Introduction
The term "Fetal Growth Restriction" (FGR) or intrauterine growth restriction (IUGR) are used to describe when the fetus does not reach full growth potential. This is usually determined by clinical sonography calculations of fetal weight, fetal size, or symmetry.
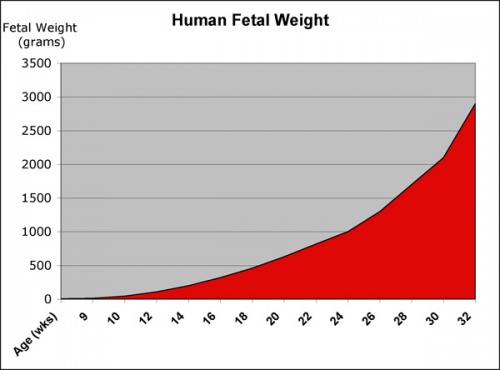
The fetal period (weeks 9 to 37) is about four times the length of the embryonic period and the clinical term may not relate directly to just the "fetal period", that is a time of extensive growth in size and mass as well as ongoing differentiation of organ systems established in the embryonic period. Clinically this period is generally described as the Second Trimester and Third Trimester. Many of the critical measurements of growth are now carried out by ultrasound and measured at birth including the Birth-Weight.
- Fetal Graphs: Crown-Rump Length (CRL) | Third trimester CRL | Head Circumference | Head Circumference 2nd Trimester | Liver Weight | Pancreas Weight | Thymus Weight | Small Intestine Length | Large Intestine Length | Length and Weight Changes | Fetal Development
Some Recent Findings
- Longitudinal changes in gestational weight gain and the association with intrauterine fetal growth[1] "Ultrasounds were targeted at17, 25, 33, and 37 weeks of gestation. Analyses involved a multi-step process. First, trajectories were estimated across gestation for maternal weight gain and fetal biometrics [abdominal circumference (AC, mm), biparietal diameter (BPD, mm), femur length (FL, mm), and estimated fetal weight (EFW, g)] using linear mixed models. Second, the association between maternal weight changes (per 5kg) and corresponding fetal growth from 0 to 17, 17 to 28, and 28 to 37 weeks was estimated for each fetal parameter adjusting for prepregnancy body mass index, height, parity, chronic diseases, age, smoking, fetal sex, and weight gain up to the respective period as applicable. Third, the probability of fetal SGA, EFW <10th percentile, at the 3rd ultrasound was estimated across the spectrum of maternal weight gain rate by SGA status at the 2nd ultrasound. RESULTS: From 0 to 17 weeks, changes in maternal weight were most strongly associated with changes in BPD [β=0.51 per 5kg (95%CI 0.26, 0.76)] and FL [β=0.46 per 5kg (95%CI 0.26, 0.65)]. From 17 to 28 weeks, AC [β=2.92 per 5kg (95%CI 1.62, 4.22)] and EFW [β=58.7 per 5kg (95%CI 29.5, 88.0)] were more strongly associated with changes in maternal weight. Increased maternal weight gain was significantly associated with a reduced probability of intrauterine SGA; for a normal weight woman with SGA at the 2nd ultrasound, the probability of fetal SGA with a weight gain rate of 0.29kg/w (10th percentile) was 59%, compared to 38% with a rate of 0.67kg/w (90th percentile). CONCLUSION: Among women at high-risk for SGA, maternal weight gain was associated with fetal growth throughout pregnancy, but had a differential relationship with specific biometrics across gestation. For women with fetal SGA identified mid-pregnancy, increased antenatal weight gain was associated with a decreased probability of fetal SGA approximately 7 weeks later."
- Inflammation in rat pregnancy inhibits spiral artery remodeling leading to fetal growth restriction and features of preeclampsia[2] "Fetal growth restriction (FGR) and preeclampsia (PE) are often associated with abnormal maternal inflammation, deficient spiral artery (SA) remodeling, and altered uteroplacental perfusion. Here, we provide evidence of a novel mechanistic link between abnormal maternal inflammation and the development of FGR with features of PE. Using a model in which pregnant rats are administered low-dose lipopolysaccharide (LPS) on gestational days 13.5-16.5, we show that abnormal inflammation resulted in FGR mediated by tumor necrosis factor-α (TNF). Inflammation was also associated with deficient trophoblast invasion and SA remodeling, as well as with altered uteroplacental hemodynamics and placental nitrosative stress. Moreover, inflammation increased maternal mean arterial pressure (MAP) and was associated with renal structural alterations and proteinuria characteristic of PE. Finally, transdermal administration of the nitric oxide (NO) mimetic glyceryl trinitrate prevented altered uteroplacental perfusion, LPS-induced inflammation, placental nitrosative stress, renal structural and functional alterations, increase in MAP, and FGR. These findings demonstrate that maternal inflammation can lead to severe pregnancy complications via a mechanism that involves increased maternal levels of TNF. Our study provides a rationale for the use of antiinflammatory agents or NO-mimetics in the treatment and/or prevention of inflammation-associated pregnancy complications."
