File:Braune 1877 plate 2 fig5.jpg: Difference between revisions
({{Braune 1877 footer}}) |
No edit summary |
||
| (3 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{Braune 1877 | ==Plate 2 Sagittal Female Fig. 5. Female pelvis, set. 30; multipara; anteflexion of uterus== | ||
Legendre, xviii. 1. Uterus. 2. Bladder. 3. Rectum. 4. Symphysis. | |||
The angle between the body and neck of the uterus impinges upon the rectum. The walls of the uterus appear throughout of uniform thickness, and the rectum and bladder are but slightly encroached upon. | |||
The bladder may be so compressed in the middle line that it assumes an hour-glass form, one portion of it still retaining the urine after the other has been emptied by the catheter. In such conditions the catheter would have to be passed into the further cavity, so that all the urine might be drawn off. | |||
The anterior lip of the os is continued into the anterior wall of the vagina without a clearly defined border, whilst the hinder is strongly prominent and has a length of one inch. The cavity of the vagina contains the canal of the cervix. The vagina itself is 3 inches in length, whilst that in fig. 4 was only 1-5 inch, and the long extended one in fig. 2, 2.8 inches. In like manner the distance of the peritoneum on the posterior wall of the vagina from the perineum is increased, being 3.24 inches ; in fig. 1 it is 2.08 inches. The conjugate diameter is large, being 4.28 inches. The ante-flexed position of the uterus is shown by Schultze to be the normal one in young persons when the bladder is empty. The uterus would, following the contracting bladder, lie upon it, and from traction exercised by the utero-vesical ligament of Courty extend the base of the bladder backwards (cf. Volkmann,'Sammlung Klinisches Yortrage,' No. 50). There is no question that during the variations of the forms of the rectum and bladder, according to the amount of their contents, a space remains in the pelvis near the uterus, which must either be temporarily filled with small intestine, or render necessary a larger amount of variability in the shape of the uterus itself. If we exclude with Claudius and Hennig the possibility of a filling-up of Douglas's pouch by the small intestine, in the case of the bladder and rectum being empty, the difficulty of representing the topography of the uterus would be enormous, as is evident to every experienced anatomist. We have the choice only, either with Henke to show the uterus set up at a fixed angle with the vagina surrounded by small intestine, or with Schultze to represent it bent over on the bladder. However important it may be to determine these relations accurately, I do not think that it can be done at present ; in any case I should not follow Schultze's statement completely. The extension of the base of the bladder does not appear to me in Schultze's plate to be correct, still less so does the assumption of a forcing of the same by means of a ligament, as Courty describes. The lax cellular tissue which lies between the uterus and the base of the bladder, and in which a large number of thin-walled veins run, cannot be regarded as a ligament in the usual sense of the word, and is not shown as such in my plates. It would be necessary to obtain a series of bodies of young females in order to study the variations of the position of the uterus in well-hardened preparations | |||
{{Braune 1877 Plate 2}} | |||
{{Braune 1877 header}} | |||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Latest revision as of 09:13, 10 November 2012
Plate 2 Sagittal Female Fig. 5. Female pelvis, set. 30; multipara; anteflexion of uterus
Legendre, xviii. 1. Uterus. 2. Bladder. 3. Rectum. 4. Symphysis.
The angle between the body and neck of the uterus impinges upon the rectum. The walls of the uterus appear throughout of uniform thickness, and the rectum and bladder are but slightly encroached upon.
The bladder may be so compressed in the middle line that it assumes an hour-glass form, one portion of it still retaining the urine after the other has been emptied by the catheter. In such conditions the catheter would have to be passed into the further cavity, so that all the urine might be drawn off.
The anterior lip of the os is continued into the anterior wall of the vagina without a clearly defined border, whilst the hinder is strongly prominent and has a length of one inch. The cavity of the vagina contains the canal of the cervix. The vagina itself is 3 inches in length, whilst that in fig. 4 was only 1-5 inch, and the long extended one in fig. 2, 2.8 inches. In like manner the distance of the peritoneum on the posterior wall of the vagina from the perineum is increased, being 3.24 inches ; in fig. 1 it is 2.08 inches. The conjugate diameter is large, being 4.28 inches. The ante-flexed position of the uterus is shown by Schultze to be the normal one in young persons when the bladder is empty. The uterus would, following the contracting bladder, lie upon it, and from traction exercised by the utero-vesical ligament of Courty extend the base of the bladder backwards (cf. Volkmann,'Sammlung Klinisches Yortrage,' No. 50). There is no question that during the variations of the forms of the rectum and bladder, according to the amount of their contents, a space remains in the pelvis near the uterus, which must either be temporarily filled with small intestine, or render necessary a larger amount of variability in the shape of the uterus itself. If we exclude with Claudius and Hennig the possibility of a filling-up of Douglas's pouch by the small intestine, in the case of the bladder and rectum being empty, the difficulty of representing the topography of the uterus would be enormous, as is evident to every experienced anatomist. We have the choice only, either with Henke to show the uterus set up at a fixed angle with the vagina surrounded by small intestine, or with Schultze to represent it bent over on the bladder. However important it may be to determine these relations accurately, I do not think that it can be done at present ; in any case I should not follow Schultze's statement completely. The extension of the base of the bladder does not appear to me in Schultze's plate to be correct, still less so does the assumption of a forcing of the same by means of a ligament, as Courty describes. The lax cellular tissue which lies between the uterus and the base of the bladder, and in which a large number of thin-walled veins run, cannot be regarded as a ligament in the usual sense of the word, and is not shown as such in my plates. It would be necessary to obtain a series of bodies of young females in order to study the variations of the position of the uterus in well-hardened preparations
- Sagittal Female: Plate 2A | Plate 2B | Plate 2 Fig.1 | Plate 2 Fig.2 | Plate 2 Fig.3 | Plate 2 Fig.4 | Plate 2 Fig.5 | Plate 2 Fig.6 | Plate 2 Fig.7 | Topographical Anatomy (1877)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Embryology - 24 Apr 2024 |
|---|
| Google Translate - select your language from the list shown below (this will open a new external page) |
|
العربية | català | 中文 | 中國傳統的 | français | Deutsche | עִברִית | हिंदी | bahasa Indonesia | italiano | 日本語 | 한국어 | မြန်မာ | Pilipino | Polskie | português | ਪੰਜਾਬੀ ਦੇ | Română | русский | Español | Swahili | Svensk | ไทย | Türkçe | اردو | ייִדיש | Tiếng Việt These external translations are automated and may not be accurate. (More? About Translations) |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Braune W. An atlas of topographical anatomy after plane sections of frozen bodies. (1877) Trans. by Edward Bellamy. Philadelphia: Lindsay and Blakiston.
