User:Z3418779: Difference between revisions
| Line 192: | Line 192: | ||
The Development section is divided into four structural components, greatly increasing ease of understanding. The information presented in this section is highly informative, well referenced and images are used well with content. “File:Development of Kidney.jpg” seems an image was uploaded incorrectly, redo using same process for the rest of the images. Abnormalities are very detailed for the two completed parts, captioning of images good. Removal or completion of Horseshoe kidney is needed. Overall an informative and well-structured page, references have to properly integrated from the ureter and abnormalities sections, completion of historical findings section is also required. | The Development section is divided into four structural components, greatly increasing ease of understanding. The information presented in this section is highly informative, well referenced and images are used well with content. “File:Development of Kidney.jpg” seems an image was uploaded incorrectly, redo using same process for the rest of the images. Abnormalities are very detailed for the two completed parts, captioning of images good. Removal or completion of Horseshoe kidney is needed. Overall an informative and well-structured page, references have to properly integrated from the ureter and abnormalities sections, completion of historical findings section is also required. | ||
===Group 3 GIT=== | |||
Good introduction, initial description of fore/mid/hindgut with listing of respective structures gives the reader an anatomical starting point. Fetal development is presented in appropriate depth. There is no acknowledgement of embryonic origin, research or abnormalities. These sections should feature in the introduction to present all parts of the report in the intro. The three separate timelines defeat the purpose of a timeline. These should either be merged into a single large timeline and remain at their present location or moved to introduce the foregut/midget/hindgut sections later on. Recent findings has a single study which is covered in good detail though 2-3 more studies would allow the reader to further understand current GIT Research. | |||
In foregut section the dot-points used should match your subheadings. For example duodenum development is covered in the stomach section but is not mentioned in the subheading resulting in its development being hard to find without trawling through the text or “Ctrl-f”. Additionally you seemed to have missed out on pancreas development entirely. Foregut could also use some more images 2-3 would be suffice. Midgut development has great information, strong table, 8/8 drawings(captions required though). Inclusion of histological features gives viewer a microscopic perspective on development. Hindgut cloaca partitioning content is well worded though references are lacking. | |||
Anorectal deformities sections should be moved under the Deformities section. The type of dotpoint style used should be standardised. Too few abnormalities in the deformities section, though after the hindgut deformities are mover there should be sufficient. There are no references supporting the possible causes of Gastroschisis. The referencing it very good unlike other pages there are no random reference subheadings. In overview format wise quite attractive, information is adequately in-depth in all sections, introduction fails to address whole page, referencing is great for a draft (exceptions being “introduction” “Liver, Gallbladder and Bile Duct”), some captions aren’t present, abnormalities in development section should be moved into deformities/abnormalities section. | |||
Revision as of 17:08, 14 October 2014
Lab attendance
Lab 2 attended though didn't know we had to do attendance on our page
Lab 3 --Z3418779 --Z3418779 (talk) 11:36, 20 August 2014 (EST)
Lab 4 --Z3418779 --Z3418779 (talk) 11:39, 27 August 2014 (EST)
Lab 6 --Z3418779 (talk) 11:27, 10 September 2014 (EST)
Lab 7 --Z3418779 (talk) 11:56, 17 September 2014 (EST)
Lab 8 --Z3418779 (talk) 11:27, 24 September 2014 (EST)
Lab Task 1; Research Paper Summaries
Li M, Zhao H-C, Li R, Yu Y, Qiao J (2014) Chromosomal Aberrations in In-Vitro Matured Oocytes Influence Implantation and Ongoing Pregnancy Rates in a Mouse Model Undergoing Intracytoplasmic Sperm Injection. PLoS ONE 9(7): e103347. doi:10.1371/journal.pone.0103347
In-vitro fertilisation (IVF) and In-vitro maturation (IVM) are potential ways to alleviate issues with gonadotrophin stimulation. IVF has been accepted as the prefered Assisted Reproductive technique because of the higher success rate then IVM, which has 7 to 12% probablitly of plantation. Previous studies have concluded that the low success rate is related to the etiology of infertility rather then the technique itself. The selection of specific oocytes based on morphological features can greatly increase chance of implantation.
The study goal is to analyse spindle and chromosome and spindle configurations during the maturation process and resulting pre- and post-implantation embryos.
