Talk:BGDA Practical Placenta - Abnormalities
<mediaplayer>http://www.youtube.com/watch?v=i9Hwn2DOgKo</mediaplayer>
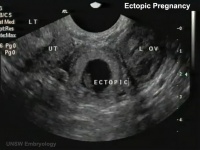
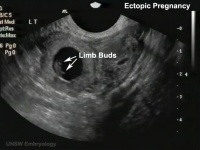
Ultrasound Ectopic Implantation
| Tubal Ectopic | Bicornuate Uterus Ectopic | ||||||
|---|---|---|---|---|---|---|---|
|
|

|

|
|

|
- Links: Ectopic Implantation | Ultrasound
Computed Tomography Ectopic Implantation
Computed Tomography imaging findings of a 37-year-old woman with interstitial pregnancy.[1] Showing initial CT detection and a subsequent scan following rupture causing a hematoma around uterus and a massive hemoperitoneum.

Initial CT - gestational sac |

Follow-up CT - massive hemoperitoneum |

CT - hematoma around uterus |
- Links: Computed Tomography
Magnetic Resonance Imaging Abdominal Ectopic Implantation
2W SPAIR sagittal MRI of lower abdomen demonstrating the placental invasion.[2]
|

|
See also Heterotopic Pregnancy
Statistics

Ectopic Pregnancies- United-States 1970-1992[3]

Ectopic Pregnancy Histology

CDC Image by Dr. Edwin P. Ewing, Jr., 1972

Ed Uthman Image (pathologist in Houston, Texas) section of ectopic (tubal) pregnancy about Carnegie stage 7 in Week 3.
Image version links: ExtraLarge 1712x1206px | Large 1024x721px | Medium 500x352px

Ed Uthman Image (pathologist in Houston, Texas) image of of ectopic (tubal) pregnancy about Carnegie stage 15 in Week 5.
Image version links: ExtraLarge 1874 x 2000px | Large 959 x 1024px | Medium 468 x 500px
Tubal Ectopic Pregnancy
| Chlamydia infections (Chlamydia trachomatis) are the most common bacterial sexually transmitted infection, often undiagnosed and asymptomatic. The infections can ascend the female genital tract, colonizing the endometrial mucosa, then the uterine tubes. This type of infection is described as pelvic inflammatory disease (PID). |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Interstitial Pregnancy
| (cornual pregnancy) A less common type 2 to 4% of ectopic pregnancies. The gestation develops in the uterine portion of the fallopian tube lateral to the round ligament. |  Interstitial ectopic pregnancy[4] |
Ovarian Ectopic Pregnancy
| Clinical operative photograph at the beginning of the procedure of the laparoscopic treatment of the ovarian pregnancy.
|

Ovarian Ectopic Pregnancy[5] |
Cervical Ectopic Pregnancy

This form of ectopic pregnancy is a rare high-risk condition and represents less than 1% of all ectopic pregnancies. The reported incidence varies between 1:1,000 to 1:18,000.
Rudimentary Horn Pregnancy
A rare types of ectopic pregnancy (about 1 in 76,000 pregnancies) in most cases the horn is non-communicating. Therefore fertilisation probably occurs by transperitoneal migration. This form untreated can also lead to uterine rupture.
Caesarean Scar Pregnancy
A rare types of ectopic pregnancy (about 1 in 2000 pregnancies), but probably increasing as caesarean rates rise. The gestation is completely surrounded by both myometrium and fibrous tissue of the caesarean section scar and separated from the endometrial cavity and endocervical canal.
- ↑ <pubmed>20046504</pubmed>| PMC2799642 | Korean J Radiol.
- ↑ <pubmed>19918376</pubmed>| Cases J.
- ↑ <pubmed>7823895</pubmed>
- ↑ <pubmed>20725587</pubmed>| German Medical Science
- ↑ <pubmed>23198195</pubmed>| Case Rep Obstet Gynecol.
- ↑ <pubmed>22110520</pubmed>| PMC3205779