- Plates: 1. Male - Sagittal body | 2. Female - Sagittal body | 3. Obliquely transverse head | 4. Transverse internal ear | 5. Transverse head | 6. Transverse neck | 7. Transverse neck and shoulders | 8. Transverse level first dorsal vertebra | 9. Transverse thorax level of third dorsal vertebra | 10. Transverse level aortic arch and fourth dorsal vertebra | 11. Transverse level of the bulbus aortae and sixth dorsal vertebra | 12. Transverse level of mitral valve and eighth dorsal vertebra | 13. Transverse level of heart apex and ninth dorsal vertebra | 14. Transverse liver stomach spleen at level of eleventh dorsal vertebra | 15. Transverse pancreas and kidneys at level of L1 vertebra | 16. Transverse through transverse colon at level of intervertebral space between L3 L4 vertebra | 17. Transverse pelvis at level of head of thigh bone | 18. Transverse male pelvis | 19. knee and right foot | 20. Transverse thigh | 21. Transverse left thigh | 22. Transverse lower left thigh and knee | 23. Transverse upper and middle left leg | 24. Transverse lower left leg | 25. Male - Frontal thorax | 26. Elbow-joint hand and third finger | 27. Transverse left arm | 28. Transverse left fore-arm | 29. Sagittal female pregnancy | 30. Sagittal female pregnancy | 31. Sagittal female at term
| Historic Disclaimer - information about historic embryology pages |
|---|
 |
File history
Click on a date/time to view the file as it appeared at that time.
| Date/Time | Thumbnail | Dimensions | User | Comment | |
|---|---|---|---|---|---|
| current | 14:04, 31 October 2012 | 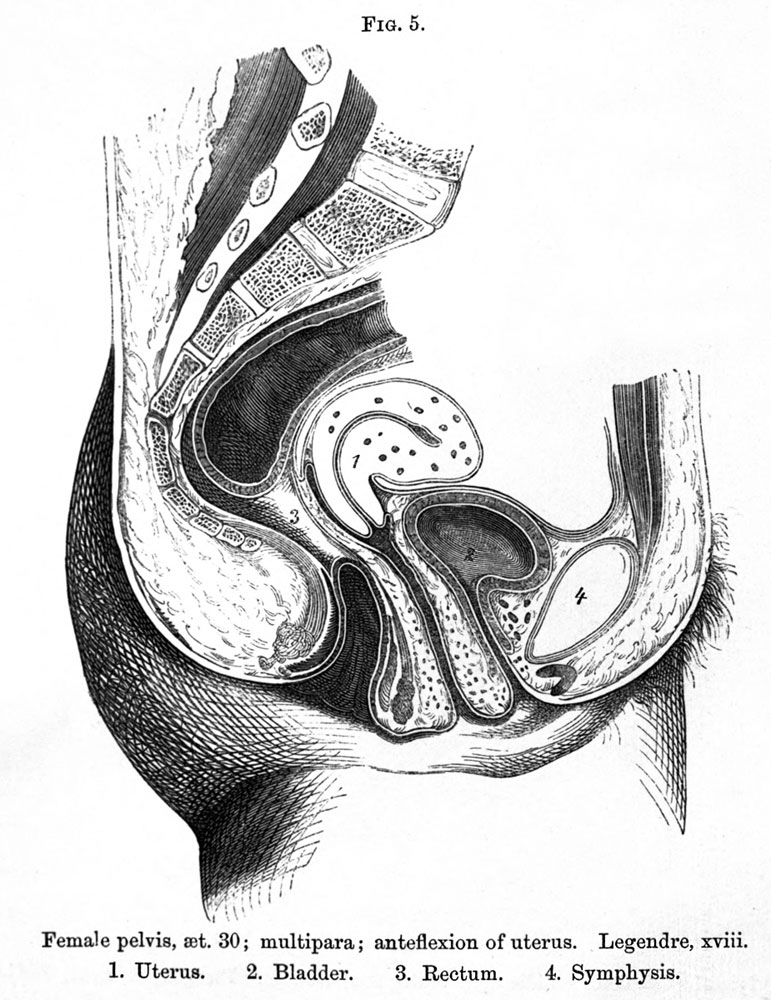 | 771 × 1,000 (169 KB) | Z8600021 (talk | contribs) | {{Braune 1877 footer}} |
You cannot overwrite this file.
File usage
The following 2 pages use this file:
{kind=link}