Experiment 1: used immature oocytes collected and matured in-vitro, with 3 cultures one at 18, 20 and 22 hours. alpha-tubulin and chromosome configurations were imaged by immunofluorescnce method. Experiment 2: used intracytoplasmic sperm injection to fertilise IVM oocytes, the pre-implanation phase was then compared to that of fertilised IVo oocytes. Expierement 3: Resulting embryos where introduced to a Pseudo-pregnant mouse, followed by dissection of fetuses on days 6.5 and 12.5.
Results; Spindle assembly in expiement 1 showed 18h had less that 50% originally, then rose to 52% in metaphase,the 20 and 22 hour grounds have significantly higher abnormalities (p<0.05) though had lower then a fresh control group. In expierment 2 1072 immature oocytes were collected and cultured with 924 becoming mature at MII stage, with 18h and 20h groups having reduced gene expression compared to 22h and control. Experiment 3 no significant difference in embryos on day 6.5, with 18h having slightly lower fetal rate then other groups. Day 12.5 showed a significantly reduced implantation rate in 18h group in comparison to control and 22 h groups. Full term development results average number of pups 18h=3, 20h=4.5, 22h =4.4, IVO=5.88
Shows greater chance of chromosome abnormalities in embryos from IVM timing and the relationship with post-implantation development in mouse models.
Shi W, Xu B, Wu L-M, Jin R-T, Luan H-B, et al. (2014) Oocytes with a Dark Zona Pellucida Demonstrate Lower Fertilization, Implantation and Clinical Pregnancy Rates in IVF/ICSI Cycles. PLoS ONE 9(2): e89409. doi:10.1371/journal.pone.0089409
Previous studies have shown abnormal morphology of oocytes and embryos results in lower viability for pre-implantation embryos and increase early pregnancy loss. This study focused on one specific oocyte abnormality a Dark Zona Pellucida (DZP)which previous studies have concluded to not significantly impact fertilization, embryo quality and pregnancy rate. Unlike previous studies DZP embryos would be seperated from NZP (Normal Zona Pellucida)
Patient population consisted of 268 infertile couples aged less than 38 years, being treated with IVRF or ICSI64 patients were put on embryo transfer cycles with occyte surronded by DZP being further subdivide based on percentage of Dark Zona pellucida; Group A(47) had 58% of Zona Pellucida dark on average and Group B(22) had entierly Dark Zona Pellucida. The remaining 204 patients made up the control group with NZP.
All patients were stimulated using a long pituitary down -regulation protocol. Oocytes were cultured in fertilisation medium. Sperm was used according to density gradient. Fertilized oocytes were placed in cleavage medium. Twenty mature oocytes (10 NZP, 10 DZP) were examined using JEOL-1230 Transmission Electron Microscope.
Reuslts; Miscarriages and live births for the three groups had no large differences. Though there were marked differences in fertilisation rate, frequency of high quality embryos, implantation rates and clinical pregnancy rates. All being lower Group B compared to control. Comparing the microscopic morphology shows no change in thickness of Zona Pellucida. NZP showed typical typical mitochondria shape; oval to spherical in shape with dense matrix and few cristae. DZP Mitochondria displayed swollen mitochondria encircling or containing vacuoles.
Study concluded that higher DZp results in decreased fertilisation rate, low rate of high quality embryos, adverse pregnancy outcomes and increased abnormal mitochondria and cytoplasmic vacuoles.
--Mark Hill These are relevant references and good summaries. You have not formatted the reference links correctly, see Help:Reference_Tutorial (4/5).
Lab Task 2; Image upload

Fetal Skeletal Muscle Progenitors [[1]]
Sakai H, Sato T, Sakurai H, Yamamoto T, Hanaoka K, et al. (2013) Fetal Skeletal Muscle Progenitors Have Regenerative Capacity after Intramuscular Engraftment in Dystrophin Deficient Mice. PLoS ONE 8(5): e63016. doi:10.1371/journal.pone.0063016
--Mark Hill Good image uploaded correctly. Reference link is not formatted. Help:Reference_Tutorial (4/5)
Lab Task 3
References
Julie R. Fuchs, Shinichi Terada, Didier Hannouche, Erin R. Ochoa, Joseph P. Vacanti, Dario O. Fauza.Engineered fetal cartilage: Structural and functional analysis in vitro. Journal of Pediatric Surgery Volume 37, Issue 12, Pages 1720–1725, December 2002
Sayer AA1, Cooper C.Fetal programming of body composition and musculoskeletal development.Early Hum Dev. 2005 Sep;81(9):735-44.
Baróti B1, Pap Z, Pánti Z, Buruian MM, Pávai Z. Morphometric and ultrasonographic study of the human fetal hip joint during intrauterine development. Rom J Morphol Embryol. 2013;54(4):977-81.
