation.org/education/info/transplant/)
- About 600–700 in the UK every year (http://www.britishlivertrust.org.uk/home/the-liver/liver-transplantation/a-history-of-liver-transplantation-and-current-statistics.aspx).
- The main limitation on numbers are the availability of donor organs.[13]
Histology

The Liver Lobule
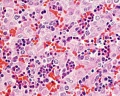
Histology-fetal liver HEx40
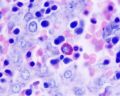
Histology-fetal liver x100


Adult liver Portal Triad

- Links: Liver Histology
Abnormalities
Congenital absence of the portal vein (CAPV) - a rare abnormality where the intestinal and splenic venous drainage bypass the liver and drain directly into the systemic veins through various porto-systemic shunts.
References
- ↑ <pubmed>21943389</pubmed>
- ↑ <pubmed>19556507</pubmed>| PMC2771431 | Science
- ↑ <pubmed>19556507</pubmed>
- ↑ <pubmed>16891202</pubmed>
- ↑ <pubmed>9407542</pubmed>
- ↑ <pubmed>9718390</pubmed>
- ↑ Lhuaire M, Tonnelet R, Renard Y, Piardi T, Sommacale D, Duparc F, Braun M & Labrousse M. (2015). Developmental anatomy of the liver from computerized three-dimensional reconstructions of four human embryos (from Carnegie stage 14 to 23). Ann. Anat. , 200, 105-13. PMID: 25866917 DOI.
- ↑ <pubmed>21829697</pubmed>| PLoS One.
- ↑ Kaufman and Bard, The Anatomical Basis of Mouse Development 1999 Academic Press
- ↑ <pubmed>19841744</pubmed>| PMC2760133 | PLoS
- ↑ <pubmed>12360416</pubmed>
- ↑ <pubmed>15057601</pubmed>
- ↑ <pubmed>20169088</pubmed>| PMC2821762
Reviews
<pubmed>21199531</pubmed> <pubmed>20551648</pubmed> <pubmed>20169172</pubmed> <pubmed>20159590</pubmed> <pubmed>20086072</pubmed> <pubmed>18484608</pubmed>
Articles
<pubmed>22371217</pubmed> <pubmed>22105167</pubmed> <pubmed>21708104</pubmed>
Search Pubmed
Search Bookshelf Liver Development
Search Pubmed Now: Liver Development | Embryonic Liver Development
Additional Images
Historic
Mall FP. A Study of the Structural Unit of the Liver (1906) Amer. J. of Anat. 5:227-308.

Fig 6 human embryo 2.1 mm

Fig 7 human embryo 4.3 mm

Fig 8 human embryo 4.3 mm

Fig 9 human embryo 4.5 mm

Fig 10 human embryo 4.5 mm

Fig 11 human embryo 4 mm

Fig 12 human embryo 6.6 mm
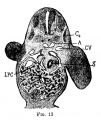
Fig 13 human embryo 5 mm

Fig 14 human embryo 5 mm

Fig 15 human embryo 7 mm
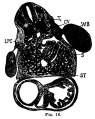
Fig 16 human embryo 7 mm

Fig 17 human embryo 7 mm
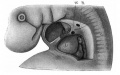
Fig 18 human embryo 9 mm

Fig 19 human embryo 9 mm

Fig 20 human embryo 9 mm

Fig 21 human embryo 11 mm

Fig 22 human embryo 11 mm

Fig 23 human embryo 11 mm

Fig 24 human embryo 11 mm
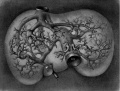
Fig 25 human embryo 11 mm

Fig 26 human embryo 20 mm

Fig 27 human embryo 20 mm

Fig 28 human embryo 24 mm

Fig 29 model human embryo 24 mm

Fig 30 model human embryo 24 mm

























{kind=link}
{kind=link}
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, April 16) Embryology Gastrointestinal Tract - Liver Development. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Gastrointestinal_Tract_-_Liver_Development
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G