File:Patten1938 plate34.jpg: Difference between revisions
mNo edit summary |
mNo edit summary |
||
| Line 8: | Line 8: | ||
===Reference=== | ===Reference=== | ||
{{Ref-Patten1938}} | {{Ref-Patten1938}} | ||
{{Footer}} | |||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Latest revision as of 15:48, 27 February 2017
Plate 34
FIGS. 17. 18 and 19. Heart of a 1 month old infant showing the conditions encountered in premature closure of the foramen ovale. (Babies and Childrens Hospital. Autopsy No. A—374. made available through the courtesy of Dr. Howard T. Karsner. Western Reserve University Medical School.) Although there is no way of being certain whether the closure as seen at autopsy had been fully established in utero. there seems no doubt that a marked ante natal stenosis. if not an atresia. must have existed. This is indicated: (1) by the slit-like fossa ovalis which is but a small fraction of the oval opening left when septum secundum normally ceases further growth: ( 2) by the complete adhesion of the valvula which does not ordinarily occur until several months after the cessation of transseptal flow: and (3) by the deficiently developed left ventricle which seems clearly attributable to lessened left atrial intake due to a foramen ovale closed. or greatly narrowed. during the growth of the fetal heart.
FIGS. 20. 21 and 22. Possible case of postnatal repair of congenital defect at the foramen ovale. The appearance of the narrowed fossa ovalis is superficially somewhat similar to the case of premature closure illustrated above. but there are two associated conditions which indicate that in this case the narrowing occurred postnatally. First is the normal development of the ventricles. If the fossa ovalis had been of its present abnormally small size during intrauterine life the left ventricle would have been undersized. Second is the faint depression which sketches the contours of a fossa ovalis of the normal size. This seems to suggest that the fossa was. at the time of birth. of the size outlined by this depression, and that the difierently disposed tissue now narrowing it was formed later. There is yet another interesting condition pointing in the same direction. In the valnila foraminis ovalis one sees an arrangement of robust strands which suggest that it might once have appeared not unlike the defective valve in Fig. 9. Between these heavy strands there is a more delicate tissue which might conceivably have been secondarily formed. Of course this entire interpretation must be regarded as tentative. but postnatal repair of a congenital defect. if it does occur. is of so much interest that it seemed worth while presenting this unique case in the hope of stimulating further observations bearing on such a possibility.
Reference
Patten BM. Developmental defects at the foramen ovale. (1938) Am J Pathol. 14(2):135-162. PMID 19970381
Cite this page: Hill, M.A. (2024, April 19) Embryology Patten1938 plate34.jpg. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/File:Patten1938_plate34.jpg
{kind=link}
{kind=link}
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G
File history
Click on a date/time to view the file as it appeared at that time.
| Date/Time | Thumbnail | Dimensions | User | Comment | |
|---|---|---|---|---|---|
| current | 15:42, 27 February 2017 |  | 1,280 × 1,905 (307 KB) | Z8600021 (talk | contribs) | |
| 15:42, 27 February 2017 | 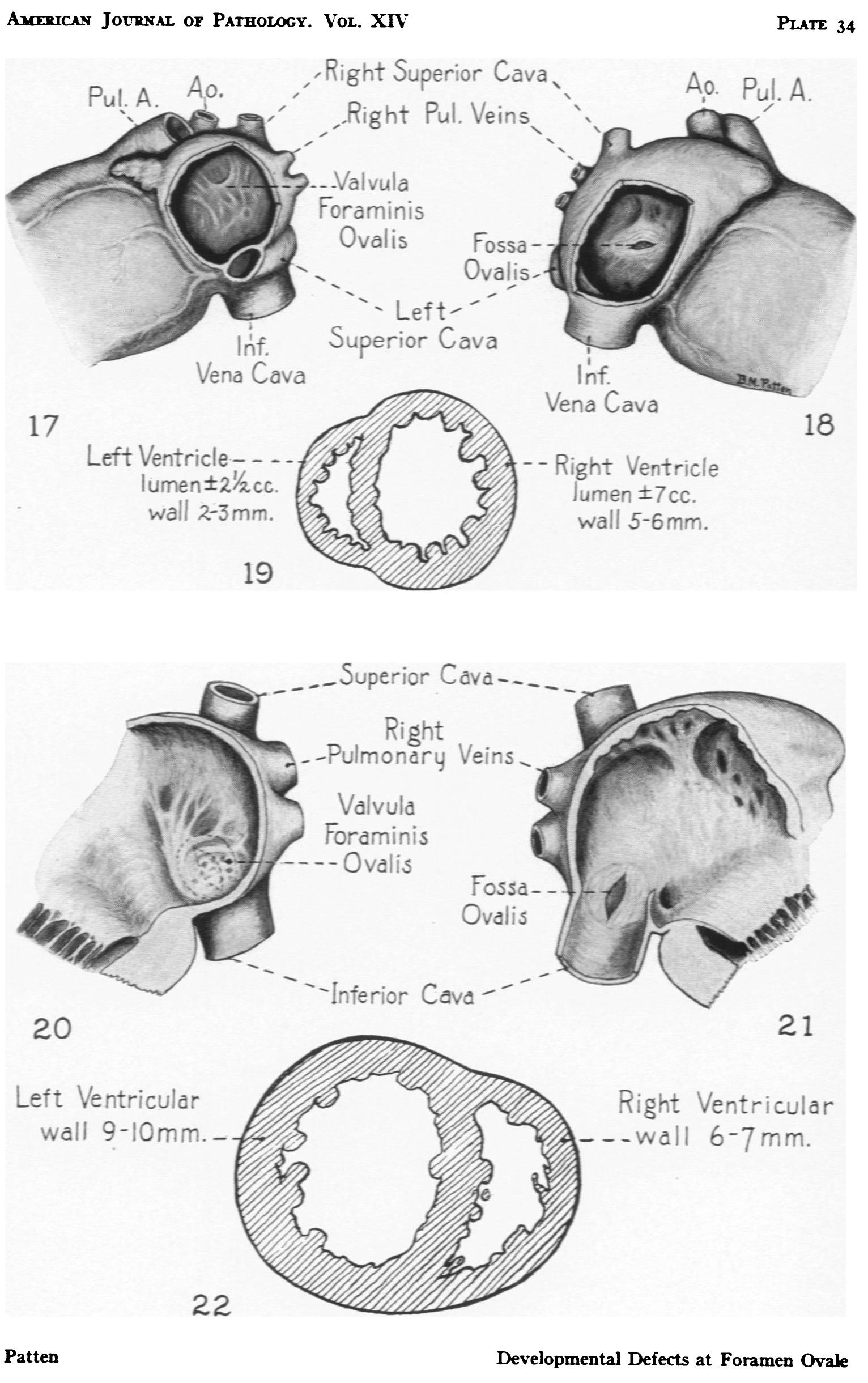 | 1,532 × 2,441 (414 KB) | Z8600021 (talk | contribs) | ===Reference=== {{Ref-Patten1938}} |
You cannot overwrite this file.
File usage
The following 2 pages use this file:
{kind=link}