Liberty G1, Boldes R, Shen O, Shaul C, Cohen SM, Yagel S. The fetal larynx and pharynx: structure and development on two- and three-dimensional ultrasound. Ultrasound Obstet Gynecol. 2013 Aug;42(2):140-8. doi: 10.1002/uog.12358. Epub 2013 Jul 16.
--Mark Hill Three relevant references, link is not formatted correctly Help:Reference_Tutorial You should have included a sentence on why these articles were selected. (4/5)
Lab Task 4
Part 1
Identify a paper that uses cord stem cells therapeutically and write a brief (2-3 paragraph) description of the paper's findings.
Stem cell therapy and curcumin synergistically enhance recovery from spinal cord injury. [[2]]
Ormond DR, Shannon C, Oppenheim J, Zeman R, Das K, et al. (2014) Stem Cell Therapy and Curcumin Synergistically Enhance Recovery from Spinal Cord Injury. PLoS ONE 9(2): e88916. doi:10.1371/journal.pone.0088916
This paper investigates the result of Stem cell micro injection on spinal cord injury recovery and the effect curcumin(anti-inflammatory form turmeric) on Stem Cell Proliferation.
Findings; The addition of low concentrations of curcumin(500nM) results in a 180% increase in neurosphere proliferation,concentrations equal or higher then 1um fragements neurospheres and causes apotptosis. BBB Scores for Moderate SCI; Scores in week 5 and 6 showed a 33% higher score in treated rats compared to control. There was no significant difference between NSC and NSC/curcumin groups. BBB Scores for Severe SCI; After 2 weeks NSC and NSC/curcumin show similarly significant improvement compared to control, this improvement degrades in later weeks. Body weight all rats showed a decrease in weight then increase corresponding to recovery, except in Severe SCI in which curcumin alone showed improvement in week 5. Soleus Muscle Mass; in Moderate SCI showed no significant differentiation, in Severe SCI all treatemnt groups had higher mass then control particularly combination NSC/curcumin. Histopathological analysis;NSC and NSC/Curcumin displayed better recovery by comparing spared area to total area
Study displays Neural stem Cell therapy with curcumin is effective in recovery in Spinal cord injury. In the case of Moderate SCI effect of NSC and NSC/Curcumin showed a similarly significant recovery increase. In Severe SCI NSC/Curcumin had a greater aid in recovery. Curcumin assists recovery by reducing inflammation and gliosis, allowing unobstructed increased availability of neurotrophic factors from neural stem cells. The increased proliferation in-vitro supports the notion proliferative properties of curcumin.
Part 2
There are a number of developmental vascular "shunts" present in the embryo, that are closed postnatally. Identify these shunts and their anatomical location.
The Cardiovascular system has three important shunts present in the developing embryo, allowing blood to flow to differ from typical postnatal circulation. The key developmental shunts are Foramen Ovale,Ductus Venosus, Ductus Arteriosus.
Foramen Ovale; present in the Interatrial septum connecting the Left atrium and Right atrium. Allows oxygenated blood to bypass the lungs and enter the arterial network immediately. Usually open at birth, soon closed by two flaps of interatrial setum forming the fossa ovalis.
Ductus Venosus; connection of the umbilical vein and portal vein and inferior vena cava, purpose is to allow blood to bypass the liver. Functionally closes at birth and structurally closes within first week.
Ductus Arteriosus; connection of pulmonary artery and proximal ascending aorta, become ligamentum arteriosum after closure at birth
Lab Task 5
Anorectal Malformation
Anorectal Malformation is a defect of the anus and rectum which occurs during fetal development. There are multiple classifications of anorectal malformation based on the associated fistula. Low lesion;colon lies close to skin with an resulting in narrowing of the anus and rectum ending in blind pouch. High lesion; anus opens into bladder or genitalia, ,Persistent cloaca; rectum, vagina and urethra are joined into a single channel.
Causes; Abnormal development during weeks 7-10 as the lower section of intestinal tract forms. Originally the lower section large intestine and urinary tract are a single mass of cells. during the 7th-10th week this single mass of cells differentiates, seperate and form their appropriate organs. There is no correlation between activity of mother during pregnancy and incidence of malformation, more common in boys then girls.
Anorectal malformation occurs in 1 of 5,000 babies. Is associated with multiple other conditions and disorders these include; spinal , congenital, tracheal, esophageal, kidney, urinary and limb defects.