- A randomised controlled trial comparing standard or intensive management of reduced fetal movements after 36 weeks gestation-a feasibility study[3] "Women presenting with reduced fetal movements (RFM) in the third trimester are at increased risk of stillbirth or fetal growth restriction. These outcomes after RFM are related to smaller fetal size on ultrasound scan, oligohydramnios and lower human placental lactogen (hPL) in maternal serum. We performed this study to address whether a randomised controlled trial (RCT) of the management of RFM was feasible with regard to: i) maternal recruitment and retention ii) patient acceptability, iii) adherence to protocol. Additionally, we aimed to confirm the prevalence of poor perinatal outcomes defined as: stillbirth, birthweight <10th centile, umbilical arterial pH <7.1 or unexpected admission to the neonatal intensive care unit. ...An RCT of management of RFM is feasible with a low rate of attrition. Investigations decrease maternal anxiety. Participants in the intensive group were more likely to have IOL for RFM. Further work is required to determine the likely level of intervention in the standard care arm in multiple centres, to develop additional placental biomarkers and to confirm that the composite outcome is valid.Trial registration ISRCTN07944306."
|
| More recent papers
|
|
This table allows an automated computer search of the external PubMed database using the listed "Search term" text link.
- This search now requires a manual link as the original PubMed extension has been disabled.
- The displayed list of references do not reflect any editorial selection of material based on content or relevance.
- References also appear on this list based upon the date of the actual page viewing.
References listed on the rest of the content page and the associated discussion page (listed under the publication year sub-headings) do include some editorial selection based upon both relevance and availability.
More? References | Discussion Page | Journal Searches | 2019 References | 2020 References
Search term: Fetal Growth Restriction
<pubmed limit=5>Fetal Growth Restriction</pubmed>
|
Reading
- Human Embryology (3rd ed.) Larson Chapter 15: Fetal development and the Fetus as Patient p481-499
- The Developing Human: Clinically Oriented Embryology (8th ed.) Moore and Persaud Chapter 6: The Fetal Period: Ninth Week to Birth
- Color Atlas of Clinical Embryology (2nd ed.) Moore, Persaud and Shiota Chapter 3: 9th to 38th weeks of human development p50-68
|
|
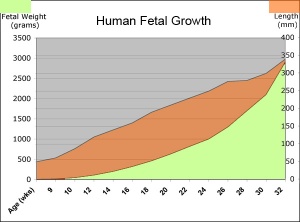
Fetal length and weight change
Second Trimester
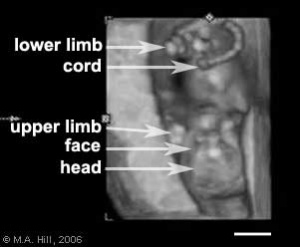
Fetus - second trimester
(ultrasound)
- Second Trimester
- Week 12 - CRL 85 mm, femur length 15 mm, biparietal diameter 25 mm.
Begin by working through the features present in the early 10 week female fetus. Then look in detail at the head development in a 12 week fetus.
Then look in detail at the head development in a 12 week fetus showing both forms of ossification in the skull.
Fetal Head Growth
Second and third trimesters
Third Trimester
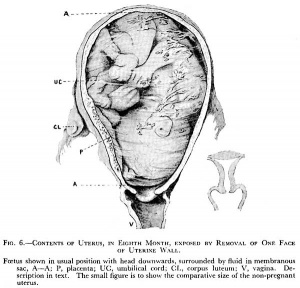
Fetus - third trimester
(historic image)
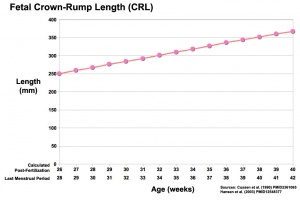
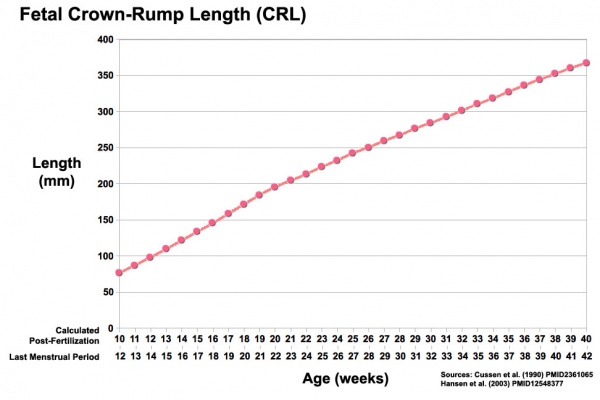
Third trimester Crown-Rump Length
- Vibration acoustically of maternal abdominal wall induces startle respone in fetus.
- Month 7 - respiratory bronchioles proliferate and end in alveolar ducts and sacs.
- Week 37 to 38 Birth.
- Links: Third Trimester
References
- ↑ <pubmed>25978857</pubmed>
- ↑ <pubmed>24395887</pubmed>
- ↑ <pubmed>23590451</pubmed>
Journals
Reviews
<pubmed></pubmed>
<pubmed></pubmed>
<pubmed>22990459</pubmed>
<pubmed>22696366</pubmed>
<pubmed>22526452</pubmed>
<pubmed></pubmed>
<pubmed></pubmed>
Articles
<pubmed>23599816</pubmed>
<pubmed></pubmed>
<pubmed></pubmed>
Search PubMed
Search Pubmed: Fetal Growth Restriction
Glossary Links
- Glossary: A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | Numbers | Symbols | Term Link
Cite this page: Hill, M.A. (2024, April 17) Embryology Abnormal Development - Fetal Growth Restriction. Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/Abnormal_Development_-_Fetal_Growth_Restriction
- What Links Here?
- © Dr Mark Hill 2024, UNSW Embryology ISBN: 978 0 7334 2609 4 - UNSW CRICOS Provider Code No. 00098G

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