Lab Task 6
Identify and write a brief description of the findings of a recent research paper on development of one of the endocrine organs covered in today's practical.
Reciprocal epithelial: endothelial paracrine interactions during thyroid development govern follicular organization and C-cells differentiation
Study investigates how endothelial cells are recruited into the developing thyroid, and wether they control thyrocytes, C-cell differentiation and glandular organization. Thyroid explants were micro dissected from Vegfa-floxed and Pax8-cre mice embryos, then cultured in gelatin-coated dishes. Embryos were fixed and RNA probed for Vegfa and VEGF. Dissected thyroids were fixed in formaldehyde and some sections were immunofluorescence. Total RNA was extracted from embryonic thyroid lobes and underwent Real time polymerase chain reaction. Control and cKO lobes were rinsed and stained with uranyl acetate and examined under an electron microscope.
Results; Through out developmental stages of Endothelial cells closely surround thyroid epithelium; VEGFA knockout mice die around the period of childbirth, Reduction in vascular density hinders reorganization of epithelial mass into mono-layers because of polarization(shown by lack of basal pole). Additionally the thyroid developmental processes of bilobation, differentiation, polarization and vascularization are reproducible in a invivo culture, if adequate oxygen and nutrients are supplied
Findings; VEGFA is increased in a hypoxic environment via Hypoxia-induced factor-1 (HIF1A). When polarity normalizes decreases VEGFA expression. VEGFA derived from epithelium recruits the dense endothelial network in thyroid and promotes expansion. Endothelial cells are crucial for reorganization of follicular cells into follicles and differentiation of C-cells.
Continual interaction of epithelial and endothelial cells determines extent of thyroid development.
Hick, A., Delmarcelle, A., Bouquet, M., Klotz, S., Copetti, T., Forez, C., Van Der Smissen, P., Sonveaux, P., Collet, J., Feron, O. and others, (2013). Reciprocal epithelial: endothelial paracrine interactions during thyroid development govern follicular organization and C-cells differentiation. Developmental biology, 381(1), pp.227--240.
http://dev.biologists.org/content/early/2014/09/05/dev.110833.short
Identify the embryonic layers and tissues that contribute to the developing teeth.
Embryonic layers; Mesoderm, Ectoderm, neural crest ectomesenchyme all contribute to teeth development;
Ectoderm; contributes to Ameloblasts which later form tooth enamel
Neural crest mesenchyme; contributes to odontoblasts which undergoes dentinogenesis forming dentin
Mesoderm: forms blood supply of dental pulp
http://www.embryology.ch/anglais/sdigestive/gesicht05.html
Lab Task 8
Testis development
Indifferent development of gonads Originates from intermediate mesoderm forming genital ridges, pronephros appears with pronephric duct and nephrogenic mesenchyme, mesonephros appears with mesonephric tubule. Both later will fully or partially degenerate. Gonads descend down to pelvic region.
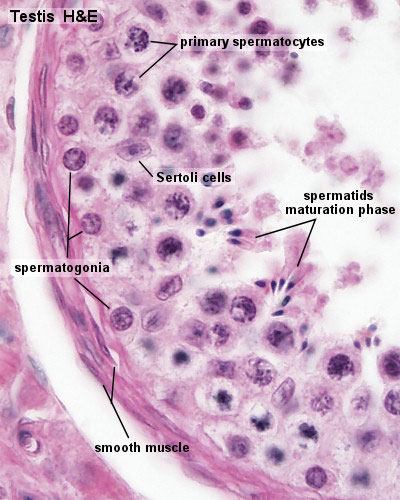
Gonadal differentiation Presence of Y chromsome has 48 protein-coding genes which begin the differentiation of the gonads into testes. In around week 6 Sertoli cells begin the appear in the primordia, to instruct germ cells; which have migrated through the primative streak. Leydig appear begin to secrete testosterone. The germ cells are enveloped in Sertoli cells which stop thier differentiation at T1 prospermatogonia until after birth.
In the testes the paramesoneph degenerates because of anti0Mullerian hormone secreted by the Sertoli cells. Mesonephric duct remains and under testosterone further differentiates to later form rete testis and ductus deferens. Testis cords of Sertoli and Germ Cells differentiate into semiferous tubules.

https://embryology.med.unsw.edu.au/embryology/images/d/d9/Seminiferous-tubule-HEx40.jpg External genitalia differentiation Indifferentiation stage in which cloaca is divided by proliferating mesencyme forming the urorectal septum. The presence of Dihydrotestosterone result in growth of genital tubercle and formation of genital folds. The folds are maintained then fuse creating perineal and penile raphe. Lateral to urethral folds is the labioscrotal swelling which later becomes the scrotum.
{kind=link}
Peer Reveiws
Group 1 Respiratory
The pages structure is quite well done, with appropriate use of heading. The introduction explains the general development of the respiratory system, differentiating embryonic, fetal and postnatal time-span. Like division of conducting and respiratory zones with strong general description of each zones components. The referencing of the first three heads content and images was not present though I presume this could be easily resolved. The Development stages table gives is very informative, particularly liked how the stages during the fetal period had more in-depth feature description then the embryonic and postnatal stages.
The Current research and findings section was in-depth with strong explanations and in-text referencing; only part lacking referencing is the Functional unit section. Some sentences should be broken up to avoid excessive use of commas “However, a study conducted…”. There seems to be a picture missing or placed incorrectly for one of the 2013 studies. The Lung Model picture is relevant but with no caption, though the description and referencing when clicking on the image is solid. Little improvement is needed for the Historical findings and Abnormalities sections, great referencing and content. Particularly impressed with the sheer amount of abnormalities presented, with information being sourced from 2-3 references for each abnormality.
To improve referencing needs to be added particularly to the introduction, conduction and respiratory zone. The references need to be collected at the bottom of the page instead of after every couple of sections. The removal of the multiple reference subheadings would make the content and page in general easier to navigate. Many of the earlier images should be captioned properly and referenced properly, with missing info like ((Template: Student Image)), description, copyright info. The content of Respiratory and Lung Development Stages could be slightly more in-depth though not too significant of an issue. Overall content is written well, providing information on all the important objectives, only place improvement is properly required is referencing and some formatting.
Group 2 Respiratory
Nice introduction addressing function of the system to set the tone, more detail in the development of components would be preferable. Abnormalities part of introduction has sufficient detail and referencing. The description of anatomical and histological structure described is mostly post-natal, more linking the structure to embryonic beginning and fetal continuation of development. Historic findings heading should be removed or expanded on, searching for articles before a certain period could be helpful. Introduction is easy to understand and presents the structure of the page exceptionally.
Developmental timeline is good at giving the reader a simple overview of renal development, putting it into a table would make it look more professional. The Current research model section gives readers much insight into the method developmental stages were discovered. I would recommend find additional 1-2 methods.
The Development section is divided into four structural components, greatly increasing ease of understanding. The information presented in this section is highly informative, well referenced and images are used well with content. “File:Development of Kidney.jpg” seems an image was uploaded incorrectly, redo using same process for the rest of the images. Abnormalities are very detailed for the two completed parts, captioning of images good. Removal or completion of Horseshoe kidney is needed. Overall an informative and well-structured page, references have to properly integrated from the ureter and abnormalities sections, completion of historical findings section is also required.
Group 3 GIT
Good introduction, initial description of fore/mid/hindgut with listing of respective structures gives the reader an anatomical starting point. Fetal development is presented in appropriate depth. There is no acknowledgement of embryonic origin, research or abnormalities. These sections should feature in the introduction to present all parts of the report in the intro. The three separate timelines defeat the purpose of a timeline. These should either be merged into a single large timeline and remain at their present location or moved to introduce the foregut/midget/hindgut sections later on. Recent findings has a single study which is covered in good detail though 2-3 more studies would allow the reader to further understand current GIT Research.
In foregut section the dot-points used should match your subheadings. For example duodenum development is covered in the stomach section but is not mentioned in the subheading resulting in its development being hard to find without trawling through the text or “Ctrl-f”. Additionally you seemed to have missed out on pancreas development entirely. Foregut could also use some more images 2-3 would be suffice. Midgut development has great information, strong table, 8/8 drawings(captions required though). Inclusion of histological features gives viewer a microscopic perspective on development. Hindgut cloaca partitioning content is well worded though references are lacking.
Anorectal deformities sections should be moved under the Deformities section. The type of dotpoint style used should be standardised. Too few abnormalities in the deformities section, though after the hindgut deformities are mover there should be sufficient. There are no references supporting the possible causes of Gastroschisis. The referencing it very good unlike other pages there are no random reference subheadings. In overview format wise quite attractive, information is adequately in-depth in all sections, introduction fails to address whole page, referencing is great for a draft (exceptions being “introduction” “Liver, Gallbladder and Bile Duct”), some captions aren’t present, abnormalities in development section should be moved into deformities/abnormalities section.